Potrebbero piacerti anche
- Canadian: Hypoglycemia: Understanding The EnemyDocumento8 pagineCanadian: Hypoglycemia: Understanding The EnemyndistantiNessuna valutazione finora
- Colloidal Silvervs MonkeypoxDocumento20 pagineColloidal Silvervs MonkeypoxJed BatistaNessuna valutazione finora
- Multiple Choice QuestionsDocumento7 pagineMultiple Choice QuestionsDr-Sanjay SinghaniaNessuna valutazione finora
- CVA Nursing Lesson PlanDocumento6 pagineCVA Nursing Lesson Plansimonjosan60% (5)
- Diabetes Mellitus and Oral Health: An Interprofessional ApproachDa EverandDiabetes Mellitus and Oral Health: An Interprofessional ApproachNessuna valutazione finora
- Co 2019 Controle Glicemico IntDocumento8 pagineCo 2019 Controle Glicemico InthauhauNessuna valutazione finora
- Communicable Disease ReviewerDocumento18 pagineCommunicable Disease ReviewerMicah Jonah Elicaño100% (1)
- Assessment and Treatment of Hyperglycemia in Critically IllDocumento6 pagineAssessment and Treatment of Hyperglycemia in Critically IllYousif ElmasryNessuna valutazione finora
- Lesson Plan On Tuberculosis (Health Talk)Documento8 pagineLesson Plan On Tuberculosis (Health Talk)Priyanka Jangra100% (2)
- UKPDS Study Shows Benefits of Lowering Blood Glucose and Blood Pressure in Type 2 DiabetesDocumento5 pagineUKPDS Study Shows Benefits of Lowering Blood Glucose and Blood Pressure in Type 2 DiabetesAgustin MendezNessuna valutazione finora
- Br. J. Anaesth. 2011 Nicholson 65 73Documento9 pagineBr. J. Anaesth. 2011 Nicholson 65 73Adán 'OlveeraNessuna valutazione finora
- Diabetologia: UK Prospective Diabetes Study (UKPDS)Documento14 pagineDiabetologia: UK Prospective Diabetes Study (UKPDS)GuadalupeNessuna valutazione finora
- Hypoglycemia: Table 1Documento8 pagineHypoglycemia: Table 1erik1585Nessuna valutazione finora
- The UK Prospective Diabetes Study (UKPDS) : Clinical and Therapeutic Implications For Type 2 DiabetesDocumento6 pagineThe UK Prospective Diabetes Study (UKPDS) : Clinical and Therapeutic Implications For Type 2 DiabetesLaila KurniaNessuna valutazione finora
- Hypoglycemia - The Neglected ComplicationDocumento23 pagineHypoglycemia - The Neglected Complication4g5xwdvh9sNessuna valutazione finora
- Gudoy, Charies Jamille 12-WeierstrassDocumento4 pagineGudoy, Charies Jamille 12-WeierstrasschaNessuna valutazione finora
- Hypoglycemia: The Neglected Complication: Review ArticleDocumento16 pagineHypoglycemia: The Neglected Complication: Review Articlesiti nur aishah jalilNessuna valutazione finora
- Emerging Role of Dipeptidyl Peptidase-IV (DPP-4) Inhibitor Vildagliptin in The Management of Type 2 DiabetesDocumento9 pagineEmerging Role of Dipeptidyl Peptidase-IV (DPP-4) Inhibitor Vildagliptin in The Management of Type 2 DiabetesIndrasuari Anak Agung AyuNessuna valutazione finora
- Diabetes Control Reduces Cardiovascular RiskDocumento5 pagineDiabetes Control Reduces Cardiovascular RiskMahesh DmNessuna valutazione finora
- Trerapi Insulin Siip 2Documento10 pagineTrerapi Insulin Siip 2Indra YudaNessuna valutazione finora
- Editorial: Preventing Diabetic Retinopathy ProgressionDocumento3 pagineEditorial: Preventing Diabetic Retinopathy ProgressionRashellya RasyidaNessuna valutazione finora
- Cardiovascular Outcomes StudiesDocumento5 pagineCardiovascular Outcomes StudiesAnonymous LOeICSOqNessuna valutazione finora
- 349 FullDocumento3 pagine349 FullsenkonenNessuna valutazione finora
- Control GlicemicoDocumento20 pagineControl GlicemicomiguelalmenarezNessuna valutazione finora
- Metabolic Syndrome as a Predictor of DiabetesDocumento10 pagineMetabolic Syndrome as a Predictor of DiabetesChiranjeeviNessuna valutazione finora
- New Combination Treatments in The Management of Diabetes: Focus On Sitagliptin - MetforminDocumento10 pagineNew Combination Treatments in The Management of Diabetes: Focus On Sitagliptin - MetforminGd PadmawijayaNessuna valutazione finora
- Diabetes ManagementDocumento13 pagineDiabetes ManagementdanielmanuNessuna valutazione finora
- Polypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 DiabetesDocumento12 paginePolypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 Diabetesapi-311409998Nessuna valutazione finora
- ADVANCE: Action in Diabetes and Vascular Disease: Original ArticleDocumento6 pagineADVANCE: Action in Diabetes and Vascular Disease: Original ArticleMade LascanoNessuna valutazione finora
- A New Perspective On Metformin Therapy in Type 1 DiabetesDocumento7 pagineA New Perspective On Metformin Therapy in Type 1 DiabetesdeckardmaxNessuna valutazione finora
- Garber 2007Documento6 pagineGarber 2007Diana SamuezaNessuna valutazione finora
- PP Lancet 1998 Ukpds33Documento17 paginePP Lancet 1998 Ukpds33HelloNessuna valutazione finora
- ADO in BRCDocumento10 pagineADO in BRCVlahtNessuna valutazione finora
- Management of Diabetes Mellitus in Patients With Chronic Kidney DiseaseDocumento9 pagineManagement of Diabetes Mellitus in Patients With Chronic Kidney DiseasezakyNessuna valutazione finora
- tmpFF74 TMPDocumento2 paginetmpFF74 TMPFrontiersNessuna valutazione finora
- British Journal of Diabetes & Vascular Disease-2006-Pratley-150-6Documento8 pagineBritish Journal of Diabetes & Vascular Disease-2006-Pratley-150-6Nurul FajrinaNessuna valutazione finora
- Hypoglycemia, Diabetes, and Cardiovascular Events: C V. D, G B. B, V FDocumento6 pagineHypoglycemia, Diabetes, and Cardiovascular Events: C V. D, G B. B, V FHervi LaksariNessuna valutazione finora
- Hypoglycemia - 2014 Morales N DoronDocumento8 pagineHypoglycemia - 2014 Morales N DoronDian Eka RamadhaniNessuna valutazione finora
- Morales2014 PDFDocumento8 pagineMorales2014 PDFIneke IntaniaNessuna valutazione finora
- Jurnal Hipoglikemia PDFDocumento8 pagineJurnal Hipoglikemia PDFAyu Aprilita BastariNessuna valutazione finora
- Glycemic Control in Newly InsuDocumento17 pagineGlycemic Control in Newly Insucahyo wahyuNessuna valutazione finora
- Artigo Citado Dizendo Que Hiperglicemia Posprandial Sendo Um Preditor Melhor Qe Hemoglobina GlicadaDocumento7 pagineArtigo Citado Dizendo Que Hiperglicemia Posprandial Sendo Um Preditor Melhor Qe Hemoglobina GlicadabonelockNessuna valutazione finora
- Diagnosis and Treatment of Diabetic Nephropathy in Type 1 and Type 2 Diabetes Patients 2155 9929 1000295Documento4 pagineDiagnosis and Treatment of Diabetic Nephropathy in Type 1 and Type 2 Diabetes Patients 2155 9929 1000295Hening Tirta KusumawardaniNessuna valutazione finora
- Insulin resistance icuDocumento18 pagineInsulin resistance icuLucero GutierrezNessuna valutazione finora
- SGLT2 Inhibitors: The Future For Treatment of Type 2 Diabetes Mellitus and Other Chronic DiseasesDocumento6 pagineSGLT2 Inhibitors: The Future For Treatment of Type 2 Diabetes Mellitus and Other Chronic DiseasesLucian SiriteanuNessuna valutazione finora
- The Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainDocumento5 pagineThe Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainRyzka Izza MayFanyNessuna valutazione finora
- Perspectives in Diabetes: Postprandial Hyperglycemia and Diabetes ComplicationsDocumento7 paginePerspectives in Diabetes: Postprandial Hyperglycemia and Diabetes ComplicationsHania Asmarani RahmanitaNessuna valutazione finora
- Management of Blood GlucoseDocumento8 pagineManagement of Blood GlucoseerwanNessuna valutazione finora
- Ajhp 140168Documento12 pagineAjhp 140168cherrygems99Nessuna valutazione finora
- Update On Insulin Therapy For Type 2 DiabetesDocumento9 pagineUpdate On Insulin Therapy For Type 2 DiabetesRIKANessuna valutazione finora
- Definition and interpretation of remission in type 2 diabetes consensus reportDocumento8 pagineDefinition and interpretation of remission in type 2 diabetes consensus reportMaria Alejandra Quispe FloresNessuna valutazione finora
- DM in CKD Core Curriculum 2022Documento9 pagineDM in CKD Core Curriculum 2022Di KlauNessuna valutazione finora
- HbA1C Fluctuations Predict Diabetic NephropathyDocumento5 pagineHbA1C Fluctuations Predict Diabetic NephropathyDerison MarsinovaNessuna valutazione finora
- DeFronzo PDFDocumento23 pagineDeFronzo PDFMara HmNessuna valutazione finora
- Pharmacological Management of Type 2 Diabetes Mellitus: Rationale For Rational Use of InsulinDocumento9 paginePharmacological Management of Type 2 Diabetes Mellitus: Rationale For Rational Use of InsulinAditya Rachman Van Der ArjunaqueeNessuna valutazione finora
- Jurnal 1Documento17 pagineJurnal 1convenienceNessuna valutazione finora
- Intensification of Insulin Therapy in Patients With Type 2 Diabetes Mellitus An Algorithm For Basal Bolus TherapyDocumento12 pagineIntensification of Insulin Therapy in Patients With Type 2 Diabetes Mellitus An Algorithm For Basal Bolus TherapyYudi Fadilah100% (1)
- Heart Views-Cardio GlicemicDocumento24 pagineHeart Views-Cardio Glicemicsupit1Nessuna valutazione finora
- Obsgyn Referat FullDocumento3 pagineObsgyn Referat FullasdaadNessuna valutazione finora
- DerosaDocumento13 pagineDerosaAmeliana KamaludinNessuna valutazione finora
- Impact of Cardiovascular Outcomes On The Development and Approval of Medications For The Treatment of Diabetes MellitusDocumento11 pagineImpact of Cardiovascular Outcomes On The Development and Approval of Medications For The Treatment of Diabetes MellitusBayu Setyo NugrohoNessuna valutazione finora
- InsulinaDocumento8 pagineInsulinaClaudiu SufleaNessuna valutazione finora
- Standar Medical TreatmentDocumento17 pagineStandar Medical TreatmentIba SuprasabaNessuna valutazione finora
- UKPDSDocumento39 pagineUKPDSIsaac TellezNessuna valutazione finora
- MY NATURE CUREDocumento16 pagineMY NATURE CUREhemraj.koiralaNessuna valutazione finora
- Importance of Sputum Collection in Follow-Up in TBDocumento6 pagineImportance of Sputum Collection in Follow-Up in TBdradityagoreNessuna valutazione finora
- Case Study (2) - 115851Documento2 pagineCase Study (2) - 115851Qaisrani Y9Nessuna valutazione finora
- HEALTH 8: Communicable DiseaseDocumento31 pagineHEALTH 8: Communicable DiseaseElissah S PabilonaNessuna valutazione finora
- Cause of Lower Limb Edema and Hypoproteinemia DiagDocumento2 pagineCause of Lower Limb Edema and Hypoproteinemia DiagVictoria HNessuna valutazione finora
- MPH Curriculum KU NepalDocumento50 pagineMPH Curriculum KU Nepalpreeti A0% (1)
- Tulburari FunctionaleDocumento158 pagineTulburari Functionalelleticia87Nessuna valutazione finora
- Chronic Kidney Disease LIFA FixxxDocumento19 pagineChronic Kidney Disease LIFA FixxxMuzdalifa MohamadNessuna valutazione finora
- History of St. JudeDocumento3 pagineHistory of St. JudejeezNessuna valutazione finora
- Dengue: What Is Dengue Fever? What Is Dengue Hemorrhagic Fever?Documento9 pagineDengue: What Is Dengue Fever? What Is Dengue Hemorrhagic Fever?Abdul Shakur FaisalNessuna valutazione finora
- Sexually Transmitted Disesase.: Ralph Gabriel QuinalDocumento16 pagineSexually Transmitted Disesase.: Ralph Gabriel QuinalJohn Michael MonteflacoNessuna valutazione finora
- Nonspecific Low Back Pain: Clinical PracticeDocumento9 pagineNonspecific Low Back Pain: Clinical PracticeandhikahadiNessuna valutazione finora
- Daftar Pustaka Sistemic SclerosisDocumento2 pagineDaftar Pustaka Sistemic SclerosisSalwiyadiNessuna valutazione finora
- Hepatitis C PHD ThesisDocumento8 pagineHepatitis C PHD Thesisafkogftet100% (2)
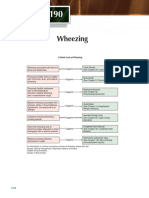
- Chapter 190: A Quick Guide to Wheezing CausesDocumento1 paginaChapter 190: A Quick Guide to Wheezing CausespelinNessuna valutazione finora
- Laboratory Report:: Shaynad Ambalathveettil SharafudheenDocumento1 paginaLaboratory Report:: Shaynad Ambalathveettil Sharafudheenshaynad binsharafNessuna valutazione finora
- La Union Arrival Card - V1 PDFDocumento2 pagineLa Union Arrival Card - V1 PDFLorei LeeNessuna valutazione finora
- Discussion - DM AssessmentDocumento1 paginaDiscussion - DM AssessmentSarah WhiteNessuna valutazione finora
- Severe - Acute - Respiratory - Syndrome - Coronavirus - 2 WikiDocumento30 pagineSevere - Acute - Respiratory - Syndrome - Coronavirus - 2 WikiUnggul YudhaNessuna valutazione finora
- Rare Disease Day Sample Fundraising LetterDocumento1 paginaRare Disease Day Sample Fundraising LetterKate GatesNessuna valutazione finora
- Disorders of The Upper Respiratory TractDocumento3 pagineDisorders of The Upper Respiratory TractJannelle Dela CruzNessuna valutazione finora
- Organism ID & Types of ShockDocumento5 pagineOrganism ID & Types of ShockAdrian BrillantesNessuna valutazione finora
- The Relationship Between Asthma and Allergic Rhinitis in The Iraqi PopulationDocumento7 pagineThe Relationship Between Asthma and Allergic Rhinitis in The Iraqi PopulationTasia DeastutiNessuna valutazione finora
- Takaful coverage for your lifestyle and legacyDocumento27 pagineTakaful coverage for your lifestyle and legacySubang Jaya Youth ClubNessuna valutazione finora
- Kesadaran Diri WPS Melakukan Pemeriksaan VCT Di Layanan Mobile VCT Rsud Raa Soewondo PatiDocumento15 pagineKesadaran Diri WPS Melakukan Pemeriksaan VCT Di Layanan Mobile VCT Rsud Raa Soewondo PatiMuhammad AntonNessuna valutazione finora
- New insights into treating mycoplasma without compromising egg qualityDocumento2 pagineNew insights into treating mycoplasma without compromising egg qualityDrivailaNessuna valutazione finora