Potrebbero piacerti anche
- Assignment 1Documento4 pagineAssignment 1mp1757100% (1)
- Nursing Head-to-Toe Assessment Cheat Sheet - Nurseslabs PDFDocumento7 pagineNursing Head-to-Toe Assessment Cheat Sheet - Nurseslabs PDFNyeweh Sia Yomba67% (15)
- 2019 CCS Exam PreparationDocumento2 pagine2019 CCS Exam PreparationKian GonzagaNessuna valutazione finora
- CPC Practice Exam 2018 Includes 150 Prac PDFDocumento3 pagineCPC Practice Exam 2018 Includes 150 Prac PDFRakesh Ghare50% (2)
- Medical Language Immerse YourselfDocumento1.025 pagineMedical Language Immerse YourselfChristian TaillandierNessuna valutazione finora
- Ambulatory Payment Classifications (APCs)Documento44 pagineAmbulatory Payment Classifications (APCs)timvrghs123Nessuna valutazione finora
- HI 215 Purdue University Global Payment and Reimbursement Process Case StudyDocumento2 pagineHI 215 Purdue University Global Payment and Reimbursement Process Case StudyAlejandro VeraNessuna valutazione finora
- Medical Coding PPT by Pooji 1Documento9 pagineMedical Coding PPT by Pooji 1babupandu925Nessuna valutazione finora
- ICD-9-CM To ICD-10 Common Codes For Cardiovascular Disease: A Quick Reference For Quest Diagnostics ClientsDocumento1 paginaICD-9-CM To ICD-10 Common Codes For Cardiovascular Disease: A Quick Reference For Quest Diagnostics Clientssyaiful rinantoNessuna valutazione finora
- Unusual Presentation of May-Thurner SyndromeDocumento5 pagineUnusual Presentation of May-Thurner SyndromeJ. Ruben HermannNessuna valutazione finora
- ICL-Coding Operative ReportDocumento33 pagineICL-Coding Operative ReportHIMOfficial100% (2)
- Principles of Healthcare Reimbursement: Sixth EditionDocumento28 paginePrinciples of Healthcare Reimbursement: Sixth EditionDestiny Hayes100% (2)
- Drug Therapy Requiring Intensive Monitoring For ToxicityDocumento1 paginaDrug Therapy Requiring Intensive Monitoring For ToxicityadllurikaushikNessuna valutazione finora
- Medical Billing & Insurance Coding: Unlocking The Mystery of CPT CodingDocumento22 pagineMedical Billing & Insurance Coding: Unlocking The Mystery of CPT CodingAjay IyerNessuna valutazione finora
- Medical Coding SpecialistDocumento2 pagineMedical Coding SpecialistRoney Raju PhilipNessuna valutazione finora
- Anesthesia CPT CodesDocumento2 pagineAnesthesia CPT CodesSundarajan ManiNessuna valutazione finora
- HCC Coding Feb 2022 ICD-10 InformantDocumento2 pagineHCC Coding Feb 2022 ICD-10 InformantSonali PawarNessuna valutazione finora
- Dane Sultzer, OD: Condition CPT Codes Imaging/Procedure Codes Consider CommentsDocumento1 paginaDane Sultzer, OD: Condition CPT Codes Imaging/Procedure Codes Consider CommentsMaharNadirAliNessuna valutazione finora
- CPT 2023 Further Refines E - M Coding - AAPC Knowledge CenterDocumento5 pagineCPT 2023 Further Refines E - M Coding - AAPC Knowledge CenterKittu ReddyNessuna valutazione finora
- HCPro Inc., Adrianne E. Avillion DEd RN Reviewer ICD-10 Competency Assessment For Coders Anatomy and PhysiologyDocumento54 pagineHCPro Inc., Adrianne E. Avillion DEd RN Reviewer ICD-10 Competency Assessment For Coders Anatomy and PhysiologyamruthkiranbabujiNessuna valutazione finora
- PDFDocumento55 paginePDFJasliya Ismail100% (1)
- Medical Terminology On CPC Exam2 - YouTubeDocumento2 pagineMedical Terminology On CPC Exam2 - YouTubedgina8800Nessuna valutazione finora
- Coding For Medical Home VisitsDocumento14 pagineCoding For Medical Home VisitsSicColoNessuna valutazione finora
- DRG Overview of All Patient Refined Diagostic Related GroupsDocumento42 pagineDRG Overview of All Patient Refined Diagostic Related Groupsjaypee pengNessuna valutazione finora
- Ch06 IntroductionToCPTDocumento84 pagineCh06 IntroductionToCPTagnaveenanNessuna valutazione finora
- A Quarterly Publication of The Central Office On ICD-10-CM/PCSDocumento34 pagineA Quarterly Publication of The Central Office On ICD-10-CM/PCSharu haroonNessuna valutazione finora
- CRC Coding Boot Camp 2019 FINALDocumento2 pagineCRC Coding Boot Camp 2019 FINALRuban Kumar0% (1)
- Clinica Coading PlanDocumento13 pagineClinica Coading PlanNagib OtaybiNessuna valutazione finora
- Derm CodingDocumento8 pagineDerm CodingVinay100% (1)
- CPC H Preparation Course Syllabus 2011-11-10 1Documento3 pagineCPC H Preparation Course Syllabus 2011-11-10 1blac_xeroNessuna valutazione finora
- Icd 10 FinalDocumento7 pagineIcd 10 Finalanto_prapNessuna valutazione finora
- Medical Coding SpecialistDocumento3 pagineMedical Coding Specialistapi-789518410% (1)
- Medical Terminology Test - KeyDocumento8 pagineMedical Terminology Test - KeyAnonymous MtKJkerbpUNessuna valutazione finora
- American Dictations GastroDocumento15 pagineAmerican Dictations GastroSaru BashaNessuna valutazione finora
- Icd 10Documento4 pagineIcd 10Radhika ShahNessuna valutazione finora
- MBC Cover Letter N Resume JyapjyapDocumento3 pagineMBC Cover Letter N Resume Jyapjyapapi-397923551Nessuna valutazione finora
- Seronegative Myasthenia Gravis Presenting With PneumoniaDocumento4 pagineSeronegative Myasthenia Gravis Presenting With PneumoniaJ. Ruben HermannNessuna valutazione finora
- Medicine PDFDocumento385 pagineMedicine PDFMaheshNessuna valutazione finora
- Evaluation & Management CodingDocumento14 pagineEvaluation & Management Codingsherrij1025Nessuna valutazione finora
- E/M: Physical Examination CodingDocumento29 pagineE/M: Physical Examination CodingSupercoderNessuna valutazione finora
- CPC - Certified Professional CoderDocumento2 pagineCPC - Certified Professional Codershamlee PNessuna valutazione finora
- Chapter 6 Coding and Billing Basics PDFDocumento33 pagineChapter 6 Coding and Billing Basics PDFamruthkiranbabujiNessuna valutazione finora
- Why Coding Is ImportantDocumento35 pagineWhy Coding Is ImportantKholylah Afifah Nur RangkutiNessuna valutazione finora
- Coding Clinic 2nd QTR 2021Documento24 pagineCoding Clinic 2nd QTR 2021haru haroon100% (1)
- HSMN Healthcare Payment MethodologiesDocumento20 pagineHSMN Healthcare Payment MethodologiesMarvin Whitfield100% (1)
- Medical CodingDocumento7 pagineMedical CodingRaj DhotreNessuna valutazione finora
- 2021 Evaluation and Management Summary: New Patient VisitsDocumento2 pagine2021 Evaluation and Management Summary: New Patient Visitsmedical coding100% (1)
- 9 Key Radiology Medical Coding Tips For CodersDocumento4 pagine9 Key Radiology Medical Coding Tips For Codersayesha100% (1)
- Ahima ExamplesDocumento3 pagineAhima ExamplesNerry WasawordNessuna valutazione finora
- Medical Coder / BillerDocumento1 paginaMedical Coder / Billerapi-77384278Nessuna valutazione finora
- CPT Modifier NewDocumento10 pagineCPT Modifier NewSeenuvasanLeeManiNessuna valutazione finora
- Risk Adjustment Coding PDFDocumento38 pagineRisk Adjustment Coding PDFGordana Puzovic100% (2)
- HITT 2335 Abstracting-Coding RecordsDocumento15 pagineHITT 2335 Abstracting-Coding RecordsMatthew Fleck100% (1)
- Practical Exam CPCDocumento15 paginePractical Exam CPCkingNessuna valutazione finora
- Coding Cardiac CatheterizationsDocumento4 pagineCoding Cardiac Catheterizationsapi-270110430Nessuna valutazione finora
- Hcpcs Codes LVL 2Documento1 paginaHcpcs Codes LVL 2baskarjoNessuna valutazione finora
- Medical Coding SummaryDocumento5 pagineMedical Coding SummaryYhanie De GuzmanNessuna valutazione finora
- I10 2022 Coding GuidelinesDocumento34 pagineI10 2022 Coding GuidelinesagnaveenanNessuna valutazione finora
- Coder or CPC or Billing or HCC Risk or Trainer or EHR TrainerDocumento3 pagineCoder or CPC or Billing or HCC Risk or Trainer or EHR Trainerapi-78205606Nessuna valutazione finora
- Health Record Technician I: Passbooks Study GuideDa EverandHealth Record Technician I: Passbooks Study GuideNessuna valutazione finora
- Robbins Ch. 19 The Pancreas Review QuestionsDocumento3 pagineRobbins Ch. 19 The Pancreas Review QuestionsPA2014100% (1)
- Dapus Laprak Histologi Sistem DigestiDocumento2 pagineDapus Laprak Histologi Sistem DigestiAzizahNessuna valutazione finora
- Physical Assessment of Normal Pregnant ClientDocumento24 paginePhysical Assessment of Normal Pregnant ClientGhilah MaeNessuna valutazione finora
- DR CertificateDocumento1 paginaDR CertificateSusovan SirNessuna valutazione finora
- Reflexes in The GutDocumento2 pagineReflexes in The GutJeffrey TseNessuna valutazione finora
- Complications of CholelithiasisDocumento25 pagineComplications of CholelithiasisGibson RamseyNessuna valutazione finora
- Bagan KolestasisDocumento1 paginaBagan KolestasisSoma SkaNessuna valutazione finora
- Bio 22 Post-Lab - The Muscular System (New Ver.)Documento33 pagineBio 22 Post-Lab - The Muscular System (New Ver.)Arah Sacdalan92% (12)
- Approach To Liver Disease, Liver Function Tests, HyperbilirubinemiaDocumento34 pagineApproach To Liver Disease, Liver Function Tests, HyperbilirubinemiaKenneth NuñezNessuna valutazione finora
- Materi Anatomi DR ElieserDocumento49 pagineMateri Anatomi DR ElieserAbhauasjsjjjNessuna valutazione finora
- FicatulDocumento107 pagineFicatulkoxNessuna valutazione finora
- Biliary SecretionDocumento29 pagineBiliary Secretionkio josephNessuna valutazione finora
- Medicine Abdomen IappDocumento2 pagineMedicine Abdomen IappJudrelle Krizia MarianoNessuna valutazione finora
- I. Similar To Rounded Abdomen Only Greater. Anticipated in Pregnancy, Also Seen in Obesity, Ascites, and Other Conditions IIDocumento3 pagineI. Similar To Rounded Abdomen Only Greater. Anticipated in Pregnancy, Also Seen in Obesity, Ascites, and Other Conditions IIroxanneNessuna valutazione finora
- Endodermal Derivatives, Formation of The Gut and Its Subsequent RotationDocumento14 pagineEndodermal Derivatives, Formation of The Gut and Its Subsequent RotationmikeNessuna valutazione finora
- Abdominal Pain in Physical Therapy Practice PDFDocumento12 pagineAbdominal Pain in Physical Therapy Practice PDFdanielNessuna valutazione finora
- Abdomen Anatomy PDFDocumento53 pagineAbdomen Anatomy PDFKirk CobainNessuna valutazione finora
- Anatomi Blok 9Documento2 pagineAnatomi Blok 9Grace RaveenaNessuna valutazione finora
- Lecture 3 GB Obstructive JaundiceDocumento39 pagineLecture 3 GB Obstructive JaundiceEkaterina TitovaNessuna valutazione finora
- Annisa Setyadi - 22010114130157 Lab 3Documento4 pagineAnnisa Setyadi - 22010114130157 Lab 3trifamonika23Nessuna valutazione finora
- Stability: P. Ratan Khuman M.P.T. (Ortho & Sports)Documento56 pagineStability: P. Ratan Khuman M.P.T. (Ortho & Sports)Diogo BarrosNessuna valutazione finora
- Metabolism (Ncm-216)Documento10 pagineMetabolism (Ncm-216)Sofronio OmboyNessuna valutazione finora
- PhysioEx Exercise 9 Activity 6Documento4 paginePhysioEx Exercise 9 Activity 6MARILYN MARIANA HERNANDEZ MENDOZA100% (1)
- 2018 Management of Hepatitis BDocumento13 pagine2018 Management of Hepatitis BCamboy D' JablezNessuna valutazione finora
- Tips Vs BrtoDocumento11 pagineTips Vs BrtoCsiszár MártonNessuna valutazione finora
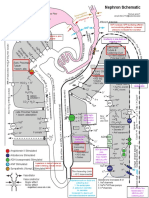
- NephronMap Copy2Documento1 paginaNephronMap Copy2Anonymous KxwaMDhANessuna valutazione finora
- Digestive System - Kelompok A4Documento102 pagineDigestive System - Kelompok A4Fathoni akbarNessuna valutazione finora
- Diagnostic LaparosDocumento11 pagineDiagnostic LaparosDr-Shadi MeteirNessuna valutazione finora