Potrebbero piacerti anche
- The Little Black Book To Crushing STEP 1 V4.0 U PDFDocumento1.441 pagineThe Little Black Book To Crushing STEP 1 V4.0 U PDFAce Usmle91% (11)
- Metals in MedicineDocumento4 pagineMetals in MedicineSavi sharmaNessuna valutazione finora
- Heavy Metal Detox KlinghardftDocumento34 pagineHeavy Metal Detox KlinghardftAlice Lee100% (10)
- AP Practice Test Chapter 16-20Documento27 pagineAP Practice Test Chapter 16-20swagtothemax100% (1)
- 10 1016@j Jtemb 2019 05 003Documento6 pagine10 1016@j Jtemb 2019 05 003Lịch PhạmNessuna valutazione finora
- Toxicity of Metal Updated Lead, Mercury and AluminiumDocumento21 pagineToxicity of Metal Updated Lead, Mercury and AluminiumAshish ShresthaNessuna valutazione finora
- Estrés Oxidativo Inducido Por Metales y Enfermedades Humanas)Documento23 pagineEstrés Oxidativo Inducido Por Metales y Enfermedades Humanas)palomitadanceNessuna valutazione finora
- Applsci 10 04118 v2Documento16 pagineApplsci 10 04118 v2ancuta.lupaescuNessuna valutazione finora
- Metal Ions in Biological Systems PDFDocumento4 pagineMetal Ions in Biological Systems PDFVigyan PravahaNessuna valutazione finora
- The Effects of Heavy Metals On Human Metabolism: Toxicology Mechanisms and MethodsDocumento11 pagineThe Effects of Heavy Metals On Human Metabolism: Toxicology Mechanisms and MethodsTRINH HUỲNH NGỌC DIỄMNessuna valutazione finora
- سارة 3Documento4 pagineسارة 3Sara AbdoNessuna valutazione finora
- Heavy Metal Induced Oxidative Stress & Its Possible Reversal by Chelation TherapyDocumento23 pagineHeavy Metal Induced Oxidative Stress & Its Possible Reversal by Chelation TherapyArnab BiswasNessuna valutazione finora
- Review Article: Chelation: Harnessing and Enhancing Heavy Metal Detoxification-A ReviewDocumento14 pagineReview Article: Chelation: Harnessing and Enhancing Heavy Metal Detoxification-A ReviewaprilfitriaNessuna valutazione finora
- Molecules: Zinc Complexes With Nitrogen Donor Ligands As Anticancer AgentsDocumento41 pagineMolecules: Zinc Complexes With Nitrogen Donor Ligands As Anticancer AgentsDelhi VillanoNessuna valutazione finora
- Metallothionein: An Overview On Its Metal Homeostatic Regulation in MammalsDocumento6 pagineMetallothionein: An Overview On Its Metal Homeostatic Regulation in MammalsOmar ReynosoNessuna valutazione finora
- Final DocumentDocumento16 pagineFinal Documentreajon panditNessuna valutazione finora
- 2020 - Effects of Histidine Modification of Chitosan Microparticles On Metal Ion AdsorptionDocumento10 pagine2020 - Effects of Histidine Modification of Chitosan Microparticles On Metal Ion Adsorptionfreirethamyres0Nessuna valutazione finora
- Processes: Metal Ions, Metal Chelators and Metal Chelating Assay As Antioxidant MethodDocumento16 pagineProcesses: Metal Ions, Metal Chelators and Metal Chelating Assay As Antioxidant Methodwow tryNessuna valutazione finora
- Synthesis and Characterization of EDTA ComplexesDocumento7 pagineSynthesis and Characterization of EDTA ComplexesLucas PereiraNessuna valutazione finora
- BIC PartI VN PDFDocumento62 pagineBIC PartI VN PDFNguyễn Văn CườngNessuna valutazione finora
- 736-Article Text-10-1-10-20220223Documento10 pagine736-Article Text-10-1-10-20220223debapriya.ikrabNessuna valutazione finora
- Reviews: Antimicrobial Activity of Metals: Mechanisms, Molecular Targets and ApplicationsDocumento14 pagineReviews: Antimicrobial Activity of Metals: Mechanisms, Molecular Targets and ApplicationsChemist.AlchemistNessuna valutazione finora
- 7-21 Titanium SteinemannDocumento15 pagine7-21 Titanium SteinemannAntonio Vieira Ribeiro FilhoNessuna valutazione finora
- Sathya 2023 BP 18442D11Documento11 pagineSathya 2023 BP 18442D112019t00490Nessuna valutazione finora
- 2022 Biosensor For Heavy Metals Detection in Wastewater A Review Karthik VelusamyDocumento17 pagine2022 Biosensor For Heavy Metals Detection in Wastewater A Review Karthik VelusamyAngela Viviana Alzate GarciaNessuna valutazione finora
- Stox2211-6843446 015403Documento9 pagineStox2211-6843446 015403Obaiah JamakalaNessuna valutazione finora
- Zina Envtal Toxicology Assignment100-1%Documento30 pagineZina Envtal Toxicology Assignment100-1%Tesfahun TakeleNessuna valutazione finora
- GP Heavymetalstoxicityinanimals RJAVFS PDFDocumento8 pagineGP Heavymetalstoxicityinanimals RJAVFS PDFHuy VịtNessuna valutazione finora
- Novel Thiosemicarbazone Derivatives and TheirDocumento39 pagineNovel Thiosemicarbazone Derivatives and TheirAnis BouchamaNessuna valutazione finora
- Metal StressDocumento11 pagineMetal Stressವಿಶ್ವಾಸ್ ಗೌಡNessuna valutazione finora
- A Review On Silver-Mediated DNA Base Pairs Methodology and ApplicationDocumento17 pagineA Review On Silver-Mediated DNA Base Pairs Methodology and ApplicationIsabela DragomirNessuna valutazione finora
- Toxicology Reports: SciencedirectDocumento10 pagineToxicology Reports: SciencedirectafbmgNessuna valutazione finora
- RH Katsaros2002Documento12 pagineRH Katsaros2002Juanita Pulido TeutaNessuna valutazione finora
- Effects of Mixing Metal Ions On Oxidative DNA Damage Mediated by A Fenton-Type ReductionDocumento9 pagineEffects of Mixing Metal Ions On Oxidative DNA Damage Mediated by A Fenton-Type ReductionEko RaharjoNessuna valutazione finora
- Gold 3 e MS ReactivityDocumento14 pagineGold 3 e MS ReactivityLaísa BarséNessuna valutazione finora
- Synthesis, Characterization and Antimicrobial Properties of Mixed Ligand of Sulphamethoxazole and Trimethoprim and Their Manganese (II) and Copper (II) ComplexesDocumento6 pagineSynthesis, Characterization and Antimicrobial Properties of Mixed Ligand of Sulphamethoxazole and Trimethoprim and Their Manganese (II) and Copper (II) ComplexesInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- L4 Toxic Effects of Metals-UpdatedDocumento55 pagineL4 Toxic Effects of Metals-UpdatedAmr SewilamNessuna valutazione finora
- Heavy Metals and Living Systems An OverviewDocumento9 pagineHeavy Metals and Living Systems An OverviewZulfiqar AliNessuna valutazione finora
- Heavy Metals Causing Toxicity in Animals and Fishes: December 2014Documento8 pagineHeavy Metals Causing Toxicity in Animals and Fishes: December 2014Jonathan NoelNessuna valutazione finora
- Iron and Copper Metabolism: Miguel Arredondo, Marco T. Nu N EzDocumento15 pagineIron and Copper Metabolism: Miguel Arredondo, Marco T. Nu N EzkonyekNessuna valutazione finora
- A Review On Organic Colorimetric and Fluorescent Chemosensors For The Detection of ZN II IonsDocumento18 pagineA Review On Organic Colorimetric and Fluorescent Chemosensors For The Detection of ZN II Ionsbijoystudent481Nessuna valutazione finora
- Inorganica Chimica Acta: Research PaperDocumento7 pagineInorganica Chimica Acta: Research PaperSansanNessuna valutazione finora
- Highlights of Heavy Metals Molecular Toxicity Mechanisms, Exposure Dynamics, and Environmental PresenceDocumento12 pagineHighlights of Heavy Metals Molecular Toxicity Mechanisms, Exposure Dynamics, and Environmental PresenceKIU PUBLICATION AND EXTENSIONNessuna valutazione finora
- Analytical Methods For Estimation of Metals: Shah Jignesh, Khanvilkar Vineeta, Shirode Abhay and Kadam VilasraoDocumento18 pagineAnalytical Methods For Estimation of Metals: Shah Jignesh, Khanvilkar Vineeta, Shirode Abhay and Kadam VilasraoGRd JNessuna valutazione finora
- Gravimetric Coordinate For System PDFDocumento11 pagineGravimetric Coordinate For System PDFMuhammad SoraniNessuna valutazione finora
- Biogenic Metallic Elements in The Human Brain?Documento10 pagineBiogenic Metallic Elements in The Human Brain?jocollingwoodNessuna valutazione finora
- Chapter 1 Novel NanomaterialsDocumento47 pagineChapter 1 Novel Nanomaterialswjohn6182Nessuna valutazione finora
- Metal Chemistry Group WorkDocumento12 pagineMetal Chemistry Group WorkParis GreenNessuna valutazione finora
- Universiti Tenaga Nasional: Progress Report 1Documento18 pagineUniversiti Tenaga Nasional: Progress Report 1Tengku AsyrafNessuna valutazione finora
- Ghanghas 2021Documento29 pagineGhanghas 2021Lionel TchanaNessuna valutazione finora
- Rangabhashiyam 2018Documento70 pagineRangabhashiyam 2018dineshkumar HICET STAFF CHEMICALNessuna valutazione finora
- 2009 - Altas - Inhibitory Effect of Heavy Metals On Methane-Producing AnaerobicDocumento6 pagine2009 - Altas - Inhibitory Effect of Heavy Metals On Methane-Producing AnaerobicJulio ReyesNessuna valutazione finora
- Antioxidants 12 00243 v2 1Documento28 pagineAntioxidants 12 00243 v2 1quimicosorioNessuna valutazione finora
- Heavy Metals Causing Toxicity in Animals and Fishes: February 2014Documento8 pagineHeavy Metals Causing Toxicity in Animals and Fishes: February 2014Mahad QaziNessuna valutazione finora
- Molecular Mechanism and Targets of The Antimicrobial Activity of Metal NanoparticlesDocumento6 pagineMolecular Mechanism and Targets of The Antimicrobial Activity of Metal NanoparticlesRodolfo Angulo OlaisNessuna valutazione finora
- Article Biosorbentes ImportanciadeColumna OKDocumento25 pagineArticle Biosorbentes ImportanciadeColumna OKAnonymous NSbxWMNessuna valutazione finora
- Cap 5Documento20 pagineCap 5Erick Contreras PeláezNessuna valutazione finora
- Assignment JuelDocumento5 pagineAssignment JuelShoaib AhmedNessuna valutazione finora
- Tchou N Wou 2012Documento32 pagineTchou N Wou 2012haneen radNessuna valutazione finora
- Dennehy Et Al. 2022Documento8 pagineDennehy Et Al. 2022Eleonora Freire EspeletaNessuna valutazione finora
- Mechanism of Action and Applications of The Antimicrobial Properties of CopperDocumento12 pagineMechanism of Action and Applications of The Antimicrobial Properties of CopperAninditaTrikusumaNessuna valutazione finora
- GPS RobotDocumento2 pagineGPS RobotAditya VermaNessuna valutazione finora
- RANDOMIZATIONDocumento13 pagineRANDOMIZATIONAditya VermaNessuna valutazione finora
- I Hereby Declare That This Assignment Is My Individual Work and I Have Not Copied It From Any Source. Shahwar HasanDocumento8 pagineI Hereby Declare That This Assignment Is My Individual Work and I Have Not Copied It From Any Source. Shahwar HasanAditya VermaNessuna valutazione finora
- How Stuff WorlsDocumento24 pagineHow Stuff WorlsAditya VermaNessuna valutazione finora
- Physics Term Paper by Aditya RajDocumento11 paginePhysics Term Paper by Aditya RajAditya VermaNessuna valutazione finora
- METALLODRUGSDocumento21 pagineMETALLODRUGSAditya Verma100% (1)
- Devendra Pratap SinghDocumento3 pagineDevendra Pratap SinghAditya VermaNessuna valutazione finora
- Biochem Lec Midterm TransesDocumento17 pagineBiochem Lec Midterm Transescathryna gaylanNessuna valutazione finora
- Topic 2.7 Transcriptin and TranslationDocumento7 pagineTopic 2.7 Transcriptin and TranslationSakina İmanovaNessuna valutazione finora
- Orca Share Media1662355444548 6972424090491517852Documento9 pagineOrca Share Media1662355444548 6972424090491517852Mic Houston Mar T. ParroNessuna valutazione finora
- Post It Note Science DNA Replication, Transcription and Translation Mini.1.Kreitzer-houslerDocumento4 paginePost It Note Science DNA Replication, Transcription and Translation Mini.1.Kreitzer-houslerCHRISTEROP0% (1)
- Techno-1.3-The Molecular Basis of HeredityDocumento30 pagineTechno-1.3-The Molecular Basis of HeredityMark DeGrootteNessuna valutazione finora
- Medical Microbiolog1Documento226 pagineMedical Microbiolog1gardenya100% (5)
- Central DogmaDocumento28 pagineCentral DogmaBryant Villarin BaldivicioNessuna valutazione finora
- Movie Links Molecular Biology of The CellDocumento18 pagineMovie Links Molecular Biology of The CellmotabsbviniNessuna valutazione finora
- DNA StructureDocumento4 pagineDNA StructuregabriellemichelleNessuna valutazione finora
- TOPIC 8: Teaching Plan 8C.1 Producing Recombinant DNADocumento17 pagineTOPIC 8: Teaching Plan 8C.1 Producing Recombinant DNAsalmaNessuna valutazione finora
- TOPIC 6.1 - 6.2 - DNA Structure and Replication, Student Learning GuideDocumento4 pagineTOPIC 6.1 - 6.2 - DNA Structure and Replication, Student Learning GuideL ChanNessuna valutazione finora
- Molecular Basis of InheritanceDocumento52 pagineMolecular Basis of InheritancezoologyNessuna valutazione finora
- Nucleic Acid Written ReportDocumento28 pagineNucleic Acid Written ReportCatnikimco100% (1)
- Exam Molecular BiologyDocumento6 pagineExam Molecular BiologyLân Lu100% (2)
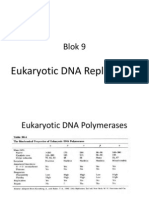
- Eukaryotic DNA Replication Blok9Documento15 pagineEukaryotic DNA Replication Blok9'Alivia Nabdakh ClocheNessuna valutazione finora
- Chapter-6 Molecular Basis of InheritanceDocumento17 pagineChapter-6 Molecular Basis of Inheritanceshodhan shettyNessuna valutazione finora
- Gene Expression 1Documento14 pagineGene Expression 1John LazaroNessuna valutazione finora
- BioK DP Notes 2.7Documento18 pagineBioK DP Notes 2.7Lal ÖzşahinNessuna valutazione finora
- MCQDocumento9 pagineMCQpkm7929Nessuna valutazione finora
- BCHN+213 2023 T2memoDocumento5 pagineBCHN+213 2023 T2memowhoeversaidthis1Nessuna valutazione finora
- NSEB Question Paper 2017Documento28 pagineNSEB Question Paper 2017Ashutosh100% (1)
- Candy Dna and Replication Lab StudentDocumento2 pagineCandy Dna and Replication Lab Studentapi-253533661Nessuna valutazione finora
- HSC Biology Module 5Documento21 pagineHSC Biology Module 5adneeniqbal259Nessuna valutazione finora
- FA - BiochemistryDocumento62 pagineFA - BiochemistryMargaret GraceNessuna valutazione finora
- Mod 6 Day2-Dna ReplicationDocumento17 pagineMod 6 Day2-Dna Replicationapi-293001217Nessuna valutazione finora
- Microbiology Principles and Explorations 10th Edition Black Test BankDocumento38 pagineMicrobiology Principles and Explorations 10th Edition Black Test Bankcharles90br100% (15)
- MCB 110 Study GuideDocumento10 pagineMCB 110 Study GuideAlexPowersNessuna valutazione finora
- Biology Passing Material KAYAKA PU COLLEGE KALABURAGIDocumento23 pagineBiology Passing Material KAYAKA PU COLLEGE KALABURAGIRAJAGOPAL93% (15)