Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Nursing students' clinical experience at mental health facilityDocumento4 pagineNursing students' clinical experience at mental health facilityAdrian Dela CruzNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- AttestationDocumento1 paginaAttestationAdrian Dela CruzNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Reference: What Is Chronic Obstructive Pulmonary Disease? COPD FoundationDocumento4 pagineReference: What Is Chronic Obstructive Pulmonary Disease? COPD FoundationAdrian Dela CruzNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Woman With Asthma Exacerbation Discharged AMA Due To Care For Elderly MotherDocumento1 paginaWoman With Asthma Exacerbation Discharged AMA Due To Care For Elderly MotherDe Leon CjNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
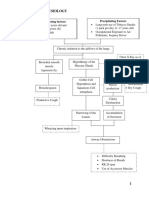
- Vi. Pathophysiology: Precipitating Factors Predisposing FactorsDocumento1 paginaVi. Pathophysiology: Precipitating Factors Predisposing FactorsAdrian Dela CruzNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Geno GrammDocumento1 paginaGeno GrammAdrian Dela CruzNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Table PlanDocumento5 pagineTable PlanAdrian Dela CruzNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Vii. Laboratory Results: Hemoglobin 129 MG/DL 140-160 MG/DL LowDocumento2 pagineVii. Laboratory Results: Hemoglobin 129 MG/DL 140-160 MG/DL LowAdrian Dela CruzNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- HamavhvDocumento7 pagineHamavhvAdrian Dela CruzNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- MMMMMMMMMMMDocumento4 pagineMMMMMMMMMMMAdrian Dela CruzNessuna valutazione finora
- Bibliography on Chronic Kidney Disease Symptoms and TreatmentsDocumento2 pagineBibliography on Chronic Kidney Disease Symptoms and TreatmentsAdrian Dela CruzNessuna valutazione finora
- Introduction NNDocumento6 pagineIntroduction NNAdrian Dela CruzNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- 0.3table of ContentsDocumento2 pagine0.3table of ContentsAdrian Dela CruzNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Chronic Kidney Failure Case Study LSPU College of NursingDocumento1 paginaChronic Kidney Failure Case Study LSPU College of NursingAdrian Dela CruzNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- QuestionDocumento1 paginaQuestionAdrian Dela CruzNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Comprehensive Exam NCM 145Documento17 pagineComprehensive Exam NCM 145Adrian Dela CruzNessuna valutazione finora
- Chronic Kidney Failure Case Study LSPU College of NursingDocumento1 paginaChronic Kidney Failure Case Study LSPU College of NursingAdrian Dela CruzNessuna valutazione finora
- Drug Used To Treat High Blood PressureDocumento4 pagineDrug Used To Treat High Blood PressureAdrianPaul Dela CruzNessuna valutazione finora
- Laguna State Polytechnic University: Group 2 Nutrition - Lab BSN - Ii A Ms. Ma. Janice M. BernardoDocumento5 pagineLaguna State Polytechnic University: Group 2 Nutrition - Lab BSN - Ii A Ms. Ma. Janice M. BernardoAdrian Dela CruzNessuna valutazione finora
- Drug Used To Treat High Blood PressureDocumento4 pagineDrug Used To Treat High Blood PressureAdrianPaul Dela CruzNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- To Work Peacefully For Political and Social ReformsDocumento2 pagineTo Work Peacefully For Political and Social ReformsAdrian Dela CruzNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Soil LiquefactionDocumento12 pagineSoil LiquefactionKikin Kikin PelukaNessuna valutazione finora
- Phenomenological of in Church and TV WorshipDocumento18 paginePhenomenological of in Church and TV WorshipCindy TirtaNessuna valutazione finora
- Maureen L. Walsh - Re-Imagining Redemption. Universal Salvation in The Theology of Julian of NorwichDocumento20 pagineMaureen L. Walsh - Re-Imagining Redemption. Universal Salvation in The Theology of Julian of NorwichAni LupascuNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- BCP-8000 User's ManualDocumento36 pagineBCP-8000 User's ManualAsad PatelNessuna valutazione finora
- Oecumenius’ Exegetical Method in His Commentary on the RevelationDocumento10 pagineOecumenius’ Exegetical Method in His Commentary on the RevelationMichał WojciechowskiNessuna valutazione finora
- SB Z Audio2Documento2 pagineSB Z Audio2api-151773256Nessuna valutazione finora
- Usjr Temfacil Balance of Work Schedule Aug 25, 2022Documento5 pagineUsjr Temfacil Balance of Work Schedule Aug 25, 2022Maribeth PalumarNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Chapter 10 AP GP PDFDocumento3 pagineChapter 10 AP GP PDFGeorge ChooNessuna valutazione finora
- Juan Martin Garcia System Dynamics ExercisesDocumento294 pagineJuan Martin Garcia System Dynamics ExercisesxumucleNessuna valutazione finora
- Concept Page - Using Vagrant On Your Personal Computer - Holberton Intranet PDFDocumento7 pagineConcept Page - Using Vagrant On Your Personal Computer - Holberton Intranet PDFJeffery James DoeNessuna valutazione finora
- Final Decision W - Cover Letter, 7-14-22Documento19 pagineFinal Decision W - Cover Letter, 7-14-22Helen BennettNessuna valutazione finora
- Caterpillar Ep15krtDocumento37 pagineCaterpillar Ep15krtIvan MajikNessuna valutazione finora
- F-16c.1 Ginkgo Ginkgolic AcidDocumento2 pagineF-16c.1 Ginkgo Ginkgolic AcidNarongchai PongpanNessuna valutazione finora
- Qualitative Research EssayDocumento9 pagineQualitative Research EssayMichael FoleyNessuna valutazione finora
- Lesson 2 Socio Anthropological View of The SelfDocumento12 pagineLesson 2 Socio Anthropological View of The SelfAilyn RamosNessuna valutazione finora
- VivsayamDocumento87 pagineVivsayamvalarumsakthi100% (2)
- Sto - Cristo Proper Integrated School 1 Grading Grade 9 Science Table of SpecializationDocumento2 pagineSto - Cristo Proper Integrated School 1 Grading Grade 9 Science Table of Specializationinah jessica valerianoNessuna valutazione finora
- House Designs, QHC, 1950Documento50 pagineHouse Designs, QHC, 1950House Histories100% (8)
- LTE EPC Technical OverviewDocumento320 pagineLTE EPC Technical OverviewCristian GuleiNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 2018-04-12 List Mold TVSDocumento5 pagine2018-04-12 List Mold TVSFerlyn ValentineNessuna valutazione finora
- Handout Tematik MukhidDocumento72 pagineHandout Tematik MukhidJaya ExpressNessuna valutazione finora
- Gotham City: A Study into the Darkness Reveals Dangers WithinDocumento13 pagineGotham City: A Study into the Darkness Reveals Dangers WithinajNessuna valutazione finora
- Proceedings of The 16 TH WLCDocumento640 pagineProceedings of The 16 TH WLCSabrinaNessuna valutazione finora
- Clausius TheoremDocumento3 pagineClausius TheoremNitish KumarNessuna valutazione finora
- CIRC 314-AN 178 INP EN EDENPROD 195309 v1Documento34 pagineCIRC 314-AN 178 INP EN EDENPROD 195309 v1xloriki_100% (1)
- Entrepreneurship Project On Jam, Jelly & PicklesDocumento24 pagineEntrepreneurship Project On Jam, Jelly & Picklesashish karshinkarNessuna valutazione finora
- Fake News Poems by Martin Ott Book PreviewDocumento21 pagineFake News Poems by Martin Ott Book PreviewBlazeVOX [books]Nessuna valutazione finora
- An Online ECG QRS Detection TechniqueDocumento6 pagineAn Online ECG QRS Detection TechniqueIDESNessuna valutazione finora
- Cyclograph User ManualDocumento15 pagineCyclograph User ManualPeter BateNessuna valutazione finora
- VA TearDownDocumento5 pagineVA TearDownfaj_larcfave5149Nessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 3.5 su 5 stelle3.5/5 (2)