Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- IMO Ship Waste Delivery Receipt Mepc - Circ - 645Documento1 paginaIMO Ship Waste Delivery Receipt Mepc - Circ - 645wisnukerNessuna valutazione finora
- Ficha Tecnica-Skyjack SJ3219 8mtDocumento2 pagineFicha Tecnica-Skyjack SJ3219 8mtLESLY MILENA MORENO CORALNessuna valutazione finora
- 1762 Ob8 PDFDocumento16 pagine1762 Ob8 PDFRodríguez EdwardNessuna valutazione finora
- Elements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesDocumento8 pagineElements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesSadman Shaid SaadNessuna valutazione finora
- Logic NotesDocumento19 pagineLogic NotesCielo PulmaNessuna valutazione finora
- Updated G10 Class Routine Effective From 12 January 2023Documento1 paginaUpdated G10 Class Routine Effective From 12 January 2023NiloyNessuna valutazione finora
- Someone Who Believes in YouDocumento1 paginaSomeone Who Believes in YouMANOLO C. LUCENECIONessuna valutazione finora
- Assignment 2 Unit 20 Fully Completed - ReviewedDocumento5 pagineAssignment 2 Unit 20 Fully Completed - Reviewedchris.orisawayiNessuna valutazione finora
- Lafarge Interior Building Solutions BrochureDocumento24 pagineLafarge Interior Building Solutions BrochuretwinpixtwinpixNessuna valutazione finora
- Innerwear Industry Pitch PresentationDocumento19 pagineInnerwear Industry Pitch PresentationRupeshKumarNessuna valutazione finora
- Cambridge IGCSE Paper 2Documento4 pagineCambridge IGCSE Paper 2irajooo epik zizterNessuna valutazione finora
- JC Series Jaw Crusher PDFDocumento8 pagineJC Series Jaw Crusher PDFgarrybieber100% (1)
- TM-8000 HD Manual PDFDocumento37 pagineTM-8000 HD Manual PDFRoxana BirtumNessuna valutazione finora
- Cisco 2500 Series RoutersDocumento16 pagineCisco 2500 Series RoutersJull Quintero DazaNessuna valutazione finora
- Lec 4 - 4th WeekDocumento40 pagineLec 4 - 4th Weekrajpoot aliNessuna valutazione finora
- Module-4 (PDFDrive)Documento67 pagineModule-4 (PDFDrive)Divya priya KNessuna valutazione finora
- Electric ScootorDocumento40 pagineElectric Scootor01fe19bme079Nessuna valutazione finora
- Determinants - DPP 01 (Of Lec 02) - Lakshya JEE 2.0 2024Documento3 pagineDeterminants - DPP 01 (Of Lec 02) - Lakshya JEE 2.0 2024Apurv ChitranshNessuna valutazione finora
- Catalogo Aesculap PDFDocumento16 pagineCatalogo Aesculap PDFHansNessuna valutazione finora
- 2015 Nos-Dcp National Oil Spill Disaster Contingency PlanDocumento62 pagine2015 Nos-Dcp National Oil Spill Disaster Contingency PlanVaishnavi Jayakumar100% (1)
- Ali Erdemir: Professional ExperienceDocumento3 pagineAli Erdemir: Professional ExperienceDunkMeNessuna valutazione finora
- Assignment 1Documento3 pagineAssignment 1farhang_tNessuna valutazione finora
- Math COT 3Documento18 pagineMath COT 3Icy Mae SenadosNessuna valutazione finora
- Surface TensionDocumento13 pagineSurface TensionElizebeth GNessuna valutazione finora
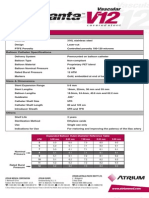
- Advanta V12 Data SheetDocumento2 pagineAdvanta V12 Data SheetJuliana MiyagiNessuna valutazione finora
- The FOA Reference For Fiber Optics - Fiber Optic TestingDocumento19 pagineThe FOA Reference For Fiber Optics - Fiber Optic TestingvsalaiselvamNessuna valutazione finora
- PEH Q3 Long QuizDocumento1 paginaPEH Q3 Long QuizBenedict LumagueNessuna valutazione finora
- Tugas Dikumpulkan Pada Hari Sabtu, 11 April 2020. Apabila Email Bermasalah Dapat Mengirimkan Via WA PribadiDocumento4 pagineTugas Dikumpulkan Pada Hari Sabtu, 11 April 2020. Apabila Email Bermasalah Dapat Mengirimkan Via WA PribadiFebry SugiantaraNessuna valutazione finora
- Health Promotion Throughout The Life Span 7th Edition Edelman Test BankDocumento35 pagineHealth Promotion Throughout The Life Span 7th Edition Edelman Test Bankcourtneyharrisbpfyrkateq100% (17)
- Dual Op Amp and Voltage Reference Ap4310/ADocumento12 pagineDual Op Amp and Voltage Reference Ap4310/AМихаил ЯненкоNessuna valutazione finora