Potrebbero piacerti anche
- A Randomized, Double-Blind, Placebo-Controlled Study of Citalopram in Adolescents With Major Depressive Disorder - Von Knorring 2006Documento5 pagineA Randomized, Double-Blind, Placebo-Controlled Study of Citalopram in Adolescents With Major Depressive Disorder - Von Knorring 2006Julio JuarezNessuna valutazione finora
- Meta-Analyses of Statin Therapy For Primary Prevention Do Not Answer Key Questions: An Empirical Appraisal of 5 Years of Statin Meta-AnalysesDocumento8 pagineMeta-Analyses of Statin Therapy For Primary Prevention Do Not Answer Key Questions: An Empirical Appraisal of 5 Years of Statin Meta-AnalysesJulio JuarezNessuna valutazione finora
- Enhanced Vasculotoxic Metal Excretion in Post-Myocardial Infarction Patients Following A Single Edetate Disodium-Based Infusion - Arenas 2017Documento7 pagineEnhanced Vasculotoxic Metal Excretion in Post-Myocardial Infarction Patients Following A Single Edetate Disodium-Based Infusion - Arenas 2017Julio JuarezNessuna valutazione finora
- The Citalopram CIT-MD-18 Pediatric Depression Trial - Jureidini Et Al 2016Documento11 pagineThe Citalopram CIT-MD-18 Pediatric Depression Trial - Jureidini Et Al 2016Julio JuarezNessuna valutazione finora
- Closed Financial Loops: When They Happen in Government, They're Called Corruption in Medicine, They're Just A Footnote - Dejesus Morales 2017Documento6 pagineClosed Financial Loops: When They Happen in Government, They're Called Corruption in Medicine, They're Just A Footnote - Dejesus Morales 2017Julio JuarezNessuna valutazione finora
- Energy Expenditure at Rest and During ExerciseDocumento10 pagineEnergy Expenditure at Rest and During ExerciseJulio JuarezNessuna valutazione finora
- Ernst 2012Documento1 paginaErnst 2012Julio JuarezNessuna valutazione finora
- Oronowicz-Jaśkowiak 2019 PDFDocumento8 pagineOronowicz-Jaśkowiak 2019 PDFJulio JuarezNessuna valutazione finora
- On Holy Cows and Golden Calves (In Psychiatry) - Van Praag 2003Documento4 pagineOn Holy Cows and Golden Calves (In Psychiatry) - Van Praag 2003Julio JuarezNessuna valutazione finora
- Effect of Exercise Augmentation of Cognitive Behavioural Therapy For The Treatment of Suicidal Ideation and Depression - Abdollahi 2017Documento18 pagineEffect of Exercise Augmentation of Cognitive Behavioural Therapy For The Treatment of Suicidal Ideation and Depression - Abdollahi 2017Julio JuarezNessuna valutazione finora
- Empirically Derived Criteria Cast Doubt On The Clinical Significance of Antidepressant-Placebo Differences - Moncrieff & Kirsch 2015Documento3 pagineEmpirically Derived Criteria Cast Doubt On The Clinical Significance of Antidepressant-Placebo Differences - Moncrieff & Kirsch 2015Julio JuarezNessuna valutazione finora
- Banning Mercury AmalgamDocumento16 pagineBanning Mercury AmalgamJulio JuarezNessuna valutazione finora
- A Regulatory Apologia-A Review of Placebo-Controlled Studies in Regulatory Submissions of New-Generation Antidepressants - Melander 2008Documento5 pagineA Regulatory Apologia-A Review of Placebo-Controlled Studies in Regulatory Submissions of New-Generation Antidepressants - Melander 2008Julio JuarezNessuna valutazione finora
- Initial Severity and Antidepressant Benefits: A Meta-Analysis of Data Submitted To The Food and Drug Administration - Kirsch 2008Documento9 pagineInitial Severity and Antidepressant Benefits: A Meta-Analysis of Data Submitted To The Food and Drug Administration - Kirsch 2008Julio JuarezNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Journal SeptemberDocumento36 pagineJournal Septemberramkumarm05Nessuna valutazione finora
- Anti ParkinsonDocumento38 pagineAnti Parkinsonarif khalidNessuna valutazione finora
- Pharmacy Board ExamDocumento2 paginePharmacy Board ExamRhealyn LegaspiNessuna valutazione finora
- Chemo Stability Chart - AtoKDocumento59 pagineChemo Stability Chart - AtoKAfifah Nur Diana PutriNessuna valutazione finora
- Pharmacoepidemiology: Pinar Yalcin Balcik, Gulcan KahramanDocumento6 paginePharmacoepidemiology: Pinar Yalcin Balcik, Gulcan KahramandebbyirmaNessuna valutazione finora
- PropofolDocumento3 paginePropofolamelwd100% (1)
- Phenytoin Sodium 50 MG Film-Coated Tablets (Phenytoin Sodium) PL 16363/0253Documento17 paginePhenytoin Sodium 50 MG Film-Coated Tablets (Phenytoin Sodium) PL 16363/0253Mohammed shamiul ShahidNessuna valutazione finora
- ENDOTRACHEAL INTUBATIOn SandeepDocumento17 pagineENDOTRACHEAL INTUBATIOn SandeepSimran JosanNessuna valutazione finora
- FDA Recall NoticeDocumento3 pagineFDA Recall NoticeAnonymous Pb39klJNessuna valutazione finora
- Pharma Drug SufficesDocumento3 paginePharma Drug SufficesJillian GayleNessuna valutazione finora
- Ellex Glaucoma BrochureDocumento12 pagineEllex Glaucoma BrochureHaag-Streit UK (HS-UK)Nessuna valutazione finora
- BetahistinDocumento2 pagineBetahistinThuc TranNessuna valutazione finora
- BOTOXDocumento12 pagineBOTOXJanani KrishnanNessuna valutazione finora
- Drug Study AssignmentDocumento1 paginaDrug Study AssignmentDaniela Claire FranciscoNessuna valutazione finora
- Behavioral Psychosis in DementiaDocumento62 pagineBehavioral Psychosis in DementiaAlexander NavarraNessuna valutazione finora
- Med GuideDocumento7 pagineMed GuideEko YuliantoNessuna valutazione finora
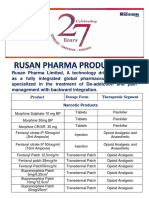
- Rusan Pharma Product ListDocumento4 pagineRusan Pharma Product ListSanjay SharmaNessuna valutazione finora
- Package Leaflet: Information For The User: Lidocaine 9.6% W.WDocumento2 paginePackage Leaflet: Information For The User: Lidocaine 9.6% W.WPankaj RadadiyaNessuna valutazione finora
- Cataract Surgery ProtocolsDocumento17 pagineCataract Surgery ProtocolsRahul ShastriNessuna valutazione finora
- Improvement of Opioid Addiction Medication Through Extended-Release Naltrexone: A Comparative, Experimental and Laboratory ApproachDocumento3 pagineImprovement of Opioid Addiction Medication Through Extended-Release Naltrexone: A Comparative, Experimental and Laboratory ApproachMediterr J Pharm Pharm SciNessuna valutazione finora
- Important Information: A Patient's Guide To Treating Premature Ejaculation With PRILIGY (Dapoxetine)Documento9 pagineImportant Information: A Patient's Guide To Treating Premature Ejaculation With PRILIGY (Dapoxetine)Sahil VijanNessuna valutazione finora
- Hypnotism - L. W. de LaurenceDocumento195 pagineHypnotism - L. W. de LaurenceGrantNessuna valutazione finora
- Skeletal Muscle Relaxants: Kenneth C. Jackson, II Charles E. Argoff Andrew DubinDocumento1 paginaSkeletal Muscle Relaxants: Kenneth C. Jackson, II Charles E. Argoff Andrew DubinFaith Acu CureNessuna valutazione finora
- Endotracheal IntubationDocumento4 pagineEndotracheal Intubationrupali gahalianNessuna valutazione finora
- General AnesthesiaDocumento6 pagineGeneral AnesthesiaTaqi MehdiNessuna valutazione finora
- UVU - NURS 2430 - Unit III - Ch. 12: Introduction To Psychiatric DrugsDocumento2 pagineUVU - NURS 2430 - Unit III - Ch. 12: Introduction To Psychiatric Drugsisapatrick8126Nessuna valutazione finora
- Sachin Kumar CV Updated On 01-05-2014Documento5 pagineSachin Kumar CV Updated On 01-05-2014Sachin Kumar PrajapatiNessuna valutazione finora
- StimulantsDocumento4 pagineStimulantsLinh-Trang NguyenNessuna valutazione finora
- Pain ManagementDocumento21 paginePain ManagementTedi SunandarNessuna valutazione finora
- Crash CartDocumento2 pagineCrash CartMenGuitarNessuna valutazione finora