Potrebbero piacerti anche
- CNHS SHS Enrollment Form 2019Documento2 pagineCNHS SHS Enrollment Form 2019Arthur Capawing100% (8)
- Thesis 1 Syllabus ONLINEDocumento11 pagineThesis 1 Syllabus ONLINEEarl averzosa100% (2)
- Philippine Indigenous Communities: A Strong Partner For Sustainable DevelopmentDocumento66 paginePhilippine Indigenous Communities: A Strong Partner For Sustainable DevelopmentROSARIO CHARLENE IRISH P.Nessuna valutazione finora
- ASSCAT Vision, Mission & Quality PolicyDocumento16 pagineASSCAT Vision, Mission & Quality PolicyRuby Jane DuradoNessuna valutazione finora
- Application For Afp Service Aptitude TestDocumento1 paginaApplication For Afp Service Aptitude Testジェラルド ジェラルドNessuna valutazione finora
- Benefits of Taking TESDA CoursesDocumento2 pagineBenefits of Taking TESDA CoursesJun-Jun Putot PagoyNessuna valutazione finora
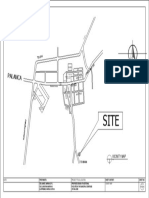
- Vicinity MapDocumento1 paginaVicinity MapJonathan Marvin DueNessuna valutazione finora
- List of Trainings of TeachersDocumento2 pagineList of Trainings of TeachersMaTheresaRosarioBulataoNessuna valutazione finora
- House DrainDocumento19 pagineHouse DrainDonna Cece MelgarNessuna valutazione finora
- BFP RequirementsDocumento4 pagineBFP RequirementsJohn Blake GriffinNessuna valutazione finora
- Water Line Layout Sewer and Drainage Layout P-2: Ground Floor IsometricDocumento1 paginaWater Line Layout Sewer and Drainage Layout P-2: Ground Floor IsometricAubrey ManelleNessuna valutazione finora
- 11th Most Outstanding Civil Engineer StudentDocumento2 pagine11th Most Outstanding Civil Engineer Studentanjenineg0% (1)
- Application Form For The Oral DefenseDocumento1 paginaApplication Form For The Oral DefenseKath PalabricaNessuna valutazione finora
- (Fibonacci) Seatwork 1 Answers - LeftDocumento2 pagine(Fibonacci) Seatwork 1 Answers - LeftZeri LabadiaNessuna valutazione finora
- Reaction PaperDocumento2 pagineReaction PaperjennyNessuna valutazione finora
- Educ 3 ReviewerDocumento21 pagineEduc 3 ReviewerMa.Lourdes CamporidondoNessuna valutazione finora
- Job Proficiency Rating SheetDocumento3 pagineJob Proficiency Rating SheetnellafayericoNessuna valutazione finora
- Cnu Cte LetterheadDocumento1 paginaCnu Cte LetterheadIce EscolanoNessuna valutazione finora
- Survey QuestionnaireDocumento10 pagineSurvey Questionnaireromeo pilongo0% (1)
- Purposive Communication: Module 7: Communication For Various PurposesDocumento11 paginePurposive Communication: Module 7: Communication For Various PurposesKatherine Marie BerouNessuna valutazione finora
- Terminologies in Simple CurveDocumento8 pagineTerminologies in Simple Curvejason roqueNessuna valutazione finora
- 1st Assessment Exam in Specialization 2020 - 2021 With Answer KeyDocumento3 pagine1st Assessment Exam in Specialization 2020 - 2021 With Answer KeyDhealine Jusayan100% (1)
- HandbookDocumento145 pagineHandbookRondipsNessuna valutazione finora
- Narrative ReportDocumento24 pagineNarrative ReportNineveh FernandoNessuna valutazione finora
- WoW BiPSU LEARNING CONTINUITY PLANDocumento23 pagineWoW BiPSU LEARNING CONTINUITY PLANDGDelfin100% (1)
- Surveying: Polytechnic University of The PhilippinesDocumento84 pagineSurveying: Polytechnic University of The Philippinesacurvz2005Nessuna valutazione finora
- Mountaineering: A History For FilipinosDocumento11 pagineMountaineering: A History For FilipinosGiorjia Mae VeranNessuna valutazione finora
- Praise and Worship Line UpDocumento14 paginePraise and Worship Line UpjayroldparcedeNessuna valutazione finora
- Taping Over Uneven SlopeDocumento3 pagineTaping Over Uneven SlopeShealtiel Regine Cinco-AyalaNessuna valutazione finora
- Pinning CeremonyDocumento4 paginePinning CeremonyJOHN POL MAGLASANGNessuna valutazione finora
- Tos Language Programs and Policies in Multilingual SocietiesDocumento2 pagineTos Language Programs and Policies in Multilingual SocietiesBernadette Barro Gomez100% (1)
- Biscast Nexus PaperDocumento1 paginaBiscast Nexus PaperAnonymous otTloRzXhNessuna valutazione finora
- 5 - Setting Up Surveying InstrumentsDocumento4 pagine5 - Setting Up Surveying InstrumentsAbi ArcadioNessuna valutazione finora
- Research Paper Chapter 2Documento6 pagineResearch Paper Chapter 2lucas100% (1)
- Rules of BadmintonDocumento7 pagineRules of BadmintonAllan F. RolomaNessuna valutazione finora
- RRL and Frameworks PDFDocumento47 pagineRRL and Frameworks PDFXXXXXNessuna valutazione finora
- Supreme Student Government WorkplanDocumento3 pagineSupreme Student Government WorkplanCharena Pavia VillegasNessuna valutazione finora
- Entrep Chapter 2 LessonDocumento20 pagineEntrep Chapter 2 LessonMyrna Delos Santos AbuniawanNessuna valutazione finora
- Curriculum Development For Teachers 2014Documento95 pagineCurriculum Development For Teachers 2014Glory fil Amor GarciaNessuna valutazione finora
- Statistical Treatment of DataDocumento1 paginaStatistical Treatment of DataKaty Martha100% (1)
- TH Differential Calculus Solution PDFDocumento4 pagineTH Differential Calculus Solution PDFEdwin Quinlat DevizaNessuna valutazione finora
- Tuguegarao City, Cagayan 3500: St. Paul University PhilippinesDocumento57 pagineTuguegarao City, Cagayan 3500: St. Paul University Philippinesmarchelly simonNessuna valutazione finora
- Case AnalysisDocumento1 paginaCase Analysis나다니엘Nessuna valutazione finora
- Dela Cruz, Kyla J. Term Paper 12 Civil Engineering and Environmental ScienceDocumento12 pagineDela Cruz, Kyla J. Term Paper 12 Civil Engineering and Environmental ScienceKyla Dela CruzNessuna valutazione finora
- Ra 10621Documento6 pagineRa 10621Angel VirayNessuna valutazione finora
- Worksheet 1 & 2 Mathematics in The Modern WorldDocumento2 pagineWorksheet 1 & 2 Mathematics in The Modern WorldJENNIFER BALMES100% (2)
- Title of The Research Paper: Isabela State University - Echague, IsabelaDocumento2 pagineTitle of The Research Paper: Isabela State University - Echague, IsabelaNatasha Mae BatagNessuna valutazione finora
- VMGODocumento35 pagineVMGOFrancis CalubayanNessuna valutazione finora
- Narrative: Denr Cenro Jampason, Initao, Misamis OrientalDocumento34 pagineNarrative: Denr Cenro Jampason, Initao, Misamis OrientalJoseniel Antipasado LuegoNessuna valutazione finora
- Cavite State University: Cvsu Vision Cvsu MissionDocumento16 pagineCavite State University: Cvsu Vision Cvsu MissionAira MaeNessuna valutazione finora
- EDFS 21 BSEM3 - Module 1Documento20 pagineEDFS 21 BSEM3 - Module 1Mary ann GarciaNessuna valutazione finora
- Trainee: Progress Chart Front Office Services NciiDocumento24 pagineTrainee: Progress Chart Front Office Services NciiCatherine Mae Lammag BuananNessuna valutazione finora
- Unit 6 Ensure Teacher Quality Through Competency Framework and StandardsDocumento25 pagineUnit 6 Ensure Teacher Quality Through Competency Framework and StandardsJoshuaNessuna valutazione finora
- Chapter 3 North Grand Haven Kulang Nalang NG Chapter 5Documento163 pagineChapter 3 North Grand Haven Kulang Nalang NG Chapter 5Mymy santosNessuna valutazione finora
- Ce 3151 and Ce 3151d (Lec and Lab)Documento75 pagineCe 3151 and Ce 3151d (Lec and Lab)Asus LaptopNessuna valutazione finora
- Prelim Exam in Stat.Documento4 paginePrelim Exam in Stat.MICHELLE DE LOS REYES100% (1)
- CPE 110 - Second SemDocumento4 pagineCPE 110 - Second SemYla Monique PareñasNessuna valutazione finora
- MBA - 5 PagesDocumento5 pagineMBA - 5 PagesRitu MathurNessuna valutazione finora
- Evaluation ToolsDocumento4 pagineEvaluation ToolsJessa Mae Alegarme AlduhesaNessuna valutazione finora
- Internship Evaluation FormDocumento3 pagineInternship Evaluation Formnaruto uzumakiNessuna valutazione finora
- Appliance Scheduling Optimization With MDocumento82 pagineAppliance Scheduling Optimization With MJay ZamoraNessuna valutazione finora
- CareUEyes - Free Blue Light Filter, Screen Dimmer - 1.1.24.3 - CrackDocumento1 paginaCareUEyes - Free Blue Light Filter, Screen Dimmer - 1.1.24.3 - CrackJay ZamoraNessuna valutazione finora
- Introduction OjtDocumento4 pagineIntroduction OjtJay ZamoraNessuna valutazione finora
- S. W. O. T. Analysis: StrengthDocumento4 pagineS. W. O. T. Analysis: StrengthJay ZamoraNessuna valutazione finora
- Existing Power Plants Mindanao December 2017Documento2 pagineExisting Power Plants Mindanao December 2017Jay ZamoraNessuna valutazione finora
- Maxima and AtesDocumento16 pagineMaxima and AtesJay ZamoraNessuna valutazione finora
- Dost SPTP PDFDocumento6 pagineDost SPTP PDFJay ZamoraNessuna valutazione finora
- 09 - Chapter 3 PDFDocumento24 pagine09 - Chapter 3 PDFShamshuddin nadafNessuna valutazione finora
- Syllabus For Educational Courses in Integrated BED VBU Hazaribag PDFDocumento112 pagineSyllabus For Educational Courses in Integrated BED VBU Hazaribag PDFRajeev Ranjan100% (1)
- CHCDIV001 2 Knowledge Questions 1Documento4 pagineCHCDIV001 2 Knowledge Questions 1Carl Samson60% (5)
- Fate Plus 3 Martial Arts PDFDocumento38 pagineFate Plus 3 Martial Arts PDFIcaro 24Nessuna valutazione finora
- The Cambridge History of Libraries in Britain and Ireland, Volume 1 PDFDocumento660 pagineThe Cambridge History of Libraries in Britain and Ireland, Volume 1 PDFBalan VioletaNessuna valutazione finora
- BlazBlue - Phase 0Documento194 pagineBlazBlue - Phase 0Ivan KirinecNessuna valutazione finora
- Teaching and Teacher Education: Jo Westbrook, Alison CroftDocumento9 pagineTeaching and Teacher Education: Jo Westbrook, Alison CroftVictor PuglieseNessuna valutazione finora
- (Hinduism) John M. Denton - Gems of Advaita Vedanta - Philosophy of Unity_ A Sanskrit Reader with Selected Significant Philosophical Excerpts from the Upanishads, Bhagavad Gita, Vivekacudamani and OthDocumento144 pagine(Hinduism) John M. Denton - Gems of Advaita Vedanta - Philosophy of Unity_ A Sanskrit Reader with Selected Significant Philosophical Excerpts from the Upanishads, Bhagavad Gita, Vivekacudamani and OthAlexandre RosasNessuna valutazione finora
- Synthesis - Maximum Achievement - Brian Tracy 13p 17Documento13 pagineSynthesis - Maximum Achievement - Brian Tracy 13p 17Marya Fanta C LupuNessuna valutazione finora
- Harry Seidler Revisiting Modernism PDFDocumento24 pagineHarry Seidler Revisiting Modernism PDFBen ShenNessuna valutazione finora
- Leadership and Self-Deception - Diagrams - 20181023Documento31 pagineLeadership and Self-Deception - Diagrams - 20181023Phanniswer Ch100% (1)
- G7-Math: Ignatian Pedagogical Paradigm Lesson Plan Student PreparednessDocumento10 pagineG7-Math: Ignatian Pedagogical Paradigm Lesson Plan Student PreparednessShai Maglunsod LangotNessuna valutazione finora
- Definition of CrimeDocumento5 pagineDefinition of Crimejajubma100% (1)
- Microsoft Word - Arbitrary Reference Frame TheoryDocumento8 pagineMicrosoft Word - Arbitrary Reference Frame Theorysameerpatel157700% (1)
- SaivamDocumento62 pagineSaivamProfessorTextech100% (1)
- Unit 5Documento6 pagineUnit 5G Sindhu RavindranNessuna valutazione finora
- Review of "Turning Judaism Outward" by Chaim MillerDocumento10 pagineReview of "Turning Judaism Outward" by Chaim MillerChabad Info EnglishNessuna valutazione finora
- CSE 103: Discrete Mathematics: Predicate Rules of InferenceDocumento31 pagineCSE 103: Discrete Mathematics: Predicate Rules of InferenceAbu OUbaidaNessuna valutazione finora
- Review of "The Handbook of Morphology" by Andrew Spencer and Arnold M. Zwicky (Eds)Documento9 pagineReview of "The Handbook of Morphology" by Andrew Spencer and Arnold M. Zwicky (Eds)Pallavi HandiqueNessuna valutazione finora
- E.H. CARR-Socialism in One Country, 1924-26 Vol. 3 (A History of Soviet Russia) (1958) PDFDocumento576 pagineE.H. CARR-Socialism in One Country, 1924-26 Vol. 3 (A History of Soviet Russia) (1958) PDFHyeonwoo Kim100% (1)
- Comparison of Feelings of Inferiority Among Univer PDFDocumento5 pagineComparison of Feelings of Inferiority Among Univer PDFJohn Herald LisingNessuna valutazione finora
- Presentation ZenDocumento90 paginePresentation ZenPhillip Toland100% (7)
- Connecting The Dots Teaching Archaeology and Social RelevanceDocumento8 pagineConnecting The Dots Teaching Archaeology and Social RelevanceNicolas LaracuenteNessuna valutazione finora
- Skenario 4 SGD 23 (English)Documento16 pagineSkenario 4 SGD 23 (English)cokdebagusNessuna valutazione finora
- What Is Meant by Charactyeristic Strength of ConcreteDocumento4 pagineWhat Is Meant by Charactyeristic Strength of ConcretemmabeeNessuna valutazione finora
- Proiect de LectieDocumento4 pagineProiect de LectieBianca GloriaNessuna valutazione finora
- J A - T C L An Introduction:: OHN Ustin HE Ommand Theory OF AWDocumento6 pagineJ A - T C L An Introduction:: OHN Ustin HE Ommand Theory OF AWSubhojit DasNessuna valutazione finora
- Wilfred Owen Booklet For IOC 2012Documento26 pagineWilfred Owen Booklet For IOC 2012nadia0% (1)
- Truth MattersDocumento537 pagineTruth MattersAlexisTorres75% (4)
- HW Packet 1 - The Study of Life (KEY) PDFDocumento2 pagineHW Packet 1 - The Study of Life (KEY) PDFDavid StainesNessuna valutazione finora