Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- 2007 MCQDocumento67 pagine2007 MCQTiffani Gutierrez100% (1)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Obstetrics OverviewDocumento91 pagineObstetrics OverviewAbi TudNessuna valutazione finora
- Surgical InfectionsDocumento310 pagineSurgical InfectionsOmar Ed ChavezNessuna valutazione finora
- Plasma FibroblastDocumento11 paginePlasma FibroblastPermanent Makeup and Cryo In MaineNessuna valutazione finora
- Intestinal Obstruction 4Documento25 pagineIntestinal Obstruction 4Muvenn KannanNessuna valutazione finora
- CASP Case Control Study Checklist DownloadDocumento6 pagineCASP Case Control Study Checklist DownloadbintangNessuna valutazione finora
- Nursing Care PlanDocumento2 pagineNursing Care PlanJewelyn Bronda100% (2)
- ACP Board ReviewDocumento593 pagineACP Board ReviewC Martin TraumatoNessuna valutazione finora
- Kesici 2019Documento7 pagineKesici 2019nurahmi widyani ratriNessuna valutazione finora
- Book 1Documento2 pagineBook 1nurahmi widyani ratriNessuna valutazione finora
- NNNNNNNNNDocumento9 pagineNNNNNNNNNnurahmi widyani ratriNessuna valutazione finora
- MMMDocumento19 pagineMMMnurahmi widyani ratriNessuna valutazione finora
- Jo 8 PDFDocumento5 pagineJo 8 PDFnurahmi widyani ratriNessuna valutazione finora
- Changes in Contrast Sensitivity in Young Adults With DiabetesDocumento5 pagineChanges in Contrast Sensitivity in Young Adults With Diabetesnurahmi widyani ratriNessuna valutazione finora
- 1 s2.0 S1201971216310244 MainDocumento2 pagine1 s2.0 S1201971216310244 Mainnurahmi widyani ratriNessuna valutazione finora
- Jo 8 PDFDocumento5 pagineJo 8 PDFnurahmi widyani ratriNessuna valutazione finora
- 12 - Chronic Care ManagementDocumento54 pagine12 - Chronic Care Managementnurahmi widyani ratriNessuna valutazione finora
- WHO-SEARO Snakebite Guidelines 2010Documento162 pagineWHO-SEARO Snakebite Guidelines 2010Galantry Ahmad AzhariNessuna valutazione finora
- Nihms 604943Documento15 pagineNihms 604943nurahmi widyani ratriNessuna valutazione finora
- Nihms 604943Documento15 pagineNihms 604943nurahmi widyani ratriNessuna valutazione finora
- 10.1177 2042018810382481Documento7 pagine10.1177 2042018810382481Je SoekocoNessuna valutazione finora
- Nihms 604943Documento15 pagineNihms 604943nurahmi widyani ratriNessuna valutazione finora
- Trauma ServikalDocumento7 pagineTrauma Servikalnurahmi widyani ratriNessuna valutazione finora
- Increased Mortality Associated With The Early Coagulopathy of Trauma in Combat CasualtiesDocumento7 pagineIncreased Mortality Associated With The Early Coagulopathy of Trauma in Combat Casualtiesnurahmi widyani ratriNessuna valutazione finora
- Evaluasi Konseling Menyusui PDFDocumento9 pagineEvaluasi Konseling Menyusui PDFErica FitrianiNessuna valutazione finora
- Muchiri 2016Documento10 pagineMuchiri 2016nurahmi widyani ratriNessuna valutazione finora
- DDDDDFDocumento1 paginaDDDDDFnurahmi widyani ratriNessuna valutazione finora
- CASP Randomised Controlled Trial Checklist 2018 Fillable FormDocumento14 pagineCASP Randomised Controlled Trial Checklist 2018 Fillable Formnurahmi widyani ratriNessuna valutazione finora
- ADocumento1 paginaAnurahmi widyani ratriNessuna valutazione finora
- V. Mallikarjun RaoDocumento6 pagineV. Mallikarjun Raonurahmi widyani ratriNessuna valutazione finora
- Breastfeeding Management: Hours To Two WeeksDocumento2 pagineBreastfeeding Management: Hours To Two Weeksnurahmi widyani ratriNessuna valutazione finora
- JBI Quasi-Experimental Appraisal Tool2017Documento7 pagineJBI Quasi-Experimental Appraisal Tool2017nurahmi widyani ratriNessuna valutazione finora
- Diagnosis and Management of Acute Low Back PainDocumento2 pagineDiagnosis and Management of Acute Low Back Painnurahmi widyani ratriNessuna valutazione finora
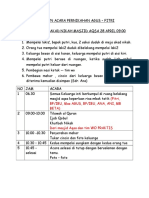
- Rundown Acara ADocumento5 pagineRundown Acara Anurahmi widyani ratriNessuna valutazione finora
- Precision Attachment: Retained OverdentureDocumento4 paginePrecision Attachment: Retained OverdentureSudhanshu Kumar KashyapNessuna valutazione finora
- Maternity Clinical Network Contact DetailsDocumento18 pagineMaternity Clinical Network Contact DetailsAlina-Gabriela MarinNessuna valutazione finora
- LPS AnnouncementsDocumento124 pagineLPS AnnouncementsNEWS CENTER MaineNessuna valutazione finora
- Bloodstream Infection Event (Central Line-Associated Bloodstream Infection and Non-Central Line Associated Bloodstream Infection)Documento50 pagineBloodstream Infection Event (Central Line-Associated Bloodstream Infection and Non-Central Line Associated Bloodstream Infection)Luthvia AnnisaNessuna valutazione finora
- Pharmacology Lab (1) : Routes of Drug AdministrationDocumento14 paginePharmacology Lab (1) : Routes of Drug AdministrationBotan AbdullahNessuna valutazione finora
- 11.efficacy and Stability of The Alar Base Cinch SutureDocumento4 pagine11.efficacy and Stability of The Alar Base Cinch SutureFabian Camelo OtorrinoNessuna valutazione finora
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocumento9 pagine2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangNessuna valutazione finora
- Scopolamine Intoxication As A Model of Transient Global AmnesiaDocumento10 pagineScopolamine Intoxication As A Model of Transient Global AmnesiaDakotaJimNessuna valutazione finora
- Progress in Retinal and Eye Research: Contents Lists Available atDocumento40 pagineProgress in Retinal and Eye Research: Contents Lists Available atSalsa BillaNessuna valutazione finora
- Unit 4: Medical EmergenciesDocumento44 pagineUnit 4: Medical EmergenciesMR々๛ AKMツNessuna valutazione finora
- Arterial DiseaseDocumento191 pagineArterial DiseaseAura DiscyacittaNessuna valutazione finora
- Ascitis Quilosa Post Cirugía Abdominal: Caso Clínico y Revisión de La LiteraturaDocumento7 pagineAscitis Quilosa Post Cirugía Abdominal: Caso Clínico y Revisión de La LiteraturaJuliet castilloNessuna valutazione finora
- Fetal Assessment DRDocumento1 paginaFetal Assessment DRMicah Lou CalambaNessuna valutazione finora
- EN - LP2 - Biopsychosocial-Model-ApproachDocumento2 pagineEN - LP2 - Biopsychosocial-Model-ApproachPinzariu Alin100% (1)
- Nursing Skills Checklist - RTDocumento6 pagineNursing Skills Checklist - RTapi-309674272Nessuna valutazione finora
- Temu Ilmiah Reumatologi (TIR) 2023 - Perhimpunan Reumatologi IndonesiaDocumento1 paginaTemu Ilmiah Reumatologi (TIR) 2023 - Perhimpunan Reumatologi IndonesiabelanjayukdiNessuna valutazione finora
- TB PosterDocumento1 paginaTB PosterSucie 1997Nessuna valutazione finora
- Cellular Aberrations Guide to Cancer DiagnosisDocumento5 pagineCellular Aberrations Guide to Cancer DiagnosisIrish Eunice Felix100% (1)
- EmekaDocumento17 pagineEmekamutiyasNessuna valutazione finora
- Pantoea Agglomerans - ADocumento9 paginePantoea Agglomerans - AmadelaineNessuna valutazione finora
- SENCHS Joins The Philippine Dengue AwarenessDocumento3 pagineSENCHS Joins The Philippine Dengue AwarenessFhikery ArdienteNessuna valutazione finora
- Asama PosterDocumento1 paginaAsama Postershuvojit moulikNessuna valutazione finora
- Staph Lecture MicrococcusDocumento30 pagineStaph Lecture Micrococcussophia salibaNessuna valutazione finora
- Eclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Documento20 pagineEclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Grigore PopaNessuna valutazione finora