Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- TBL 1 - Refractive Error SlidesDocumento66 pagineTBL 1 - Refractive Error SlidesAmirah Azman100% (4)
- LAMINECTOMYDocumento22 pagineLAMINECTOMYPatricia CaladoNessuna valutazione finora
- Expert DDX ChestDocumento1.053 pagineExpert DDX ChestClaudio Rodriguez100% (1)
- Poster PresentationsDocumento3 paginePoster PresentationsdocbinNessuna valutazione finora
- Anesthesia Anesthetic DrugsDocumento6 pagineAnesthesia Anesthetic DrugsYesi SaputriNessuna valutazione finora
- Chapter 7Documento7 pagineChapter 7Mia Kristhyn Calinawagan SabanalNessuna valutazione finora
- Review - Pelvic Nerves - From Anatomy and Physiology To Clinical ApplicationsDocumento17 pagineReview - Pelvic Nerves - From Anatomy and Physiology To Clinical ApplicationsNovi RobiyantiNessuna valutazione finora
- Mechanical Circulatory Support & Cardiothoracic Transplant: Friday 27 November 2020 Harefield HospitalDocumento1 paginaMechanical Circulatory Support & Cardiothoracic Transplant: Friday 27 November 2020 Harefield HospitalscudchssNessuna valutazione finora
- Phaco Machine Procedure PDFDocumento4 paginePhaco Machine Procedure PDFAlim SumonNessuna valutazione finora
- Module 2Documento10 pagineModule 2Renee Andrei Concepcion MozarNessuna valutazione finora
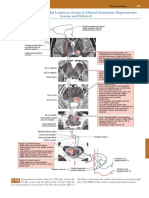
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDocumento1 paginaPosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNessuna valutazione finora
- 1411-Article Text-2128-1-10-20190318Documento65 pagine1411-Article Text-2128-1-10-20190318sagaNessuna valutazione finora
- Assisting The Patient During The Lumbar Puncture DefinitionDocumento3 pagineAssisting The Patient During The Lumbar Puncture DefinitionSHAINA CADALINNessuna valutazione finora
- PY 5.16: Record Arterial Pulse Tracing Using Finger Plethysmography in A Volunteer or Simulated EnvironmentDocumento6 paginePY 5.16: Record Arterial Pulse Tracing Using Finger Plethysmography in A Volunteer or Simulated EnvironmentADITYA SARAFNessuna valutazione finora
- Oral Surgery 2 FinalsDocumento32 pagineOral Surgery 2 FinalsKen HoiNessuna valutazione finora
- Physiology of One Lung Ventilation: Moderator-Dr. Nataraj Guide - Dr. Nagaraj Speaker - Dr. RohitDocumento59 paginePhysiology of One Lung Ventilation: Moderator-Dr. Nataraj Guide - Dr. Nagaraj Speaker - Dr. RohitPraveen RamasamyNessuna valutazione finora
- Cirugia Conceptos ActualesDocumento11 pagineCirugia Conceptos ActualesSinaivNessuna valutazione finora
- Cosmetic Derm PDFDocumento1.170 pagineCosmetic Derm PDFhesham100% (3)
- 2multiple Choice Questions in Internal MedicineDocumento15 pagine2multiple Choice Questions in Internal MedicineMEDS easyNessuna valutazione finora
- Surgical Diseases of The Pancreas and Biliary Tree (PDFDrive)Documento484 pagineSurgical Diseases of The Pancreas and Biliary Tree (PDFDrive)anovi_sky100% (1)
- Job Description of Operating Room Nurse in IndiaDocumento4 pagineJob Description of Operating Room Nurse in IndiaShine George100% (1)
- Gastrointestinal System DisordersDocumento112 pagineGastrointestinal System DisordersTaate MohammedNessuna valutazione finora
- High-Power Diode Laser Use On Fordyce Granule Excision: A Case ReportDocumento5 pagineHigh-Power Diode Laser Use On Fordyce Granule Excision: A Case ReportRisa SasmitaNessuna valutazione finora
- AuscultationDocumento41 pagineAuscultationAnonymous ZUaUz1wwNessuna valutazione finora
- Subbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansDocumento5 pagineSubbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansdoctorbanNessuna valutazione finora
- Postoperative Care: Prepare Ahead of TimeDocumento9 paginePostoperative Care: Prepare Ahead of Timewyclife akong'oNessuna valutazione finora
- Embryonal Remnants in The Testis and EpididymisDocumento9 pagineEmbryonal Remnants in The Testis and EpididymisKata TölgyesiNessuna valutazione finora
- Tatalaksana Dan Prognosis Tumor PeriampullarDocumento16 pagineTatalaksana Dan Prognosis Tumor PeriampullarVerico PratamaNessuna valutazione finora
- Malay, Age: 59 Years Old, Date of Admission: 18 August 2009 (CCU), 26 August 2009 (Ward 6B), Date of Clerking: 26 August 2009, Source ofDocumento8 pagineMalay, Age: 59 Years Old, Date of Admission: 18 August 2009 (CCU), 26 August 2009 (Ward 6B), Date of Clerking: 26 August 2009, Source ofAiman ArifinNessuna valutazione finora
- Aaron 800 - Eu AARON 900Documento60 pagineAaron 800 - Eu AARON 900Carlos Equipamiento M-h M-vNessuna valutazione finora