Potrebbero piacerti anche
- 311 Topotecan Monotherapy 5 DayDocumento4 pagine311 Topotecan Monotherapy 5 DayRuxandra BănicăNessuna valutazione finora
- Heparin Dose Adjustment in The Prescence of Renal ImpairmentDocumento5 pagineHeparin Dose Adjustment in The Prescence of Renal ImpairmentRPR KSVNessuna valutazione finora
- Enoxaparin Info SheetDocumento7 pagineEnoxaparin Info SheetjafarkassimNessuna valutazione finora
- Aminoglycoside & VancomycinDocumento10 pagineAminoglycoside & VancomycinKhor Chin PooNessuna valutazione finora
- Nursing ResponsibilitiesDocumento4 pagineNursing ResponsibilitiesMaureen Joy Cascayan EspirituNessuna valutazione finora
- Antibiotik For Renal FailureDocumento6 pagineAntibiotik For Renal FailureWidhy Joss BangetzNessuna valutazione finora
- Teicoplanin Dosing and Monitoring in AdultsDocumento3 pagineTeicoplanin Dosing and Monitoring in Adultsdps_1976Nessuna valutazione finora
- Targocid Article 30 Referral Annex III - enDocumento32 pagineTargocid Article 30 Referral Annex III - enDR JAMAL WARISNessuna valutazione finora
- CHLVPP (Hodgkin'S Lymphoma) : (Max: 10Mg) (Max: 10Mg)Documento3 pagineCHLVPP (Hodgkin'S Lymphoma) : (Max: 10Mg) (Max: 10Mg)Sindu SankarNessuna valutazione finora
- Leukemia Treatment Regimens 7937Documento3 pagineLeukemia Treatment Regimens 7937Irfan FathurrahmanNessuna valutazione finora
- NICU Drugs GuideDocumento49 pagineNICU Drugs GuideArhanNessuna valutazione finora
- Vancomycin: Group 5 R.M 2Documento31 pagineVancomycin: Group 5 R.M 2vi_wiviaNessuna valutazione finora
- Ovarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorDocumento5 pagineOvarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorAnonymous g1hIPZNessuna valutazione finora
- Chemotherapy Protocol: RegimenDocumento6 pagineChemotherapy Protocol: RegimenAlexandra AndronescuNessuna valutazione finora
- Beacopp Hem HL ADocumento8 pagineBeacopp Hem HL AAnonymous 9dVZCnTXSNessuna valutazione finora
- Id 397 TeicoplaninDocumento2 pagineId 397 TeicoplaninStacey WoodsNessuna valutazione finora
- Intravenous Vancomycin Use in Adults - 2017Documento4 pagineIntravenous Vancomycin Use in Adults - 2017Angy KarakostaNessuna valutazione finora
- Capecitabine 14 DayDocumento6 pagineCapecitabine 14 DaybrystyyNessuna valutazione finora
- Enoxaparin - Prescribing, Administration and MonitoringDocumento6 pagineEnoxaparin - Prescribing, Administration and MonitoringFaheem AlsabriaNessuna valutazione finora
- ALIPIT Midterm Exam April 8,2020Documento1 paginaALIPIT Midterm Exam April 8,2020Jude Micko Bunyi AlipitNessuna valutazione finora
- UKMi-Gentamicin InfoDocumento4 pagineUKMi-Gentamicin InfoAmisha VastaniNessuna valutazione finora
- Vancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., PharmDocumento78 pagineVancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., Pharmkharbosham100% (1)
- L 51 R Hypercvad R MaDocumento7 pagineL 51 R Hypercvad R MaMohamed MahmoudNessuna valutazione finora
- Class Indications: GentamicinDocumento3 pagineClass Indications: GentamicinBer Anne Jaropojop TahilNessuna valutazione finora
- Clinical Guideline For Vancomycin Prescribing and Therapeutic Drug MonitoringDocumento11 pagineClinical Guideline For Vancomycin Prescribing and Therapeutic Drug MonitoringFate ChanNessuna valutazione finora
- 1.13 Hyper-CVAD-MA Version 2.1Documento5 pagine1.13 Hyper-CVAD-MA Version 2.1Alina CrissNessuna valutazione finora
- Pharmacokinetic Training Packet For PharmacistsDocumento24 paginePharmacokinetic Training Packet For PharmacistsGlory Claudia KarundengNessuna valutazione finora
- Neratinib Adjuvant Treatment Breast Cancer Protocol V1.1Documento6 pagineNeratinib Adjuvant Treatment Breast Cancer Protocol V1.1smokkerNessuna valutazione finora
- Medication Fact Sheets: 3rd Edition ContributorsDocumento50 pagineMedication Fact Sheets: 3rd Edition ContributorsIndumathi ThangathirupathiNessuna valutazione finora
- Aida Protocol For Apl: InductionDocumento4 pagineAida Protocol For Apl: InductionGabrielNessuna valutazione finora
- Bone and Joint Infections BNHFT 2010 PDFDocumento3 pagineBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriNessuna valutazione finora
- CetuximabDocumento8 pagineCetuximabcrespo2816100% (1)
- Therapeutic Drug Monitoring and Pharmacokinetics of Intravenous Vancomycin For Pharmacists and Other Healthcare ProfessionalsDocumento3 pagineTherapeutic Drug Monitoring and Pharmacokinetics of Intravenous Vancomycin For Pharmacists and Other Healthcare Professionalsminhmap90_635122804Nessuna valutazione finora
- Accofil Epar Product Information enDocumento155 pagineAccofil Epar Product Information endora192424Nessuna valutazione finora
- Tuberculosis Treatment GuidelinesDocumento2 pagineTuberculosis Treatment GuidelinesMaverick CaoileNessuna valutazione finora
- ABVDDocumento3 pagineABVDEsther WanguiNessuna valutazione finora
- Azithromycin Monograph - PaediatricDocumento7 pagineAzithromycin Monograph - PaediatrictynNessuna valutazione finora
- K25. Malaria Pada AnakDocumento39 pagineK25. Malaria Pada AnakayapillaiNessuna valutazione finora
- Merck Manual: Professional VersionDocumento25 pagineMerck Manual: Professional VersionDwina Wiranti PutriNessuna valutazione finora
- Cilastati Imipenem Drug InfoDocumento19 pagineCilastati Imipenem Drug InfoCosmina GeorgianaNessuna valutazione finora
- Effect DoseDocumento30 pagineEffect DoseXyprus Darina VeloriaNessuna valutazione finora
- GentamiciniDocumento11 pagineGentamiciniBenjie SisonNessuna valutazione finora
- Revision 1Documento21 pagineRevision 1NaifmxNessuna valutazione finora
- Teicoplanin Prescribing and Therapeutic Drug Monitoring Clinical Guideline V2.0 March 2019Documento12 pagineTeicoplanin Prescribing and Therapeutic Drug Monitoring Clinical Guideline V2.0 March 2019nancy voraNessuna valutazione finora
- Kanamycin (Mode of Administration)Documento3 pagineKanamycin (Mode of Administration)Waseem MaroofiNessuna valutazione finora
- Aminogycoside AntibioticsDocumento31 pagineAminogycoside AntibioticsNurul Febrina100% (2)
- Ribociclib Protocol CRP13 B034 v1.0Documento4 pagineRibociclib Protocol CRP13 B034 v1.0Joana JohnNessuna valutazione finora
- L 44 Bendamustine 70 R CLLDocumento7 pagineL 44 Bendamustine 70 R CLLsatishNessuna valutazione finora
- ClarithromycinDocumento4 pagineClarithromycinGAYATHIRINessuna valutazione finora
- Final Anti TB in SP - SituationDocumento50 pagineFinal Anti TB in SP - SituationAbdul JalilNessuna valutazione finora
- Drug Use in Renal and Hepatic Disorders.: Chapter-VDocumento30 pagineDrug Use in Renal and Hepatic Disorders.: Chapter-VBandameedi RamuNessuna valutazione finora
- BendamustineDocumento2 pagineBendamustineagusjatNessuna valutazione finora
- Castration-Recurrent Prostate Cancer First-Line Therapy: No Visceral MetastasesDocumento2 pagineCastration-Recurrent Prostate Cancer First-Line Therapy: No Visceral Metastasesalberto cabelloNessuna valutazione finora
- New Zealand Data Sheet: 1. Product NameDocumento15 pagineNew Zealand Data Sheet: 1. Product NameMhd IjlalNessuna valutazione finora
- DurhamDocumento6 pagineDurhamAdrianus NyomanNessuna valutazione finora
- Therapeutic Drug MonitoringDocumento10 pagineTherapeutic Drug MonitoringAnnie SethiNessuna valutazione finora
- Management of Reactions in Leprosy: How Should Lepra Reactions Be Managed?Documento2 pagineManagement of Reactions in Leprosy: How Should Lepra Reactions Be Managed?Echa AdityaNessuna valutazione finora
- How To RecoverDocumento3 pagineHow To RecoverSterr LiingNessuna valutazione finora
- This Is For The Most Amazing Woman I've Ever MetDocumento1 paginaThis Is For The Most Amazing Woman I've Ever MetKenRodulfReyesVillaruelNessuna valutazione finora
- Learning ContractDocumento1 paginaLearning ContractKenRodulfReyesVillaruelNessuna valutazione finora
- European SurgeryDocumento1 paginaEuropean SurgeryKenRodulfReyesVillaruelNessuna valutazione finora
- Guidelines For Completing Application Form For Personal ID / Access CardDocumento1 paginaGuidelines For Completing Application Form For Personal ID / Access CardKenRodulfReyesVillaruelNessuna valutazione finora
- The Heartstart Course hsc38d0318Documento19 pagineThe Heartstart Course hsc38d0318KenRodulfReyesVillaruelNessuna valutazione finora
- New Login Page and InterfaceDocumento2 pagineNew Login Page and InterfaceKenRodulfReyesVillaruelNessuna valutazione finora
- Labs Final NaDocumento5 pagineLabs Final NaKenRodulfReyesVillaruelNessuna valutazione finora
- Using The Glasgow Coma Scale For Patient AssessmentDocumento7 pagineUsing The Glasgow Coma Scale For Patient AssessmentJasmin Dela TorreNessuna valutazione finora
- OSCE Assessments Candidate Briefing - 1Documento4 pagineOSCE Assessments Candidate Briefing - 1KenRodulfReyesVillaruelNessuna valutazione finora
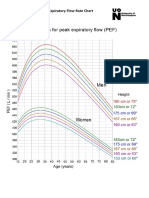
- Peak Expiratory Flow Rate Chart - 3Documento1 paginaPeak Expiratory Flow Rate Chart - 3KenRodulfReyesVillaruelNessuna valutazione finora
- Cambridge: Ad Astra 04/10/2019 10:15 Am 01 X Inf 4.50 G-10 Screen 2Documento1 paginaCambridge: Ad Astra 04/10/2019 10:15 Am 01 X Inf 4.50 G-10 Screen 2KenRodulfReyesVillaruelNessuna valutazione finora
- Grade 6 Grading System NewDocumento344 pagineGrade 6 Grading System NewKenRodulfReyesVillaruelNessuna valutazione finora
- Casay National High School: KnowledgeDocumento2 pagineCasay National High School: KnowledgeKenRodulfReyesVillaruelNessuna valutazione finora
- Inflammatory & Immunology DisorderDocumento15 pagineInflammatory & Immunology DisorderRachelle Sarmiento GarciaNessuna valutazione finora
- k12 Grading Systelsam Sample1Documento1 paginak12 Grading Systelsam Sample1KenRodulfReyesVillaruelNessuna valutazione finora
- Grade Sheet 9Documento4 pagineGrade Sheet 9KenRodulfReyesVillaruelNessuna valutazione finora
- Torrent Downloaded From Demonoid - PHDocumento1 paginaTorrent Downloaded From Demonoid - PHRossella GiglioNessuna valutazione finora
- k12 Grading Systelsam Sample1Documento1 paginak12 Grading Systelsam Sample1KenRodulfReyesVillaruelNessuna valutazione finora
- Grade 9 GRADING SHEET TEMPLATEDocumento4 pagineGrade 9 GRADING SHEET TEMPLATEPrince Yahwe RodriguezNessuna valutazione finora
- k12 Grading Systelsam Sample1Documento1 paginak12 Grading Systelsam Sample1KenRodulfReyesVillaruelNessuna valutazione finora
- Summary of RatingDocumento1 paginaSummary of Ratingalvarez9654Nessuna valutazione finora
- Chlorpromazine Drug StudyDocumento3 pagineChlorpromazine Drug StudyEmJay Balansag100% (5)
- Pembagian Barang BPJS So Des 2019 Kfa MdoDocumento56 paginePembagian Barang BPJS So Des 2019 Kfa Mdokf ttrNessuna valutazione finora
- OralMeds - ChecklistDocumento6 pagineOralMeds - ChecklistXandra BasnilloNessuna valutazione finora
- Maximum Recommended Local Anaesthetic Doses For AdultsDocumento2 pagineMaximum Recommended Local Anaesthetic Doses For AdultsadithardanaNessuna valutazione finora
- 1 Pharmacy Practice Therapeutics OTC Drugs Q&A Content Ver1Documento123 pagine1 Pharmacy Practice Therapeutics OTC Drugs Q&A Content Ver1bhaveshnidhi64100% (1)
- Lindi HaksaDocumento5 pagineLindi HaksaLANCAR FOTOCOPYNessuna valutazione finora
- Analisis Waktu Tunggu Pelayanan Resep Rawat Jalan Di Instalasi Farmasi Rumah Sakit Bhayangkara ManadoDocumento7 pagineAnalisis Waktu Tunggu Pelayanan Resep Rawat Jalan Di Instalasi Farmasi Rumah Sakit Bhayangkara Manadodewi weny sariNessuna valutazione finora
- 03) Harga Program 13 Maret 2021-DikonversiDocumento5 pagine03) Harga Program 13 Maret 2021-DikonversiRahmawati FarmacyNessuna valutazione finora
- Experiment 8 Analgesic and Anti-Inflammatory WorksheetDocumento17 pagineExperiment 8 Analgesic and Anti-Inflammatory WorksheetJANNIE BELLE RODRIGUEZNessuna valutazione finora
- ASpectrumof Psychoactive Drugsin AyurvedaDocumento5 pagineASpectrumof Psychoactive Drugsin AyurvedaUPINDERJIT SINGHNessuna valutazione finora
- PharmacologyDocumento68 paginePharmacologyvansal liu80% (5)
- Drug Use During Pregnancy and LactationDocumento42 pagineDrug Use During Pregnancy and LactationMisbahuddin MohammadNessuna valutazione finora
- Cefuroxime, Levofloxacin, Esomeprazole, and Bismuth As First-Line Therapy For Eradicating Helicobacter Pylori in Patients Allergic To PenicillinDocumento9 pagineCefuroxime, Levofloxacin, Esomeprazole, and Bismuth As First-Line Therapy For Eradicating Helicobacter Pylori in Patients Allergic To PenicillinjerryNessuna valutazione finora
- Desensitization ADULT PDFDocumento28 pagineDesensitization ADULT PDFAnonymous 9dVZCnTXSNessuna valutazione finora
- Biosaar Product CardDocumento4 pagineBiosaar Product CardRakesh RockzzNessuna valutazione finora
- Topical Finasteride in The Treatment of Androgenic Alopecia. Preliminary Evaluations After A 16-Month Therapy CourseDocumento4 pagineTopical Finasteride in The Treatment of Androgenic Alopecia. Preliminary Evaluations After A 16-Month Therapy Coursenobody100% (2)
- Risk ManagmentDocumento5 pagineRisk ManagmentRhodora Benipayo100% (3)
- Babesia & Anaplasmosis TreatmentDocumento2 pagineBabesia & Anaplasmosis TreatmentUkya Ching MogNessuna valutazione finora
- D CalDocumento2 pagineD CalShay MNessuna valutazione finora
- DDD 1Documento17 pagineDDD 1Verqueza OdzongNessuna valutazione finora
- Ekatalog 2023 Sulsel RajawaliDocumento50 pagineEkatalog 2023 Sulsel RajawaliSafria HamzaNessuna valutazione finora
- Diagnosis Banding DepresiDocumento9 pagineDiagnosis Banding DepresiHarton MuhammadNessuna valutazione finora
- MCQ PharmacokineticsDocumento10 pagineMCQ PharmacokineticsHarshit Sharma100% (1)
- Autacoids (Local Hormones) and Their Pharmacolo-Gical ModulationDocumento75 pagineAutacoids (Local Hormones) and Their Pharmacolo-Gical ModulationAgung PutraNessuna valutazione finora
- Clinical Medications WorksheetsDocumento2 pagineClinical Medications WorksheetsMichael Kuzbyt0% (1)
- Guidance Format Risk Management Plan RMP Eu Integrated Format Rev 201 enDocumento51 pagineGuidance Format Risk Management Plan RMP Eu Integrated Format Rev 201 enJavierFlórezRNessuna valutazione finora
- Evolution in The Practice of Pharmacy - Not A Revolution!Documento2 pagineEvolution in The Practice of Pharmacy - Not A Revolution!Ana Sofia MartinsNessuna valutazione finora
- NafarinDocumento2 pagineNafarinianecunar100% (2)
- Org MedDocumento11 pagineOrg MedTsukishima KeiNessuna valutazione finora
- Dokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedDocumento54 pagineDokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedMahmoud FathyNessuna valutazione finora