Potrebbero piacerti anche
- PARDIÑAS Geriatric Assessment ToolDocumento6 paginePARDIÑAS Geriatric Assessment ToolWyeth Earl Padar EndrianoNessuna valutazione finora
- Assessment-Checklist EyesDocumento2 pagineAssessment-Checklist EyesJL Rebese100% (2)
- The Nursing Process in Psychiatric/Mental Health NursingDocumento30 pagineThe Nursing Process in Psychiatric/Mental Health Nursingmp17570% (1)
- Gerontology - Geriatric Assesment FormDocumento4 pagineGerontology - Geriatric Assesment FormMakaeru100% (1)
- Name of Patient: Age: Sex: Ward/room: Diagnosis: Proposed Operation: Anesthesia: Anesthesiologist: SurgeonDocumento2 pagineName of Patient: Age: Sex: Ward/room: Diagnosis: Proposed Operation: Anesthesia: Anesthesiologist: SurgeonJan Federick Bantay100% (2)
- Attitude TherapyDocumento4 pagineAttitude TherapyEnzo DyNessuna valutazione finora
- General Nursing ResponsibilitiesDocumento3 pagineGeneral Nursing ResponsibilitiesK EV INNessuna valutazione finora
- Basic or InstrumentsDocumento21 pagineBasic or InstrumentsMabes100% (1)
- (26 29) Process Recording FormatDocumento4 pagine(26 29) Process Recording Formatpoleene de leonNessuna valutazione finora
- Geriatric AssessmentDocumento27 pagineGeriatric AssessmentNeil Philip MaturanNessuna valutazione finora
- Cardiac System AssessmentDocumento14 pagineCardiac System AssessmentValarmathi100% (1)
- Checklist of NursesDocumento1 paginaChecklist of NursesDhananjay Saini100% (4)
- Foot Care Procedure ChecklistDocumento3 pagineFoot Care Procedure ChecklistMarku LeeNessuna valutazione finora
- National Core Competency StandardsDocumento89 pagineNational Core Competency Standardsverna100% (1)
- Interview Guide For Nursing Health HistoryDocumento3 pagineInterview Guide For Nursing Health HistoryDersly LaneNessuna valutazione finora
- Clinical Evaluation Format and HEALTH TALK BSC JIMSHDocumento3 pagineClinical Evaluation Format and HEALTH TALK BSC JIMSHKiran Mini RaviNessuna valutazione finora
- Checklist - Medication AdministrationsDocumento37 pagineChecklist - Medication AdministrationsNichola Tappin100% (1)
- Duties and Responsibilities of Nurses in OtDocumento5 pagineDuties and Responsibilities of Nurses in Otvinnu kalyan100% (1)
- 05 N293 33108Documento23 pagine05 N293 33108Arjay G ParaniNessuna valutazione finora
- Mobility and Immobility: Group 1Documento46 pagineMobility and Immobility: Group 1Andrea Huecas Tria80% (5)
- Case Study - Balanced Skeletal TractionDocumento1 paginaCase Study - Balanced Skeletal Tractionzeverino castillo50% (2)
- 14 3 Performance Checklist - Medical AsepsisDocumento2 pagine14 3 Performance Checklist - Medical Asepsistwy113100% (2)
- Clinical Rotation Plan BSCDocumento10 pagineClinical Rotation Plan BSCBabita DhruwNessuna valutazione finora
- Cast, Brace, Traction CompilationDocumento13 pagineCast, Brace, Traction CompilationMar Ordanza100% (1)
- Bedside Clinics IVDocumento10 pagineBedside Clinics IVjothi100% (2)
- Pleural Effusion-Individual CPDocumento42 paginePleural Effusion-Individual CPKristine Mae Sugarol100% (1)
- Indent Verification of Labour RoomDocumento4 pagineIndent Verification of Labour RoomRajeshwariNessuna valutazione finora
- Colostomy Care ChecklistDocumento2 pagineColostomy Care ChecklistAlessandra Dominique MarianoNessuna valutazione finora
- Retracting and Exposing InstrumentsDocumento3 pagineRetracting and Exposing InstrumentsTherese Manalansan AlvarezNessuna valutazione finora
- Performance Checklist On Unoccupied Bed MakingDocumento2 paginePerformance Checklist On Unoccupied Bed MakingCes Aria88% (8)
- Final Case StudyDocumento35 pagineFinal Case StudyArvic Fritz CastañasNessuna valutazione finora
- Procedure On Lumber PunctureDocumento8 pagineProcedure On Lumber PunctureDimpal ChoudharyNessuna valutazione finora
- Staffing ComputationsDocumento24 pagineStaffing ComputationsOliric Acnab Nabcih100% (4)
- Geriatric History TakingDocumento27 pagineGeriatric History TakingPraise BechaydaNessuna valutazione finora
- The Legal Laws of Nursing Practice in The PhilippinesDocumento76 pagineThe Legal Laws of Nursing Practice in The PhilippinesTuTitNessuna valutazione finora
- Fundamental of NursingDocumento1 paginaFundamental of Nursingioana_ciobincanNessuna valutazione finora
- Lesson7 Geriatric AssessmentDocumento11 pagineLesson7 Geriatric AssessmentDennis Nabor Muñoz, RN,RMNessuna valutazione finora
- Apnmc Ta FormDocumento1 paginaApnmc Ta FormArunachala Vijay0% (1)
- ANA StandardsDocumento1 paginaANA Standardsointeriano100% (1)
- Surgical Question Paper 2021Documento21 pagineSurgical Question Paper 2021Winter Bear75% (4)
- Alcoholism Care PlanDocumento11 pagineAlcoholism Care Planilakkiya ilakkiyaNessuna valutazione finora
- Apgar ScoreDocumento22 pagineApgar ScoreBharat ThapaNessuna valutazione finora
- PE Essential Checklist For OSCE Part 1Documento3 paginePE Essential Checklist For OSCE Part 1Palwasha MalikNessuna valutazione finora
- Comprehensive Geriatric AssessmentDocumento12 pagineComprehensive Geriatric AssessmentNadja Jamilah100% (3)
- Use The Following Criteria in Evaluating The Skill PerformanceDocumento4 pagineUse The Following Criteria in Evaluating The Skill Performancekookie100% (1)
- Injections Lesson PlanDocumento6 pagineInjections Lesson Planapi-257582566100% (1)
- Physiological ChangesDocumento1 paginaPhysiological ChangesJilian McGuganNessuna valutazione finora
- Range of Motion Procedure Checklist-1Documento2 pagineRange of Motion Procedure Checklist-1api-288919673100% (2)
- 18-Checklist For Cardiovascular AssessmentDocumento2 pagine18-Checklist For Cardiovascular Assessmentgladz25100% (2)
- Medical 2021 Question Paper BSC NursingDocumento24 pagineMedical 2021 Question Paper BSC NursingWinter BearNessuna valutazione finora
- WALKING AIDS (Assistive Devices) : College of NursingDocumento15 pagineWALKING AIDS (Assistive Devices) : College of NursingJojo JustoNessuna valutazione finora
- MSN II 01.7.2020-OSCE in Instillation of Ear DropsDocumento3 pagineMSN II 01.7.2020-OSCE in Instillation of Ear DropsYAMINIPRIYANNessuna valutazione finora
- Updated Intake Packet 2020Documento21 pagineUpdated Intake Packet 2020Allison GomoNessuna valutazione finora
- Clinical Diagnostic AssessmentDocumento7 pagineClinical Diagnostic Assessmentjirehcounseling83% (6)
- Add and Adhd ResearchDocumento25 pagineAdd and Adhd Researchapi-520142437100% (1)
- Wellness Coach HandoutsDocumento6 pagineWellness Coach HandoutsKschleseNessuna valutazione finora
- Nursing Process and Mental Status Examination (MSE)Documento34 pagineNursing Process and Mental Status Examination (MSE)DUQUE DANA KATENessuna valutazione finora
- The Severe and Persistent Mental Illness Progress Notes PlannerDa EverandThe Severe and Persistent Mental Illness Progress Notes PlannerNessuna valutazione finora
- Behavioural DisordersDocumento18 pagineBehavioural DisordersAnsu MaliyakalNessuna valutazione finora
- Gordon's 11 Health Patterns With Corresponding Nursing DiagnosisDocumento3 pagineGordon's 11 Health Patterns With Corresponding Nursing DiagnosisAndy Swift100% (1)
- Installation Instructions INI Luma Gen2Documento21 pagineInstallation Instructions INI Luma Gen2John Kim CarandangNessuna valutazione finora
- Modern Construction HandbookDocumento498 pagineModern Construction HandbookRui Sousa100% (3)
- I. Choose The Best Option (From A, B, C or D) To Complete Each Sentence: (3.0pts)Documento5 pagineI. Choose The Best Option (From A, B, C or D) To Complete Each Sentence: (3.0pts)thmeiz.17sNessuna valutazione finora
- SM EFATEX Rev D2 3 1 2018 PDFDocumento20 pagineSM EFATEX Rev D2 3 1 2018 PDFGuilhermePlacidoNessuna valutazione finora
- Pearson R CorrelationDocumento2 paginePearson R CorrelationAira VillarinNessuna valutazione finora
- ChatGPT & EducationDocumento47 pagineChatGPT & EducationAn Lê Trường88% (8)
- Bone Surface MarkingsDocumento2 pagineBone Surface MarkingsNurul Afiqah Fattin AmatNessuna valutazione finora
- Problem Solving No. 123Documento5 pagineProblem Solving No. 123Christy Joy BarboNessuna valutazione finora
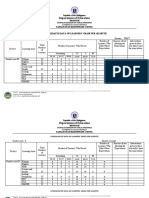
- Department of Education: Consolidated Data On Learners' Grade Per QuarterDocumento4 pagineDepartment of Education: Consolidated Data On Learners' Grade Per QuarterUsagi HamadaNessuna valutazione finora
- TM Mic Opmaint EngDocumento186 pagineTM Mic Opmaint Engkisedi2001100% (2)
- EPW, Vol.58, Issue No.44, 04 Nov 2023Documento66 pagineEPW, Vol.58, Issue No.44, 04 Nov 2023akashupscmadeeaseNessuna valutazione finora
- Does Adding Salt To Water Makes It Boil FasterDocumento1 paginaDoes Adding Salt To Water Makes It Boil Fasterfelixcouture2007Nessuna valutazione finora
- Electronic Diversity Visa ProgrambDocumento1 paginaElectronic Diversity Visa Programbsamkimari5Nessuna valutazione finora
- Stability Analysis of Geocell Reinforced Slopes by Considering Bending EffectDocumento13 pagineStability Analysis of Geocell Reinforced Slopes by Considering Bending EffectRakesh KapoorNessuna valutazione finora
- White Paper: 1 Definitive Guide To Data QualityDocumento18 pagineWhite Paper: 1 Definitive Guide To Data QualityGonçalo MartinsNessuna valutazione finora
- Ethernet/Ip Parallel Redundancy Protocol: Application TechniqueDocumento50 pagineEthernet/Ip Parallel Redundancy Protocol: Application Techniquegnazareth_Nessuna valutazione finora
- Halloween EssayDocumento2 pagineHalloween EssayJonathan LamNessuna valutazione finora
- Javascript Notes For ProfessionalsDocumento490 pagineJavascript Notes For ProfessionalsDragos Stefan NeaguNessuna valutazione finora
- BIOAVAILABILITY AND BIOEQUIVALANCE STUDIES Final - PPTX'Documento32 pagineBIOAVAILABILITY AND BIOEQUIVALANCE STUDIES Final - PPTX'Md TayfuzzamanNessuna valutazione finora
- English For Academic and Professional Purposes - ExamDocumento3 pagineEnglish For Academic and Professional Purposes - ExamEddie Padilla LugoNessuna valutazione finora
- Man Bni PNT XXX 105 Z015 I17 Dok 886160 03 000Documento36 pagineMan Bni PNT XXX 105 Z015 I17 Dok 886160 03 000Eozz JaorNessuna valutazione finora
- Ficha Técnica Panel Solar 590W LuxenDocumento2 pagineFicha Técnica Panel Solar 590W LuxenyolmarcfNessuna valutazione finora
- Anker Soundcore Mini, Super-Portable Bluetooth SpeakerDocumento4 pagineAnker Soundcore Mini, Super-Portable Bluetooth SpeakerM.SaadNessuna valutazione finora
- HRM Practices in NepalDocumento22 pagineHRM Practices in NepalBodhiNessuna valutazione finora
- PTW Site Instruction NewDocumento17 paginePTW Site Instruction NewAnonymous JtYvKt5XENessuna valutazione finora
- .CLP Delta - DVP-ES2 - EX2 - SS2 - SA2 - SX2 - SE&TP-Program - O - EN - 20130222 EDITADODocumento782 pagine.CLP Delta - DVP-ES2 - EX2 - SS2 - SA2 - SX2 - SE&TP-Program - O - EN - 20130222 EDITADOMarcelo JesusNessuna valutazione finora
- BDocumento28 pagineBLubaNessuna valutazione finora
- Jinivefsiti: Sultan LorisDocumento13 pagineJinivefsiti: Sultan LorisSITI HAJAR BINTI MOHD LATEPINessuna valutazione finora
- Jurnal Job DescriptionDocumento13 pagineJurnal Job DescriptionAji Mulia PrasNessuna valutazione finora
- The Pneumatics of Hero of AlexandriaDocumento5 pagineThe Pneumatics of Hero of Alexandriaapi-302781094Nessuna valutazione finora