Potrebbero piacerti anche
- Neurological DisordersDocumento6 pagineNeurological DisordersSoojung Nam100% (3)
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicDa EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicValutazione: 5 su 5 stelle5/5 (1)
- Hypoxic Ischemic Encephalopathy (Hie) : AlgorithmDocumento11 pagineHypoxic Ischemic Encephalopathy (Hie) : AlgorithmAndreiMunteanuNessuna valutazione finora
- Seizures and The Epilepsies in Infants, Children, and AdolescentsDocumento8 pagineSeizures and The Epilepsies in Infants, Children, and AdolescentsCecille Ann CayetanoNessuna valutazione finora
- Phtls 9th Edition Prep Packets 2019aDocumento19 paginePhtls 9th Edition Prep Packets 2019ajuan4401100% (2)
- Acute Stroke Management by Carlos L Chua PDFDocumento61 pagineAcute Stroke Management by Carlos L Chua PDFHynne Jhea EchavezNessuna valutazione finora
- Chapter 13: Schizophrenia and Other Psychotic Disorders: Multiple ChoiceDocumento24 pagineChapter 13: Schizophrenia and Other Psychotic Disorders: Multiple ChoicesnowyznNessuna valutazione finora
- Internship ReportDocumento16 pagineInternship ReportRACHANA MURALIDHAR 1833279Nessuna valutazione finora
- Febrile Seizures, Febrile Seizure Plus, First Unprovoked Seizure WebinarDocumento45 pagineFebrile Seizures, Febrile Seizure Plus, First Unprovoked Seizure WebinarTun Paksi Sareharto100% (1)
- EEG Chapter 10 - Epileptiform Normal Variant (NIF)Documento27 pagineEEG Chapter 10 - Epileptiform Normal Variant (NIF)Yossy CatarinaNessuna valutazione finora
- 2.e.case Ctudy On BPADDocumento9 pagine2.e.case Ctudy On BPADManisa Parida100% (1)
- A Child With An Epileptic Status With Growth FalteringDocumento25 pagineA Child With An Epileptic Status With Growth FalteringHasan HusienNessuna valutazione finora
- First Seizure-RCEMDocumento2 pagineFirst Seizure-RCEMalsadiqbr5Nessuna valutazione finora
- Febrile SeizuresDocumento1 paginaFebrile SeizuresDiana AlexandraNessuna valutazione finora
- Pediatric Neurology Referral Guidelines: Table of ContentsDocumento10 paginePediatric Neurology Referral Guidelines: Table of ContentsEvannelson WardhanaNessuna valutazione finora
- Ihm - Febril SeizureDocumento1 paginaIhm - Febril SeizureEmmy 1432Nessuna valutazione finora
- Truspected Stroke AlgorithmDocumento4 pagineTruspected Stroke Algorithmtri wahyunoNessuna valutazione finora
- Seizure Disorders: Nursing ManagementDocumento3 pagineSeizure Disorders: Nursing ManagementDarren Mae MosadaNessuna valutazione finora
- Evangelista Pagola Case StudyDocumento21 pagineEvangelista Pagola Case StudyMikes CastroNessuna valutazione finora
- Febrile Seizures 12 - 1 - 2019 3Documento12 pagineFebrile Seizures 12 - 1 - 2019 3ninta karinaNessuna valutazione finora
- Febrile Seizures PathwayDocumento10 pagineFebrile Seizures PathwayFerry Abu Irsyad AtthaillahNessuna valutazione finora
- Ver Tigo A ND Dizziness in The Emergenc y Depar TmentDocumento12 pagineVer Tigo A ND Dizziness in The Emergenc y Depar TmentEko SaputraNessuna valutazione finora
- Hayats ResponsesDocumento18 pagineHayats Responsesyacineone01Nessuna valutazione finora
- EpilepsiaDocumento37 pagineEpilepsiaGrigore AlexandraNessuna valutazione finora
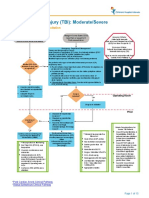
- Traumatic Brain Injury Moderate Severe Clinical PathwayDocumento15 pagineTraumatic Brain Injury Moderate Severe Clinical PathwayDobrila SimonovicNessuna valutazione finora
- High Risk Mild Head InjuryDocumento1 paginaHigh Risk Mild Head InjuryMay JPNessuna valutazione finora
- Seizure New Onset Clinical PathwayDocumento17 pagineSeizure New Onset Clinical PathwayKim Shyen BontuyanNessuna valutazione finora
- Citicoline Drug StudyDocumento2 pagineCiticoline Drug StudyJC LumayaNessuna valutazione finora
- ED Adult NICE Final 1107Documento2 pagineED Adult NICE Final 1107Guillermo Calderaro0% (1)
- Benign Febrile Seizure: PediatricsDocumento2 pagineBenign Febrile Seizure: PediatricsKrista P. AguinaldoNessuna valutazione finora
- Bacterial MeningitisDocumento2 pagineBacterial Meningitisjennielunay00Nessuna valutazione finora
- F Seizures AssessDocumento1 paginaF Seizures Assessmahmudajannatul.7Nessuna valutazione finora
- COP Week 4Documento32 pagineCOP Week 4hasti.khaledyanNessuna valutazione finora
- BCCA AB in Febrile Neutropenia GuidelinesDocumento2 pagineBCCA AB in Febrile Neutropenia GuidelinesAlvy SyukrieNessuna valutazione finora
- 3B2 Preceptorial Nov 18 SFSeizuresDocumento79 pagine3B2 Preceptorial Nov 18 SFSeizuresAbigail PaasaNessuna valutazione finora
- 2017 Stroke in Childhood - Pathway PosterDocumento1 pagina2017 Stroke in Childhood - Pathway PosterDeomicah SolanoNessuna valutazione finora
- Pediatric SeizuresDocumento64 paginePediatric SeizuresShobithaNessuna valutazione finora
- When Should Brain Imaging Precede Lumbar Puncture in Cases of Suspected Bacterial MeningitisDocumento3 pagineWhen Should Brain Imaging Precede Lumbar Puncture in Cases of Suspected Bacterial Meningitistsiko111Nessuna valutazione finora
- 18.d SeizuresDocumento6 pagine18.d SeizuresSamantha LuiNessuna valutazione finora
- Febrile Convulsions Clinical Guideline V4.0 February 2020Documento10 pagineFebrile Convulsions Clinical Guideline V4.0 February 2020AzmiNessuna valutazione finora
- EpilepsyDocumento38 pagineEpilepsyB AuNessuna valutazione finora
- Principles of Seizure ManagementDocumento119 paginePrinciples of Seizure ManagementRenan Toledo SandaloNessuna valutazione finora
- Endo 5Documento1 paginaEndo 5Bea YmsnNessuna valutazione finora
- Materi I DR HadryastutiDocumento38 pagineMateri I DR HadryastutiyuliNessuna valutazione finora
- Hydrocephalus Clinical Pathway: James L. PatigayonDocumento6 pagineHydrocephalus Clinical Pathway: James L. PatigayonJayson OlileNessuna valutazione finora
- Head Injury: Closed Head Injury EG: Falls, Motor Vehicle Crashes, Bicycle InjuriesDocumento13 pagineHead Injury: Closed Head Injury EG: Falls, Motor Vehicle Crashes, Bicycle InjuriesJudy HandlyNessuna valutazione finora
- Farmakoterapi I: EpilepsiDocumento83 pagineFarmakoterapi I: EpilepsisafiraNessuna valutazione finora
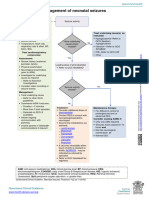
- Neonatal SeizuresDocumento33 pagineNeonatal SeizuresNursulfia MaharaniNessuna valutazione finora
- Battisti Nnconvulsions enDocumento130 pagineBattisti Nnconvulsions enangelinaNessuna valutazione finora
- Dr. I Gusti Ngurah Suwarba, Sp.A (K) Dr. Dewi Sutriani M, Sp.ADocumento28 pagineDr. I Gusti Ngurah Suwarba, Sp.A (K) Dr. Dewi Sutriani M, Sp.ASheryl ElitaNessuna valutazione finora
- Neo SeizureDocumento27 pagineNeo SeizureAchyut KanungoNessuna valutazione finora
- Guillian Barre Astra ZenecaDocumento6 pagineGuillian Barre Astra ZenecaGerardo de Gyves AvilaNessuna valutazione finora
- PREDICTALGORITHM v1 1 29.01.21Documento2 paginePREDICTALGORITHM v1 1 29.01.21selvi zhafirahNessuna valutazione finora
- Concept Map Meningitis TheoryDocumento3 pagineConcept Map Meningitis TheoryMia AuliaNessuna valutazione finora
- Concept Map Meningitis TheoryDocumento3 pagineConcept Map Meningitis TheoryMia AuliaNessuna valutazione finora
- Hepatitis B VaccineDocumento4 pagineHepatitis B VaccineShantal AbelloNessuna valutazione finora
- Neonatal SeizuresDocumento4 pagineNeonatal SeizuresSerag EdeenNessuna valutazione finora
- Etable 1. Encephalitis Diagnostic Criteria From Selected Published StudiesDocumento4 pagineEtable 1. Encephalitis Diagnostic Criteria From Selected Published StudiesNadine N'dilimabakaNessuna valutazione finora
- Finals - MCN RLEDocumento6 pagineFinals - MCN RLEKorean GirlNessuna valutazione finora
- Convulsive Disorders: Presenters: Kabwe Chanda EliasDocumento30 pagineConvulsive Disorders: Presenters: Kabwe Chanda EliasHomeground entertainmentNessuna valutazione finora
- Pediatric EpilepsyDocumento1 paginaPediatric EpilepsyRangel AngelNessuna valutazione finora
- 1538 Exam 5 IntracranialDocumento31 pagine1538 Exam 5 IntracranialJade EdanoNessuna valutazione finora
- MIni CaseSTUDY pediaWARDDocumento10 pagineMIni CaseSTUDY pediaWARDDANIELLA MALARANG MELNessuna valutazione finora
- NRN 202 Concept Map Patho-Altered Mental StatusDocumento1 paginaNRN 202 Concept Map Patho-Altered Mental StatusWendy Gilbert50% (2)
- AAN2023 PedsNCC Case1 Compositeslides 4.13Documento14 pagineAAN2023 PedsNCC Case1 Compositeslides 4.13Evelina ȘabanovNessuna valutazione finora
- The Effects of Dehydration On Brain Volume - Preliminary ResultsDocumento6 pagineThe Effects of Dehydration On Brain Volume - Preliminary ResultsCharina Geofhany DeboraNessuna valutazione finora
- 922 FullDocumento7 pagine922 FullCharina Geofhany DeboraNessuna valutazione finora
- Comparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile Seizures PDFDocumento5 pagineComparison of The Effects of Clobazam and Diazepam in Prevention of Recurrent Febrile Seizures PDFCharina Geofhany DeboraNessuna valutazione finora
- Acute Surgical Abdomen: An Unusual Presentation of Pulmonary EmbolusDocumento4 pagineAcute Surgical Abdomen: An Unusual Presentation of Pulmonary EmbolusCharina Geofhany DeboraNessuna valutazione finora
- Acute Cerebral Infarction Masked by A Brain Tumor: Kwo-Whei Lee Chung-Ping LoDocumento6 pagineAcute Cerebral Infarction Masked by A Brain Tumor: Kwo-Whei Lee Chung-Ping LoCharina Geofhany DeboraNessuna valutazione finora
- Meng Mammogram JulDocumento4 pagineMeng Mammogram JulLivia MillNessuna valutazione finora
- Electrical InjuriesDocumento1 paginaElectrical InjuriesIkhwan SalamNessuna valutazione finora
- Powerpoint On HemophiliaDocumento26 paginePowerpoint On HemophiliaTheo Sanson100% (1)
- Common Classifications of Aphasia PDFDocumento1 paginaCommon Classifications of Aphasia PDFAhmad HasanNessuna valutazione finora
- 10 Jenis Penyakit Tertinggi THN 2021Documento3 pagine10 Jenis Penyakit Tertinggi THN 2021yusuf dikaNessuna valutazione finora
- Cauda Equina SyndromeDocumento5 pagineCauda Equina SyndromeEdward XiamNessuna valutazione finora
- Edu Adhd PaperDocumento8 pagineEdu Adhd Paperapi-534406008Nessuna valutazione finora
- Theresa ncp-7Documento3 pagineTheresa ncp-7Jovel CortezNessuna valutazione finora
- Unit 4 Substance Induced Psychotic Disorder: StructureDocumento17 pagineUnit 4 Substance Induced Psychotic Disorder: StructureSachin RaturiNessuna valutazione finora
- OBE - Syllabus - Psych 109 Abnormal PsychologyDocumento15 pagineOBE - Syllabus - Psych 109 Abnormal PsychologySharrah Laine AlivioNessuna valutazione finora
- Womac Hip Score (WHS) : Pain Severity (On Average) During The Past MonthDocumento3 pagineWomac Hip Score (WHS) : Pain Severity (On Average) During The Past MonthPetru CarajaNessuna valutazione finora
- 3-Anxiety DisordersDocumento57 pagine3-Anxiety DisordersVidya BalaNessuna valutazione finora
- P2 Lec Latest QsDocumento17 pagineP2 Lec Latest QsGesta, Van Gerard T.Nessuna valutazione finora
- Mediclear: Site Office - 90, Vasant Complex, Mayur Vihar, DelhiDocumento3 pagineMediclear: Site Office - 90, Vasant Complex, Mayur Vihar, Delhiafsarkhan85Nessuna valutazione finora
- Presentation of Hirschsprung's DiseaseDocumento2 paginePresentation of Hirschsprung's DiseaseMarcela Di VincenzoNessuna valutazione finora
- Plabable Gems Endocrine PDF P7aDocumento44 paginePlabable Gems Endocrine PDF P7aayşenur sevinçNessuna valutazione finora
- Cereves Asq EngDocumento2 pagineCereves Asq EngMariana ZglavociNessuna valutazione finora
- Syncope: Global Cerebral Blood FlowDocumento7 pagineSyncope: Global Cerebral Blood FlowChananNessuna valutazione finora
- Neuroscience and Biobehavioral ReviewsDocumento10 pagineNeuroscience and Biobehavioral ReviewsBotez MartaNessuna valutazione finora
- QuizzesDocumento6 pagineQuizzesJafinNessuna valutazione finora
- Conduct DisorderDocumento5 pagineConduct Disordertri ummiNessuna valutazione finora
- Portfolio Output No. 13: Research On Anxiety Disorder/DepressionDocumento7 paginePortfolio Output No. 13: Research On Anxiety Disorder/DepressionAnnikah Trizya FACTONessuna valutazione finora
- 2000605-2 FOC 18 4s Critique FinalDocumento65 pagine2000605-2 FOC 18 4s Critique FinalAna ZahariaNessuna valutazione finora
- Patient X - Acute PancreatitisDocumento22 paginePatient X - Acute PancreatitisKen TokkNessuna valutazione finora
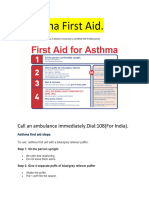
- Asthama First Aid.Documento3 pagineAsthama First Aid.Manoj KumarNessuna valutazione finora