Potrebbero piacerti anche
- Arteri LineDocumento13 pagineArteri Linemuthia octavianaNessuna valutazione finora
- Intra-Arterial Catheterization For Invasive Monitoring: Indications, Insertion Techniques, and Interpretation - UpToDateDocumento40 pagineIntra-Arterial Catheterization For Invasive Monitoring: Indications, Insertion Techniques, and Interpretation - UpToDatejuanpbagurNessuna valutazione finora
- CVP MonitoringDocumento10 pagineCVP MonitoringRaghu RajanNessuna valutazione finora
- Peripherally Inserted Central CatheterDocumento4 paginePeripherally Inserted Central CatheterDivine Grace Arreglo AbingNessuna valutazione finora
- 2 150507152224 Lva1 App6892Documento55 pagine2 150507152224 Lva1 App6892poojaNessuna valutazione finora
- O o o o o o o o o o o oDocumento9 pagineO o o o o o o o o o o oAshish PandeyNessuna valutazione finora
- Central Venous AccessDocumento20 pagineCentral Venous AccessCarlos GuerreroNessuna valutazione finora
- (FEU) Central Venous Pressure Notes PDFDocumento25 pagine(FEU) Central Venous Pressure Notes PDFBryJos tiongsonNessuna valutazione finora
- Acesso Vascular EmergenciaDocumento9 pagineAcesso Vascular EmergenciaSílvia TrindadeNessuna valutazione finora
- Discuss Reasons Why Patients Might Need Central Venous AccessDocumento7 pagineDiscuss Reasons Why Patients Might Need Central Venous AccessKandie LoweNessuna valutazione finora
- Hemodialysis Shunt, Graft, and Fistula CareDocumento11 pagineHemodialysis Shunt, Graft, and Fistula CareArjon Clint Reyes SulapasNessuna valutazione finora
- Critical Care ProtocolsDocumento19 pagineCritical Care ProtocolsPrabhat KumarNessuna valutazione finora
- Arterial Lines MonitoringDocumento13 pagineArterial Lines MonitoringJoseph Beredo33% (3)
- Cateter Venoso Central PDFDocumento37 pagineCateter Venoso Central PDFClaris PachecoNessuna valutazione finora
- Overview of Central Venous Access - UpToDateDocumento27 pagineOverview of Central Venous Access - UpToDateJAvier GarciaNessuna valutazione finora
- Placement of An Arterial LineDocumento2 paginePlacement of An Arterial Linem0ka7Nessuna valutazione finora
- Sister Nivedita Govt. Nursing College Igmc, ShimlaDocumento10 pagineSister Nivedita Govt. Nursing College Igmc, ShimlashivaniNessuna valutazione finora
- IV Cannulation and Fixation Infusion PumpDocumento23 pagineIV Cannulation and Fixation Infusion PumpUday Kumar0% (1)
- CVPDocumento25 pagineCVPNikhil YadavNessuna valutazione finora
- Cap 2013 NejmDocumento7 pagineCap 2013 NejmpaulaandreavargasbNessuna valutazione finora
- Intravenous FluidsDocumento3 pagineIntravenous FluidsKristine Artes AguilarNessuna valutazione finora
- CVC Partner 1Documento40 pagineCVC Partner 1stefani83Nessuna valutazione finora
- Overview of Central Venous AccessDocumento13 pagineOverview of Central Venous AccessnathanaelandryNessuna valutazione finora
- Hemodynamic Monitoring 1Documento10 pagineHemodynamic Monitoring 1Savita HanamsagarNessuna valutazione finora
- Central Venous CatheterDocumento5 pagineCentral Venous Catheterasmaa_gamal14Nessuna valutazione finora
- Acesso VenosoDocumento4 pagineAcesso VenosoAnderson AmaralNessuna valutazione finora
- Chest Drain ManagementDocumento7 pagineChest Drain ManagementanuzNessuna valutazione finora
- Procedure-Central Venous Access Catheter InsertionDocumento18 pagineProcedure-Central Venous Access Catheter Insertionmohamad dildarNessuna valutazione finora
- kh7 CVPDocumento50 paginekh7 CVPأبوأحمد الحكيمNessuna valutazione finora
- Intravenous CannulationDocumento37 pagineIntravenous CannulationUday KumarNessuna valutazione finora
- Central Venous CathetersDocumento17 pagineCentral Venous Catheterslulu vox100% (1)
- Central Venous PressureDocumento4 pagineCentral Venous Pressuremike_steven12Nessuna valutazione finora
- Insertion of Umbilical Lines in NeonatesDocumento6 pagineInsertion of Umbilical Lines in Neonatesgaaneshsubra5Nessuna valutazione finora
- Seminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingDocumento52 pagineSeminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingAyen AlingNessuna valutazione finora
- Vascular AccessDocumento48 pagineVascular AccessJason Samuel Fredrick100% (4)
- Newcastle Neonatal Service Guidelines Vascular AccessDocumento5 pagineNewcastle Neonatal Service Guidelines Vascular AccessVineet KumarNessuna valutazione finora
- Common Procedures in Paediatric IcuDocumento17 pagineCommon Procedures in Paediatric IcuNeethu Mariya MathewNessuna valutazione finora
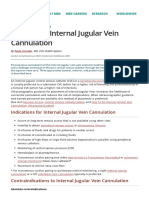
- How To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionDocumento9 pagineHow To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionnaveenNessuna valutazione finora
- Umbilical Vein CatheterizationDocumento3 pagineUmbilical Vein CatheterizationrohitNessuna valutazione finora
- Arterial Blood GasDocumento55 pagineArterial Blood GasDharlyn MungcalNessuna valutazione finora
- Nasogastric Tube InsertionDocumento11 pagineNasogastric Tube InsertionDiane Kate Tobias Magno100% (1)
- Acesso Venoso TecnicaDocumento16 pagineAcesso Venoso TecnicaNatascha CabralNessuna valutazione finora
- Arterial LineDocumento2 pagineArterial LineRaghav Goyal100% (1)
- Hemodynamic MonitoringDocumento10 pagineHemodynamic MonitoringDivya Joy100% (1)
- CVP Care (Swapnil (Documento18 pagineCVP Care (Swapnil (SWAPNIL WANJARINessuna valutazione finora
- Hemodynamics MonitoringDocumento12 pagineHemodynamics MonitoringBhawna Joshi100% (3)
- Group3 - Sunico, Valenzuna, VelezDocumento15 pagineGroup3 - Sunico, Valenzuna, VelezMichelle SunicoNessuna valutazione finora
- CVPDocumento23 pagineCVPShalini KaluraNessuna valutazione finora
- DR Tarun BhatnagarDocumento40 pagineDR Tarun Bhatnagararhim aljalyNessuna valutazione finora
- CVP Line CareDocumento37 pagineCVP Line CareArvindJoshiNessuna valutazione finora
- Thoracentesis NejmDocumento4 pagineThoracentesis Nejmton-ton-toniNessuna valutazione finora
- 42nd Issue-Article 136Documento2 pagine42nd Issue-Article 136Sohil ElfarNessuna valutazione finora
- CVP Final 2021Documento11 pagineCVP Final 2021Ahmed AshrafNessuna valutazione finora
- Percutaneous Transluminal Coronary AngioplastyDocumento22 paginePercutaneous Transluminal Coronary AngioplastyArya Gaunker100% (1)
- Central Venous Access: RSUD Duren SawitDocumento48 pagineCentral Venous Access: RSUD Duren SawitMonica HerdiatiNessuna valutazione finora
- Akses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaDocumento28 pagineAkses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaSaeful AmbariNessuna valutazione finora
- Central LinesDocumento7 pagineCentral LineslaneeceshariNessuna valutazione finora
- Placement of Subclavian Venous CathetersDocumento36 paginePlacement of Subclavian Venous CathetersCourtneykdNessuna valutazione finora
- Demonstration On Iv CannulationDocumento54 pagineDemonstration On Iv CannulationAnusha100% (1)
- Vit ADocumento9 pagineVit AmalathiNessuna valutazione finora
- IddcpDocumento6 pagineIddcpmalathi100% (1)
- Types of Shock: Ms. Saheli Chakraborty 2 Year MSC Nursing Riner, BangaloreDocumento36 pagineTypes of Shock: Ms. Saheli Chakraborty 2 Year MSC Nursing Riner, Bangaloremalathi100% (6)
- Vit ADocumento9 pagineVit AmalathiNessuna valutazione finora
- GlaucomeaDocumento21 pagineGlaucomeamalathiNessuna valutazione finora
- PeritonitisDocumento232 paginePeritonitismalathiNessuna valutazione finora
- Neuroo 170210095341 PDFDocumento162 pagineNeuroo 170210095341 PDFmalathiNessuna valutazione finora
- Total Quality Management in Healthcare Organizations An OverviewDocumento37 pagineTotal Quality Management in Healthcare Organizations An OverviewmalathiNessuna valutazione finora
- PeritonitisDocumento232 paginePeritonitismalathiNessuna valutazione finora
- Summary of The Alberta Clinical Practice Guideline, August 1996Documento2 pagineSummary of The Alberta Clinical Practice Guideline, August 1996malathiNessuna valutazione finora
- Ana 2 LecDocumento32 pagineAna 2 LecmalathiNessuna valutazione finora
- 19 October 2019Documento126 pagine19 October 2019malathiNessuna valutazione finora
- Submitted by Balkeej Kaur MSC 1 Year Acon, Sri Muktsar SahibDocumento41 pagineSubmitted by Balkeej Kaur MSC 1 Year Acon, Sri Muktsar SahibmalathiNessuna valutazione finora
- Total Quality Management (TQM)Documento31 pagineTotal Quality Management (TQM)malathi100% (1)
- Efinitions:: Career Opportunities: An Individual Should Start Career Planning Right From Childhood. ..Documento40 pagineEfinitions:: Career Opportunities: An Individual Should Start Career Planning Right From Childhood. ..malathiNessuna valutazione finora
- HerniaDocumento47 pagineHerniamalathiNessuna valutazione finora
- AndardsDocumento50 pagineAndardsmalathiNessuna valutazione finora
- Chapt 44 GallbladderDocumento85 pagineChapt 44 GallbladdermalathiNessuna valutazione finora
- Hypertension Research PaperDocumento73 pagineHypertension Research PaperLadylace AmandyNessuna valutazione finora
- 0 en Brochure Angiodroid 2020Documento12 pagine0 en Brochure Angiodroid 2020Produtos IntraviewNessuna valutazione finora
- Dr. Linus Pauling Heart Protocol (Pauling Therapy) With 12 Grams of Vitamin C and 6 Grams of LysineDocumento2 pagineDr. Linus Pauling Heart Protocol (Pauling Therapy) With 12 Grams of Vitamin C and 6 Grams of LysineEbook PdfNessuna valutazione finora
- FITTP and Red Flags TabulationDocumento4 pagineFITTP and Red Flags Tabulationalyssa marie salcedo100% (2)
- Levo-Milri 2021Documento7 pagineLevo-Milri 2021Fer AlmazanNessuna valutazione finora
- 10 1016@j Chest 2020 09 269Documento29 pagine10 1016@j Chest 2020 09 269Wanderson100% (1)
- 2020-03-01 Reader's DigestDocumento134 pagine2020-03-01 Reader's DigestHisha AlainaNessuna valutazione finora
- 2020 08 10 Sanjay Pandarbale Yogesh Nerkar Sufala MalnekarDocumento4 pagine2020 08 10 Sanjay Pandarbale Yogesh Nerkar Sufala MalnekarYogesh NerkarNessuna valutazione finora
- Evidence Based Cardiology 4th EdDocumento424 pagineEvidence Based Cardiology 4th EdROGER LUDEÑA SALAZARNessuna valutazione finora
- Adrenaline - EpinephrineDocumento3 pagineAdrenaline - Epinephrinesweety DangiNessuna valutazione finora
- Physiology Practical 2: Toad HeartDocumento10 paginePhysiology Practical 2: Toad HeartAdams OdanjiNessuna valutazione finora
- Dabl Educational TrustMonitors For Self-Measurement of Blood Pressure (SBPM)Documento1 paginaDabl Educational TrustMonitors For Self-Measurement of Blood Pressure (SBPM)iranbengoaNessuna valutazione finora
- DEFIBRILLATORDocumento12 pagineDEFIBRILLATORRajath N Gowda 1SG18EE062Nessuna valutazione finora
- Cardiology Investigation Echo Doppler (2D Echo) EchocardiographyDocumento2 pagineCardiology Investigation Echo Doppler (2D Echo) EchocardiographyManohar Kumar100% (2)
- Aortic DissectionDocumento24 pagineAortic Dissectionsameeha semiNessuna valutazione finora
- CT2p7E-Biology Paper 3 TZ1 HL-1Documento14 pagineCT2p7E-Biology Paper 3 TZ1 HL-156ch5k5p7nNessuna valutazione finora
- Appropriation Weeks 4-5Documento6 pagineAppropriation Weeks 4-5AURA CAMILA LEÓN ÁLVAREZNessuna valutazione finora
- Overview of The Circulation Pressure, Flow and ResistanceDocumento7 pagineOverview of The Circulation Pressure, Flow and ResistanceSalsabilla Ameranti PutriNessuna valutazione finora
- Pulse PressureDocumento3 paginePulse PressureYovie Anggara SaputraNessuna valutazione finora
- GE Discovery VCT BrochureDocumento11 pagineGE Discovery VCT Brochurerabbani.moNessuna valutazione finora
- 7100RELDocumento52 pagine7100RELCarlos CarreñoNessuna valutazione finora
- A Cluster-Randomizaed Trial of Blood-Pressure Reduction in Black BaDocumento11 pagineA Cluster-Randomizaed Trial of Blood-Pressure Reduction in Black BaRoberto SanchezNessuna valutazione finora
- Communicative English Lab ManualDocumento8 pagineCommunicative English Lab ManualJCT Placement CellNessuna valutazione finora
- ECG QuizDocumento6 pagineECG QuizIsland Rae100% (1)
- (PDF) A Study of Noninvasive Cardiac Output and Other Cardiorespiratory Parameters in Various Neurosurgical PositionsDocumento11 pagine(PDF) A Study of Noninvasive Cardiac Output and Other Cardiorespiratory Parameters in Various Neurosurgical PositionsSadhi RashydNessuna valutazione finora
- Study: Length/ Significant Digits Controlled TermsDocumento36 pagineStudy: Length/ Significant Digits Controlled TermsHarish NuvvulaNessuna valutazione finora
- Dr. Satyam Rajvanshi Dr. Ram Manohar Lohia Hospital, New DelhiDocumento124 pagineDr. Satyam Rajvanshi Dr. Ram Manohar Lohia Hospital, New DelhiazizhaNessuna valutazione finora
- Tabel Dosis Nicardipine: Pelarut/Cairan Infus Yang Dapat DigunakanDocumento8 pagineTabel Dosis Nicardipine: Pelarut/Cairan Infus Yang Dapat DigunakanAtik LestariNessuna valutazione finora
- Circulatory System WorksheetDocumento2 pagineCirculatory System Worksheetrubixcube4550% (12)
- ECG Diagnosis: Right Ventricular Myocardial Infarction: Clinical MedicineDocumento2 pagineECG Diagnosis: Right Ventricular Myocardial Infarction: Clinical MedicineNadyaindriati96Nessuna valutazione finora