Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
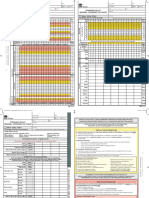
- SAGO AdultObsDocumento2 pagineSAGO AdultObsTim BrownNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- CBSE SyllabusDocumento22 pagineCBSE SyllabusMlivia Dcruze100% (1)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- EMT B Study Guid2Documento11 pagineEMT B Study Guid2varela86100% (1)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Maple Tree MenuDocumento6 pagineMaple Tree MenuSpencer FormanNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hpc3 - The Menu and Its CourseDocumento3 pagineHpc3 - The Menu and Its Coursemark danielNessuna valutazione finora
- The Lost HerdDocumento16 pagineThe Lost Herddarkdel100% (2)
- Personal IdentificationDocumento122 paginePersonal Identificationkarl luisNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- 7 Reading Task 1. For Questions 1-6, Read The Text Below and Decide Which Answer (A, B, C or D) Best Fits Each Gap. Fill in The Table Below The TextDocumento2 pagine7 Reading Task 1. For Questions 1-6, Read The Text Below and Decide Which Answer (A, B, C or D) Best Fits Each Gap. Fill in The Table Below The TextСофия ТимофееваNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- MethiorepDocumento4 pagineMethiorepprafulwonderfulNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Exercise Pamphlet PDFDocumento2 pagineExercise Pamphlet PDFBrittanyNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Brain Teasers 1Documento2 pagineBrain Teasers 1Starpiter80% (10)
- Global Perspectives PaperDocumento9 pagineGlobal Perspectives Paperapi-373229634Nessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- "Health Is Wealth" - A Short Moral Story: "Paid in Full With One Glass of MilkDocumento4 pagine"Health Is Wealth" - A Short Moral Story: "Paid in Full With One Glass of MilkkaloibestNessuna valutazione finora
- Labor and Delivery CMCC NotesDocumento12 pagineLabor and Delivery CMCC Notesrcestabillo6949100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Whats The SettingDocumento2 pagineWhats The Settingapi-2428046300% (2)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Reproduction Extra QuestionsDocumento10 pagineReproduction Extra Questionschayyakudopa9Nessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- 2022 - 2023 Sunrise Sunset Tables Entire YearDocumento2 pagine2022 - 2023 Sunrise Sunset Tables Entire YearmartsNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Evolution DPP 01Documento2 pagineEvolution DPP 01Naveen KumarJangirNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- My Little Donkey LetraDocumento2 pagineMy Little Donkey LetraGabriela HernándezNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Anatomy PDFDocumento114 pagineAnatomy PDFkhualabear101100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Dimensions of The DentureDocumento8 pagineDimensions of The DentureetequetaquiNessuna valutazione finora
- Master ChartDocumento3 pagineMaster Chartsudhir74Nessuna valutazione finora
- An Incident by Anton Pavlovich ChekhovDocumento5 pagineAn Incident by Anton Pavlovich Chekhovapi-19787590Nessuna valutazione finora
- TM2 - K37 - Eye Disorders Due To Tropical DiseasesDocumento86 pagineTM2 - K37 - Eye Disorders Due To Tropical DiseasesedelinNessuna valutazione finora
- Regulation of Cardiac Output and Venous Return by Dr. RoomiDocumento44 pagineRegulation of Cardiac Output and Venous Return by Dr. RoomiMudassar RoomiNessuna valutazione finora
- 150+ Art Careers - The Ultimate ListDocumento28 pagine150+ Art Careers - The Ultimate ListJaneNessuna valutazione finora
- Curriculum Guide: Magdev Major in Animal Production: Title and Description of Courses UnitsDocumento2 pagineCurriculum Guide: Magdev Major in Animal Production: Title and Description of Courses UnitsRomel gonzagaNessuna valutazione finora
- Една Кука Woollky Penguin Crochet Pattern by Babayaga EngDocumento4 pagineЕдна Кука Woollky Penguin Crochet Pattern by Babayaga EngDiana BozhilovaNessuna valutazione finora
- Imunologi DasarDocumento43 pagineImunologi Dasarmirza nuchalidaNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- For The Patient: Capecitabine Mriz Lei: Capecitabine (Kypswietwbin)Documento10 pagineFor The Patient: Capecitabine Mriz Lei: Capecitabine (Kypswietwbin)EmmaNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)