Potrebbero piacerti anche
- SerotoninDocumento6 pagineSerotoninghinsavitNessuna valutazione finora
- Charts For PharmacologyDocumento3 pagineCharts For PharmacologyAditi100% (1)
- Renal Drug EliminationDocumento43 pagineRenal Drug Eliminationshoaibar100% (1)
- High Performance Liquid Chromatography: Prepared By, S.R.Yadav Assistant ProfessorDocumento32 pagineHigh Performance Liquid Chromatography: Prepared By, S.R.Yadav Assistant ProfessorShweta Yadav100% (1)
- Fluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceDa EverandFluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceValutazione: 5 su 5 stelle5/5 (2)
- Administration of MedicationsDocumento11 pagineAdministration of MedicationsAsma Saleem100% (1)
- Poisoning and Drug OverdoseDocumento95 paginePoisoning and Drug OverdoseMohammed Younis Shaheen100% (2)
- Body FluidsDocumento38 pagineBody FluidsGift AiyegbeniNessuna valutazione finora
- Air Handling Systems: Eating Entilation and Ir OnditioningDocumento24 pagineAir Handling Systems: Eating Entilation and Ir OnditioningVidyaNessuna valutazione finora
- Physiology lab: Faculty of Medical laboratory since Patch 7 ليعامسإ دمحم اللهدبع مكوخأ صيخلتDocumento32 paginePhysiology lab: Faculty of Medical laboratory since Patch 7 ليعامسإ دمحم اللهدبع مكوخأ صيخلتmohammedNessuna valutazione finora
- Compilation of Community Procedures in Inspections and Exchange of InformationDocumento6 pagineCompilation of Community Procedures in Inspections and Exchange of InformationDaoNessuna valutazione finora
- Alert Medical Series: Emergency Medicine Alert IIIDa EverandAlert Medical Series: Emergency Medicine Alert IIINessuna valutazione finora
- Renal Tubular Acidosis: Moderator:Dr Nitin Joshi Presented By: Dr. Parth Nathwani MGM Medical College, MumbaiDocumento71 pagineRenal Tubular Acidosis: Moderator:Dr Nitin Joshi Presented By: Dr. Parth Nathwani MGM Medical College, MumbaiariNessuna valutazione finora
- Contamination Control in Cleanrooms - TexwipeDocumento43 pagineContamination Control in Cleanrooms - TexwipeKristian Uriel DelgadoNessuna valutazione finora
- Excretion (Dr. Imran Ashraf)Documento44 pagineExcretion (Dr. Imran Ashraf)Abdul WahabNessuna valutazione finora
- Learning Objectives:: Gas Form Lipid-Soluble Substances Water-Soluble SubstancesDocumento12 pagineLearning Objectives:: Gas Form Lipid-Soluble Substances Water-Soluble SubstancesRose Andrea De los SantosNessuna valutazione finora
- Fattori Fisiologici Legati All'assorbimento Dei FarmaciDocumento24 pagineFattori Fisiologici Legati All'assorbimento Dei FarmaciStefano PorzioNessuna valutazione finora
- Principles of Renal Measurement 1 Measuring Renal Clearance and TransportDocumento21 paginePrinciples of Renal Measurement 1 Measuring Renal Clearance and TransportBayu Kxiikdx LskdNessuna valutazione finora
- Chapter 4 - Clearance - FCCU - SP22Documento32 pagineChapter 4 - Clearance - FCCU - SP22Patras BhattiNessuna valutazione finora
- 02 - Body Fluids 2021Documento33 pagine02 - Body Fluids 2021shabnam sajidaNessuna valutazione finora
- Pharmacology-I Chapter-1 of 2Documento48 paginePharmacology-I Chapter-1 of 2No NameNessuna valutazione finora
- Acidity and Basicity of DrugsDocumento49 pagineAcidity and Basicity of DrugsNguyễn Hoàng ViệtNessuna valutazione finora
- Excretion of Drugs: Dr. G.SAILAJA, M.Pharm - PH.D., Assoc. Professor, Dept. of PharmaceuticsDocumento43 pagineExcretion of Drugs: Dr. G.SAILAJA, M.Pharm - PH.D., Assoc. Professor, Dept. of PharmaceuticsSailaja Reddy GunnamNessuna valutazione finora
- Renal Glucose and Acid Base BalanceDocumento18 pagineRenal Glucose and Acid Base BalanceAgasi MkNessuna valutazione finora
- Pysiology Team Part 1 For Mide Exam (LECTURES: 1,2,3,4,5)Documento24 paginePysiology Team Part 1 For Mide Exam (LECTURES: 1,2,3,4,5)Aboalez NopliumNessuna valutazione finora
- ELIMINATIONDocumento22 pagineELIMINATIONprashil charkariNessuna valutazione finora
- Lecture 8Documento8 pagineLecture 8Hilary ChuiNessuna valutazione finora
- L8-IV FluidsDocumento41 pagineL8-IV FluidsKrishna RajakumarNessuna valutazione finora
- Drug Absorption: - Absorption Is The Process byDocumento57 pagineDrug Absorption: - Absorption Is The Process byccccccc1Nessuna valutazione finora
- Absorption and Half-Life: Nick HolfordDocumento4 pagineAbsorption and Half-Life: Nick HolfordNurAfifahNessuna valutazione finora
- Excretion and Elimination KineticsDocumento39 pagineExcretion and Elimination KineticsYashasv BhatnagarNessuna valutazione finora
- Excretion Biotransformation Metabolism: Dr. AA Yas Drug Elimination and Clearance Drug EliminationDocumento31 pagineExcretion Biotransformation Metabolism: Dr. AA Yas Drug Elimination and Clearance Drug EliminationMohannad AlfadhalNessuna valutazione finora
- General PharmacologyDocumento13 pagineGeneral Pharmacologymalkalhmaidh03Nessuna valutazione finora
- Physiology, Lecture 4, Body Fluids and Blood (Lecture Notes)Documento17 paginePhysiology, Lecture 4, Body Fluids and Blood (Lecture Notes)Ali Al-Qudsi100% (5)
- Physiology Course: Dr. Velu M. RachelDocumento40 paginePhysiology Course: Dr. Velu M. RachelKunda JosephNessuna valutazione finora
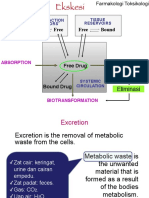
- Materi Fartok EkskresiDocumento34 pagineMateri Fartok EkskresiOskarHowayNessuna valutazione finora
- 2022 Lecture 4 Body Fluids Compartments Na K 1 3Documento49 pagine2022 Lecture 4 Body Fluids Compartments Na K 1 3Mariam ShenoudaNessuna valutazione finora
- Excretion of DrugsDocumento78 pagineExcretion of DrugsSohan PrasathNessuna valutazione finora
- Pharmacokinetics 1Documento34 paginePharmacokinetics 1Ebenezer SamuelNessuna valutazione finora
- ExcretionDocumento35 pagineExcretionHely PatelNessuna valutazione finora
- Pharmacokinetics: DR Narendra KumarDocumento60 paginePharmacokinetics: DR Narendra Kumarperala vinaykumarNessuna valutazione finora
- Body Water and Fluid CompartmentsDocumento44 pagineBody Water and Fluid CompartmentsMatende husseinNessuna valutazione finora
- Non Invasive Methods of Estimating Pharmacokinetic Parameters2Documento31 pagineNon Invasive Methods of Estimating Pharmacokinetic Parameters2Thilak Chandra50% (2)
- Urine FormationDocumento49 pagineUrine FormationMajd HusseinNessuna valutazione finora
- Renal Physiology 1Documento9 pagineRenal Physiology 1Anny AlvrzNessuna valutazione finora
- Renal Physiology LatestDocumento63 pagineRenal Physiology LatestRaudzah RamliNessuna valutazione finora
- PHARMACOLOGY (Basic Pharmacology-ANS-Endocrine)Documento23 paginePHARMACOLOGY (Basic Pharmacology-ANS-Endocrine)Famela Anne GOmez MadambaNessuna valutazione finora
- PHARMACOKINETICS & PharmacokineticsDocumento60 paginePHARMACOKINETICS & PharmacokineticsRaj PathakNessuna valutazione finora
- 1 - Renal Excretion of DrugsDocumento18 pagine1 - Renal Excretion of DrugsKashar SaeedNessuna valutazione finora
- PHA612 Experiment 11 Lab Report 1 PDFDocumento3 paginePHA612 Experiment 11 Lab Report 1 PDFkirstenshayne.maningas.pharmaNessuna valutazione finora
- Body Fluid CompartmenBDSDocumento17 pagineBody Fluid CompartmenBDSHimani JhaNessuna valutazione finora
- WaterDocumento6 pagineWaterRichard PoonNessuna valutazione finora
- (PHYSIO B) 1.2 Renal Physio Pt. 3Documento8 pagine(PHYSIO B) 1.2 Renal Physio Pt. 3miguel cuevasNessuna valutazione finora
- Pharmacokinetics - Part 1 - : W.M. TomDocumento55 paginePharmacokinetics - Part 1 - : W.M. TomLs Tamil editzzNessuna valutazione finora
- 1997 Pharmacology Semester 1 Page 1 of 7Documento7 pagine1997 Pharmacology Semester 1 Page 1 of 7ravi2likeNessuna valutazione finora
- Revision FileDocumento14 pagineRevision FileBasema HashhashNessuna valutazione finora
- Body FluidsDocumento44 pagineBody FluidsO'Brien Alfred100% (1)
- Body Fluids 2022 StudentDocumento36 pagineBody Fluids 2022 Studentshavindrap2000Nessuna valutazione finora
- GC Acid Base and Electrolytes Apr 28 2013Documento31 pagineGC Acid Base and Electrolytes Apr 28 2013Rainier Kyle AlcantaraNessuna valutazione finora
- FLG 332 Renal Physiology-2 (2019)Documento27 pagineFLG 332 Renal Physiology-2 (2019)Huzaifa KhanNessuna valutazione finora
- PharmacokineticsDocumento47 paginePharmacokineticsْNessuna valutazione finora
- Drug Elimination in KidneyDocumento24 pagineDrug Elimination in KidneyRabail GalaniNessuna valutazione finora
- Perioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud UniversityDocumento47 paginePerioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud Universityarifjo7999Nessuna valutazione finora
- Drug TransportDocumento27 pagineDrug TransportYashasv BhatnagarNessuna valutazione finora
- Physiology. Hrd.Documento549 paginePhysiology. Hrd.Sʌɩĸʌt PʌʋɭNessuna valutazione finora
- 5 - GC Dan HPLCDocumento33 pagine5 - GC Dan HPLCDewi AnjaniNessuna valutazione finora
- More “Oomph,” Nature’s Plan for Human Physical Wellness Thru Metabolic TypingDa EverandMore “Oomph,” Nature’s Plan for Human Physical Wellness Thru Metabolic TypingNessuna valutazione finora
- Pharm 4 ADocumento3 paginePharm 4 Aravi2likeNessuna valutazione finora
- Pharm 4 CDocumento4 paginePharm 4 Cravi2likeNessuna valutazione finora
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Documento4 pagineBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2likeNessuna valutazione finora
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Documento4 pagineBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2likeNessuna valutazione finora
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Documento4 pagineBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2likeNessuna valutazione finora
- Pharm 3 IDocumento3 paginePharm 3 Iravi2like100% (1)
- By Duy Thai, 1997: Choline AcetyltransferaseDocumento4 pagineBy Duy Thai, 1997: Choline Acetyltransferaseravi2likeNessuna valutazione finora
- Stimulates Ca ") .: 1997 Pharmacology Semester 1 Page 1 of 6Documento6 pagineStimulates Ca ") .: 1997 Pharmacology Semester 1 Page 1 of 6ravi2likeNessuna valutazione finora
- Pharm 3 eDocumento3 paginePharm 3 eravi2likeNessuna valutazione finora
- Pharm 3 BDocumento3 paginePharm 3 Bravi2likeNessuna valutazione finora
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Documento4 pagineBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2likeNessuna valutazione finora
- Pharm 3 CDocumento3 paginePharm 3 Cravi2likeNessuna valutazione finora
- By Duy Thai, 1997: Diffuse Out of Nerve Terminal and Act On COMPT in External TissuesDocumento5 pagineBy Duy Thai, 1997: Diffuse Out of Nerve Terminal and Act On COMPT in External Tissuesravi2likeNessuna valutazione finora
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 5Documento5 pagineBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 5ravi2likeNessuna valutazione finora
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Documento4 pagineBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2like100% (2)
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 6Documento6 pagineBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 6ravi2likeNessuna valutazione finora
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Documento4 pagineBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2likeNessuna valutazione finora
- Anti Inflammatory Drugs, by Duy Thai, 1997Documento4 pagineAnti Inflammatory Drugs, by Duy Thai, 1997ghinsavitNessuna valutazione finora
- Pharm 1 HDocumento6 paginePharm 1 Hravi2likeNessuna valutazione finora
- 1997 Pharmacology Semester 1 Page 1 of 6Documento6 pagine1997 Pharmacology Semester 1 Page 1 of 6ravi2likeNessuna valutazione finora
- Aspirin Irreversibly Inhibits Cyclo-Oxygenase: Pharmacology Semester 1 Page 1 of 5Documento6 pagineAspirin Irreversibly Inhibits Cyclo-Oxygenase: Pharmacology Semester 1 Page 1 of 5ravi2likeNessuna valutazione finora
- E Valency Ion Ion: A - Ve Value Means A Net Flow Into The CellDocumento5 pagineE Valency Ion Ion: A - Ve Value Means A Net Flow Into The Cellravi2likeNessuna valutazione finora
- 1997 Pharmacology Semester 1 Page 1 of 7Documento7 pagine1997 Pharmacology Semester 1 Page 1 of 7ravi2likeNessuna valutazione finora
- Drug AbsorptionDocumento3 pagineDrug AbsorptionTania HenriquezNessuna valutazione finora
- Presence of An Antagonist.: Pharmacology Semester 1 Page 1 of 5Documento5 paginePresence of An Antagonist.: Pharmacology Semester 1 Page 1 of 5ravi2like100% (1)
- Pharm 1 GDocumento3 paginePharm 1 Gravi2likeNessuna valutazione finora
- Pharm 1 eDocumento3 paginePharm 1 eravi2likeNessuna valutazione finora
- 1997 Pharmacology Semester 1 Page 1 of 4Documento4 pagine1997 Pharmacology Semester 1 Page 1 of 4ravi2like100% (1)
- NICE GuidelineDocumento30 pagineNICE GuidelineRalucaNessuna valutazione finora
- DiliDocumento25 pagineDiliSenarathKuleeshaKodisingheNessuna valutazione finora
- Annotated BibliographyDocumento4 pagineAnnotated Bibliographyapi-447388856Nessuna valutazione finora
- Medication OrderDocumento16 pagineMedication OrderAnonymous whcvnPBeQNessuna valutazione finora
- Tele Guide MDocumento3 pagineTele Guide MAamaar ShahorNessuna valutazione finora
- SynthesisDocumento72 pagineSynthesisОливера СтојковићNessuna valutazione finora
- Medikolegal Pengobatan Untuk Diri Sendiri (Swamedikasi) Sebagai Upaya Menyembuhkan PenyakitDocumento8 pagineMedikolegal Pengobatan Untuk Diri Sendiri (Swamedikasi) Sebagai Upaya Menyembuhkan PenyakitMiftahul JannahNessuna valutazione finora
- Missing Women Revisited by Amartya SenDocumento2 pagineMissing Women Revisited by Amartya SenDebashish BoseNessuna valutazione finora
- Vivitrol Medication GuideDocumento6 pagineVivitrol Medication GuidemrboredguyNessuna valutazione finora
- Aga Spring 2015 PDFDocumento900 pagineAga Spring 2015 PDFMuhammad Israr Ul HaqNessuna valutazione finora
- M/d/y Maintenance Meds Antibiotics Fluids Other Notes 2/1/16 - 2/12/16Documento4 pagineM/d/y Maintenance Meds Antibiotics Fluids Other Notes 2/1/16 - 2/12/16irineNessuna valutazione finora
- Materi Ibu Difa - Pelayanan ResepDocumento18 pagineMateri Ibu Difa - Pelayanan ResepCang HaedarNessuna valutazione finora
- CATALOGOAGOSTO2020Documento531 pagineCATALOGOAGOSTO2020GioCoronel100% (1)
- Unit1 DrRakhiMishra (2) CNPDocumento107 pagineUnit1 DrRakhiMishra (2) CNPAnkit Kumar VermaNessuna valutazione finora
- Drug Study ValiumDocumento4 pagineDrug Study ValiumEric EvangelistaNessuna valutazione finora
- Anti DepressantDocumento6 pagineAnti Depressantyahyaahmed152000Nessuna valutazione finora
- BIOPHARMACEUTICSDocumento132 pagineBIOPHARMACEUTICSTahaniNessuna valutazione finora
- 1 - General AnestheticsDocumento2 pagine1 - General AnestheticsChinenye AkwueNessuna valutazione finora
- MALPRACTICEDocumento43 pagineMALPRACTICEDev LitaNessuna valutazione finora
- Worthless Without Coffee - NMIMS MumbaiDocumento7 pagineWorthless Without Coffee - NMIMS MumbaiARPAN DHARNessuna valutazione finora
- Northern Nevada Certified Medical Marijuana DispensariesDocumento2 pagineNorthern Nevada Certified Medical Marijuana DispensariesEd KeatingNessuna valutazione finora
- Merck Sharp & Dohme Argentina, Inc. (A) : Business PolicyDocumento3 pagineMerck Sharp & Dohme Argentina, Inc. (A) : Business PolicyhashimhashNessuna valutazione finora
- Numericals AssignmentDocumento2 pagineNumericals AssignmentAiman SiddiquiNessuna valutazione finora
- Pharmacognostic Standardization of Bombax Costatum Pellegr and Vuillet Stem Bark (Bombacaceae)Documento7 paginePharmacognostic Standardization of Bombax Costatum Pellegr and Vuillet Stem Bark (Bombacaceae)Ayeni EmmanuelNessuna valutazione finora