Potrebbero piacerti anche
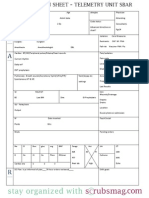
- Nurse Brain Sheet Telemetry Unit SBARDocumento1 paginaNurse Brain Sheet Telemetry Unit SBARvsosa624Nessuna valutazione finora
- Clinical Research Nursing: Scope and Standards of PracticeDa EverandClinical Research Nursing: Scope and Standards of PracticeValutazione: 5 su 5 stelle5/5 (1)
- Nursing and Patient Safety in The Operating RoomDocumento10 pagineNursing and Patient Safety in The Operating RoomJoe AbelloNessuna valutazione finora
- Steelman, Graling - 2013 - Top 10 Patient Safety Issues What More Can We DoDocumento23 pagineSteelman, Graling - 2013 - Top 10 Patient Safety Issues What More Can We DoElNessuna valutazione finora
- Medication ErrorDocumento37 pagineMedication ErrorJitendra PanthiNessuna valutazione finora
- Ebook Interpersonal Relationships - Professional Communication Skills For Canadian Nurses PDF Full Chapter PDFDocumento67 pagineEbook Interpersonal Relationships - Professional Communication Skills For Canadian Nurses PDF Full Chapter PDFconnie.lee826100% (30)
- Pediatric Case 9: Charlie Snow (Core) : Guided Reflection QuestionsDocumento3 paginePediatric Case 9: Charlie Snow (Core) : Guided Reflection QuestionsDai NguyenNessuna valutazione finora
- Alexanders Care Patient Surgery 16th Rothrock Test BankDocumento10 pagineAlexanders Care Patient Surgery 16th Rothrock Test BankfahedqNessuna valutazione finora
- ISBAR Communication - Communication Is KeyDocumento5 pagineISBAR Communication - Communication Is KeyNaNa HunNessuna valutazione finora
- STV - SWITCH-safety PatienDocumento14 pagineSTV - SWITCH-safety PatienMuhammad ZainuddinNessuna valutazione finora
- FMA - Research Report-Richmond AustriaDocumento8 pagineFMA - Research Report-Richmond Austriarichmond_austria7635Nessuna valutazione finora
- ISBAR For Clear CommunicationDocumento6 pagineISBAR For Clear Communicationmehara1920Nessuna valutazione finora
- Clinical Handover and Patient Safety Literature Review Report 2005Documento5 pagineClinical Handover and Patient Safety Literature Review Report 2005gw163ckjNessuna valutazione finora
- Final Safety Group Paper490WDocumento17 pagineFinal Safety Group Paper490WLYZETTE TERMANNessuna valutazione finora
- JCIDocumento54 pagineJCIanaskamel82Nessuna valutazione finora
- Groah 2014 Table TalkDocumento12 pagineGroah 2014 Table TalkChandra JohannesNessuna valutazione finora
- CF Rca TemplateDocumento8 pagineCF Rca TemplateEsteban García EcheverryNessuna valutazione finora
- Sample - Critical Review of ArticleDocumento11 pagineSample - Critical Review of Articleacademicproffwritter100% (1)
- Nursing Sensitive Indicators Their RoleDocumento3 pagineNursing Sensitive Indicators Their RolePuspita Eka Kurnia SariNessuna valutazione finora
- Good Practice 12 Patient HandoverDocumento4 pagineGood Practice 12 Patient HandoverDewi Ratna SariNessuna valutazione finora
- Radiation SafetyDocumento4 pagineRadiation Safetyapi-696520673Nessuna valutazione finora
- Roils PaperDocumento4 pagineRoils Paperapi-575843507Nessuna valutazione finora
- Advance Nursing PracticeDocumento5 pagineAdvance Nursing PracticeNisrin SaudNessuna valutazione finora
- Hand Off CommunicationDocumento6 pagineHand Off CommunicationALELAW100% (1)
- Surgical Safety ChecklistDocumento11 pagineSurgical Safety ChecklistEdy TahirNessuna valutazione finora
- NPSA001 Smith 2008 Bedside CheckingDocumento107 pagineNPSA001 Smith 2008 Bedside CheckingHUZEFANessuna valutazione finora
- Primary Urgent Care Guidelines UtiDocumento22 paginePrimary Urgent Care Guidelines UtiUti Nilam SariNessuna valutazione finora
- RoilspaperDocumento5 pagineRoilspaperapi-530717893Nessuna valutazione finora
- Dispensing EnvironmentDocumento72 pagineDispensing EnvironmentLeo Gonzales Calayag100% (1)
- Ipc 1Documento6 pagineIpc 1Luthfi HamdaNessuna valutazione finora
- BHA-FPX4106 - Nadhirah Lutchminarain - Assignment 1Documento11 pagineBHA-FPX4106 - Nadhirah Lutchminarain - Assignment 1Nadhirah De WetNessuna valutazione finora
- Nursing Documentation in Occupational HealthDocumento7 pagineNursing Documentation in Occupational HealthLaila JaneNessuna valutazione finora
- Article ReviewDocumento15 pagineArticle ReviewHamza Dawid HamidNessuna valutazione finora
- NR512 Applying Standardized TerminologiesDocumento6 pagineNR512 Applying Standardized TerminologiesHaris NoonNessuna valutazione finora
- Nursing Practice Today: Behrouz Pakcheshm, Imane Bagheri Zohreh KalaniDocumento9 pagineNursing Practice Today: Behrouz Pakcheshm, Imane Bagheri Zohreh KalaniFernando PintoNessuna valutazione finora
- Managing Change Towards Bedside Shift ReportDocumento12 pagineManaging Change Towards Bedside Shift Reportapi-438607141Nessuna valutazione finora
- Strength and Limitations of Early Warning ScoreDocumento33 pagineStrength and Limitations of Early Warning ScorePerawat CPNS 2018 RSUP Dr. KariadiNessuna valutazione finora
- Informatics ProjectDocumento7 pagineInformatics ProjectShannon TerrellNessuna valutazione finora
- Timely Simple DischargeDocumento52 pagineTimely Simple DischargeDesti Setyaningrum100% (1)
- Literature Review On Surgical Safety ChecklistDocumento11 pagineLiterature Review On Surgical Safety Checklistfut0mipujeg3100% (1)
- Nur 410 Bedside Shift ReportDocumento8 pagineNur 410 Bedside Shift Reportapi-448827323Nessuna valutazione finora
- Communication and Documentation For An Ambulatory Practice PDFDocumento25 pagineCommunication and Documentation For An Ambulatory Practice PDFSanti Galang GuadesNessuna valutazione finora
- Evidenced Based Nursing PracticeDocumento7 pagineEvidenced Based Nursing PracticeKim ViñasNessuna valutazione finora
- Quality and Safety Synthesis PaperDocumento6 pagineQuality and Safety Synthesis Paperapi-252807964Nessuna valutazione finora
- Daily Goals Tools Enhancing Outcomes in A Surgical Intensive Care Unit by ImplementingDocumento14 pagineDaily Goals Tools Enhancing Outcomes in A Surgical Intensive Care Unit by ImplementingAnugerah Eka PurwantiNessuna valutazione finora
- tmp7B69 TMPDocumento7 paginetmp7B69 TMPFrontiersNessuna valutazione finora
- NHS-FPX 4000 Applying Library Research SkillsDocumento7 pagineNHS-FPX 4000 Applying Library Research SkillsIrene WafulaNessuna valutazione finora
- Hewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingDocumento17 pagineHewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingCatrin_HutaurukNessuna valutazione finora
- Macapaz, EBR SBARDocumento2 pagineMacapaz, EBR SBARpius troy macapazNessuna valutazione finora
- Root Cause AnalysisDocumento5 pagineRoot Cause Analysisapi-520985654Nessuna valutazione finora
- ISBAR Communication - Communication Is KeyDocumento4 pagineISBAR Communication - Communication Is KeyalghazaliktdNessuna valutazione finora
- Clinical Decision Support SystemsDocumento8 pagineClinical Decision Support SystemsPushpendra ChauhanNessuna valutazione finora
- SafetyNET Community-Based Patient SafetyDocumento13 pagineSafetyNET Community-Based Patient SafetyGiovanna Gabriela Gachagoque RodriguezNessuna valutazione finora
- Patient Safety in RadoncDocumento4 paginePatient Safety in Radoncapi-575843507Nessuna valutazione finora
- The Implementation of Patient Safety Culture Deny Gunawan - CompressedDocumento7 pagineThe Implementation of Patient Safety Culture Deny Gunawan - Compresseddeny gunawanNessuna valutazione finora
- Or JournalDocumento2 pagineOr JournalNathaniel PulidoNessuna valutazione finora
- Applying Lean Principles To Reduce Wait Times in A VA Emergency DepartmentDocumento10 pagineApplying Lean Principles To Reduce Wait Times in A VA Emergency DepartmentNida KhoiriahNessuna valutazione finora
- Situation, Background, AssessmentDocumento25 pagineSituation, Background, AssessmentFemtoson georgeNessuna valutazione finora
- Making Health Care Safer.2Documento9 pagineMaking Health Care Safer.2YANNessuna valutazione finora
- Removal of Sharp Object Patient SaftyDocumento6 pagineRemoval of Sharp Object Patient SaftyAlibaba AlihaihaiNessuna valutazione finora
- Advances in The Management of Perioperative Patients Thirst 2020Documento16 pagineAdvances in The Management of Perioperative Patients Thirst 2020agung MaulanaNessuna valutazione finora
- Roils PaperDocumento4 pagineRoils Paperapi-569210408Nessuna valutazione finora
- Teaching Clinical Handover With ISBAR: Review Open AccessDocumento8 pagineTeaching Clinical Handover With ISBAR: Review Open AccessFernando PintoNessuna valutazione finora
- Advanced Practice and Leadership in Radiology NursingDa EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNessuna valutazione finora
- Musttool PDFDocumento6 pagineMusttool PDFAshly NygilNessuna valutazione finora
- Sepsis AlgorithmDocumento1 paginaSepsis AlgorithmAshly Nygil100% (1)
- Reading Sample Test 1 Part A All Professions 2010 PDFDocumento8 pagineReading Sample Test 1 Part A All Professions 2010 PDFKamal jeet KaurNessuna valutazione finora
- Behavioural Problems in ChildrenDocumento49 pagineBehavioural Problems in ChildrenAshly Nygil100% (1)
- Lesson Plan Section IDocumento17 pagineLesson Plan Section IAshly NygilNessuna valutazione finora
- Genetic TestingDocumento50 pagineGenetic TestingAshly NygilNessuna valutazione finora
- Organic Mental DisordersDocumento30 pagineOrganic Mental DisordersAshly Nygil100% (1)
- Patient Transfer Inter-Departement Sheet Situation: Please Use Patient ID Label When AvailableDocumento3 paginePatient Transfer Inter-Departement Sheet Situation: Please Use Patient ID Label When AvailableagungNessuna valutazione finora
- Sbar CommunicationDocumento20 pagineSbar CommunicationAngelyn SalimbajonNessuna valutazione finora
- Burgen Er 2020Documento5 pagineBurgen Er 2020HatikahatyNessuna valutazione finora
- Respiratory Physiotherapy Pocketbook An On Call Survival Guide Physiotherapy Pocketbooks 3Rd Edition Jane Cross All ChapterDocumento68 pagineRespiratory Physiotherapy Pocketbook An On Call Survival Guide Physiotherapy Pocketbooks 3Rd Edition Jane Cross All Chaptervincent.pathak166100% (10)
- Workshop On Early Warning Score System - Ali HaedarDocumento76 pagineWorkshop On Early Warning Score System - Ali HaedarVicky ShuarNessuna valutazione finora
- 5th Edition Hospital STD April 2020 PDFDocumento148 pagine5th Edition Hospital STD April 2020 PDFFeroz Ikbal100% (1)
- Nursing Handoffs A Systematic Review of The.26Documento11 pagineNursing Handoffs A Systematic Review of The.26Zoa Ng Wai Kwan100% (2)
- SBAR Technique For Communication: A Situational Briefing ModelDocumento3 pagineSBAR Technique For Communication: A Situational Briefing ModelRuang DahliaNessuna valutazione finora
- Running Head: Elements of An Organizational Model of Health CareDocumento7 pagineRunning Head: Elements of An Organizational Model of Health Careklm klmNessuna valutazione finora
- SBARDocumento2 pagineSBARNabiela Aswaty 2011125083Nessuna valutazione finora
- SH CP 43 Physical Assessment and Monitoring Policy V4 4.4.19Documento46 pagineSH CP 43 Physical Assessment and Monitoring Policy V4 4.4.19Yuspita IpitNessuna valutazione finora
- ICSI - Prevention of Unintentionally Retained Foreign Objects During Vaginal DeliveriesDocumento31 pagineICSI - Prevention of Unintentionally Retained Foreign Objects During Vaginal DeliveriesRobert GreenleeNessuna valutazione finora
- Ignatavicius: Medical-Surgical Nursing, 7th EditionDocumento9 pagineIgnatavicius: Medical-Surgical Nursing, 7th EditionGERALDE CHARLESNessuna valutazione finora
- Interprofessional Communication in Healthcare An Integrative ReviewDocumento21 pagineInterprofessional Communication in Healthcare An Integrative ReviewZoordiNessuna valutazione finora
- IC - Quality and SafetyDocumento6 pagineIC - Quality and SafetyDharylle CariñoNessuna valutazione finora
- Sbar Simulation ReflectionDocumento3 pagineSbar Simulation Reflectionapi-314635911100% (2)
- Semester 3 Learning PlanDocumento3 pagineSemester 3 Learning Planapi-315231385Nessuna valutazione finora
- Sbar Template 08Documento2 pagineSbar Template 08ayuNessuna valutazione finora
- Emergency Preparedness: Code White (Violent Person) : University Health Network Policy & Procedure ManualDocumento24 pagineEmergency Preparedness: Code White (Violent Person) : University Health Network Policy & Procedure Manualmargi13Nessuna valutazione finora
- Documenting, Reporting, Conferring, and Using InformaticsDocumento92 pagineDocumenting, Reporting, Conferring, and Using InformaticsZhiela Esteban AbivaNessuna valutazione finora
- Bell FiveGenerationsInTheNursingWorkforce 2013 PDFDocumento6 pagineBell FiveGenerationsInTheNursingWorkforce 2013 PDFarie susantoNessuna valutazione finora
- Advanced Life Support Obstetrics 2020Documento399 pagineAdvanced Life Support Obstetrics 2020Chalee InkateNessuna valutazione finora
- 3020 Unfolding Case Study Burns 1Documento2 pagine3020 Unfolding Case Study Burns 1api-546391110Nessuna valutazione finora
- Using SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation TeamsDocumento54 pagineUsing SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teamsmehara1920Nessuna valutazione finora
- Ethics of Nursing Shift ReportDocumento5 pagineEthics of Nursing Shift ReportkelllyNessuna valutazione finora
- New Test of Competence Webinar Slides 3 December 2020Documento42 pagineNew Test of Competence Webinar Slides 3 December 2020Donald QuackNessuna valutazione finora