Potrebbero piacerti anche
- Electrolyte Repletion GuidelineDocumento6 pagineElectrolyte Repletion GuidelineIla MahiraNessuna valutazione finora
- Analgesics and SedativesDocumento2 pagineAnalgesics and SedativesdrchiNessuna valutazione finora
- Pre-Operative Orders Post-Op Orders (Ga)Documento3 paginePre-Operative Orders Post-Op Orders (Ga)Alissandra OcampoNessuna valutazione finora
- Electrolyte Repletion Guideline PMGDocumento4 pagineElectrolyte Repletion Guideline PMGHany ElbarougyNessuna valutazione finora
- Farmacos Reanimacion PediatricaDocumento1 paginaFarmacos Reanimacion PediatricaMiriam C. F. TapiaNessuna valutazione finora
- PICU drug therapy challenges and safe administrationDocumento32 paginePICU drug therapy challenges and safe administrationNeethu Mariya MathewNessuna valutazione finora
- Ped Med HandbookDocumento27 paginePed Med HandbookSoad Shedeed0% (1)
- Pediatric ER Standing Order ProtocolsDocumento2 paginePediatric ER Standing Order ProtocolsCharlene FernándezNessuna valutazione finora
- Upload 8Documento2 pagineUpload 8cingyaNessuna valutazione finora
- NICU Drugs GuideDocumento49 pagineNICU Drugs GuideArhanNessuna valutazione finora
- 2015 Pain Management For PediatricDocumento2 pagine2015 Pain Management For Pediatricdiany astutiNessuna valutazione finora
- RFH COVID-19 ICU Resource Pack FULL PDFDocumento15 pagineRFH COVID-19 ICU Resource Pack FULL PDFQuique GarciaNessuna valutazione finora
- Nomogram For Adjusting Unfractionated Heparin in Adults Using Anti-Factor Xa Activity or The aPTTDocumento2 pagineNomogram For Adjusting Unfractionated Heparin in Adults Using Anti-Factor Xa Activity or The aPTTLulwaNessuna valutazione finora
- Guidelines For Nurse Controlled and Patient Controlled Analgesia Morphine InfusionDocumento2 pagineGuidelines For Nurse Controlled and Patient Controlled Analgesia Morphine Infusionfinchan IrawanNessuna valutazione finora
- Intensive Care For ChildrenDocumento98 pagineIntensive Care For ChildrenTufail MemonNessuna valutazione finora
- TDM Practical Guide Part1Documento7 pagineTDM Practical Guide Part1Ahmedshaker21100% (1)
- Electrolyte ReplacementDocumento5 pagineElectrolyte Replacementtwo.risk100% (1)
- Quick Reference Guide Corrections 2021Documento6 pagineQuick Reference Guide Corrections 2021Prashin RocharamNessuna valutazione finora
- COVID MX BsmmuDocumento2 pagineCOVID MX BsmmuNuhiat NahreenNessuna valutazione finora
- SedationDocumento1 paginaSedationratnamalaramasamyNessuna valutazione finora
- Neonatal And Pediatric Drug DosageDocumento2 pagineNeonatal And Pediatric Drug Dosagebayan mohammedNessuna valutazione finora
- Notes in Neonates محمد ابراهيم مستشفى قوص قنا.WhiteKnightLoveDocumento77 pagineNotes in Neonates محمد ابراهيم مستشفى قوص قنا.WhiteKnightLoveMaRwa IbrahimNessuna valutazione finora
- Table 16-3 - Nonopioid AnalgesicsDocumento1 paginaTable 16-3 - Nonopioid AnalgesicsDragutin PetrićNessuna valutazione finora
- Adult Electrolyte Replacement Protocol - MCLN 0006 J PDFDocumento1 paginaAdult Electrolyte Replacement Protocol - MCLN 0006 J PDFCraigNessuna valutazione finora
- Antidote Card: Orogastric Lavage With Large Bore TubeDocumento2 pagineAntidote Card: Orogastric Lavage With Large Bore Tubemataro13Nessuna valutazione finora
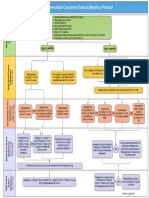
- CHAM Generalized Convulsive Status Epilepticus ProtocolDocumento1 paginaCHAM Generalized Convulsive Status Epilepticus Protocold'Agung NugrohoNessuna valutazione finora
- Picu NotesDocumento65 paginePicu NotesAhmed Mohammed100% (2)
- Condition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockDocumento4 pagineCondition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockJohnPaulOliverosNessuna valutazione finora
- Inpatient Electrolyte RepletionDocumento3 pagineInpatient Electrolyte Repletionapi-648757084Nessuna valutazione finora
- Contrast Reaction Card PediatricDocumento2 pagineContrast Reaction Card PediatricJenniffer FlorenciaNessuna valutazione finora
- Antibiotic ProtocolDocumento37 pagineAntibiotic ProtocolSrinivas VadtheNessuna valutazione finora
- Pediatric Guidelines For Medications PDFDocumento24 paginePediatric Guidelines For Medications PDFLaylatan NurNessuna valutazione finora
- Antibiotic Treatment Guidelines For Urinary Tract Infections in Children (60 Days Through 17 Years)Documento3 pagineAntibiotic Treatment Guidelines For Urinary Tract Infections in Children (60 Days Through 17 Years)Zahid AbbasNessuna valutazione finora
- Iv Infusions 6 Desired Dose (Mcg/Kg/Min) Desired Rate (ML/HR) WT (KG) MG Drug 100 ML FluidDocumento1 paginaIv Infusions 6 Desired Dose (Mcg/Kg/Min) Desired Rate (ML/HR) WT (KG) MG Drug 100 ML FluidHòa ThảoNessuna valutazione finora
- Commonly Prescribed Medications in Surgical Ed Sivakami Ver 5.0Documento23 pagineCommonly Prescribed Medications in Surgical Ed Sivakami Ver 5.0Suiweng WongNessuna valutazione finora
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Documento14 paginePaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniNessuna valutazione finora
- Dka CalculatorDocumento1 paginaDka CalculatordelfiaNessuna valutazione finora
- CalciumchannelalgorithmDocumento1 paginaCalciumchannelalgorithmLind YLNessuna valutazione finora
- Dopamine - IV AdministrationDocumento4 pagineDopamine - IV AdministrationAlexandra RainNessuna valutazione finora
- Central Nervous System InfectionsDocumento9 pagineCentral Nervous System InfectionsSaddamNessuna valutazione finora
- Fluid Therapy in Paediatrics - RevisedDocumento5 pagineFluid Therapy in Paediatrics - RevisedJehangir AllamNessuna valutazione finora
- ICE DrugsDocumento2 pagineICE DrugsRichelle FrondaNessuna valutazione finora
- Obtain 12 Lead ECG and Cardiology ConsultationDocumento2 pagineObtain 12 Lead ECG and Cardiology ConsultationPauline ChanNessuna valutazione finora
- ÷ Weight (KG) Dilute 1 ML (500mcg) of PGE1 With NS/ D5% To Yield The Total Volume From #1Documento14 pagine÷ Weight (KG) Dilute 1 ML (500mcg) of PGE1 With NS/ D5% To Yield The Total Volume From #1Nesreen G MohammedNessuna valutazione finora
- Recommended Anesthetic Agents for RabbitsDocumento1 paginaRecommended Anesthetic Agents for RabbitsRais RyuzakiNessuna valutazione finora
- PICU Drug Boluses: Drug Dose /KG Range Administration NotesDocumento5 paginePICU Drug Boluses: Drug Dose /KG Range Administration NotesMaria BudnicNessuna valutazione finora
- Adult electrolyte protocolsDocumento3 pagineAdult electrolyte protocolsRatih Dwi OctariaNessuna valutazione finora
- Intravenous Infusion Orders For Common Medications in The ED and ICU - Bunbury HospitalDocumento39 pagineIntravenous Infusion Orders For Common Medications in The ED and ICU - Bunbury Hospital9wb646hq7mNessuna valutazione finora
- SMILE (Etoposide, Ifosfamide, Methotrexate and Dexamethasone)Documento7 pagineSMILE (Etoposide, Ifosfamide, Methotrexate and Dexamethasone)SolikinNessuna valutazione finora
- Neonatal Intensive Care RecordsDocumento3 pagineNeonatal Intensive Care RecordsClaire LimosNessuna valutazione finora
- Fluids and Drugs in Postpartum Hemorrhage: by DR Izzni Adilah Dzulkifli 30th October 2022Documento35 pagineFluids and Drugs in Postpartum Hemorrhage: by DR Izzni Adilah Dzulkifli 30th October 2022miss_izzniNessuna valutazione finora
- Flip Chart-Converted 2Documento10 pagineFlip Chart-Converted 2anisah mahmudah0% (1)
- Status EpileticusDocumento2 pagineStatus EpileticusJesse M. MassieNessuna valutazione finora
- Medication Administration PolicyDocumento76 pagineMedication Administration PolicyJully GaciasNessuna valutazione finora
- Cisplatin-Pemetrexed (NSCLC)Documento5 pagineCisplatin-Pemetrexed (NSCLC)Sindu SankarNessuna valutazione finora
- Pediatric Drug DosesDocumento7 paginePediatric Drug DosesSadr AkrmNessuna valutazione finora
- Alert Medical Series: Emergency Medicine Alert IIIDa EverandAlert Medical Series: Emergency Medicine Alert IIINessuna valutazione finora
- Dimensional Analysis For Nursing StudentsDa EverandDimensional Analysis For Nursing StudentsNessuna valutazione finora
- Certificate of Completion: Dr. Mark Jacob Mallari Dela RosaDocumento2 pagineCertificate of Completion: Dr. Mark Jacob Mallari Dela RosaHakobito Dela RosaNessuna valutazione finora
- How To Make Dakin's Solution: SuppliesDocumento2 pagineHow To Make Dakin's Solution: Suppliesbradley_brown_1Nessuna valutazione finora
- CBC reference ranges by ageDocumento2 pagineCBC reference ranges by agetommy areanNessuna valutazione finora
- How To Make Dakin's Solution: SuppliesDocumento2 pagineHow To Make Dakin's Solution: Suppliesbradley_brown_1Nessuna valutazione finora
- How To Make Dakin's Solution: SuppliesDocumento2 pagineHow To Make Dakin's Solution: Suppliesbradley_brown_1Nessuna valutazione finora
- August-September 2017 budget scheduleDocumento1 paginaAugust-September 2017 budget scheduleHakobito Dela RosaNessuna valutazione finora
- Antibiotic Sensitivity TestDocumento10 pagineAntibiotic Sensitivity TestJ.A. LauronNessuna valutazione finora
- Indranila 2021Documento22 pagineIndranila 2021reski utamiNessuna valutazione finora
- Anti Thyroid DrugsDocumento22 pagineAnti Thyroid DrugsShahid HameedNessuna valutazione finora
- Surveillance of Healthcare-Associated Infections in Indonesian HospitalsDocumento12 pagineSurveillance of Healthcare-Associated Infections in Indonesian HospitalsRidha MardiyaniNessuna valutazione finora
- 4 - The Circulatory System - PPTDocumento110 pagine4 - The Circulatory System - PPTRinopro 555Nessuna valutazione finora
- Review - Presby Residency ManualDocumento400 pagineReview - Presby Residency ManualSneha SutharNessuna valutazione finora
- Veterinary AnesthesiaDocumento7 pagineVeterinary AnesthesiaMikeunoe100% (1)
- Variability and Accuracy of Sahlis Method InEstimation of Haemoglobin ConcentrationDocumento8 pagineVariability and Accuracy of Sahlis Method InEstimation of Haemoglobin Concentrationastrii 08Nessuna valutazione finora
- DKD and Sglt2iDocumento61 pagineDKD and Sglt2iماكريلا المصريNessuna valutazione finora
- Referral System in IndiaDocumento24 pagineReferral System in IndiaKailash Nagar100% (1)
- Medical Emergency Part 2Documento10 pagineMedical Emergency Part 2navyaNessuna valutazione finora
- Test Bank For Evidence Based Practice in Nursing Healthcare 4th EditionDocumento36 pagineTest Bank For Evidence Based Practice in Nursing Healthcare 4th Editiontyphous.madrierdvfzai100% (47)
- HPNDocumento32 pagineHPNkaren GoNessuna valutazione finora
- Major Clinical Features of Genital Ulcers ChecklistDocumento1 paginaMajor Clinical Features of Genital Ulcers Checklistgdudex118811Nessuna valutazione finora
- Nasogastric & Gavage - NsoDocumento5 pagineNasogastric & Gavage - NsojamesNessuna valutazione finora
- Most of Cardiac Care Unit (C.C.U) DrugsDocumento57 pagineMost of Cardiac Care Unit (C.C.U) DrugsOsama OmarNessuna valutazione finora
- Tugas Baca Jurnal BT ShuntDocumento53 pagineTugas Baca Jurnal BT ShuntVashNessuna valutazione finora
- 525 FullDocumento9 pagine525 FulldianaNessuna valutazione finora
- Immune Disorders..Ppt FairDocumento79 pagineImmune Disorders..Ppt FairSumi SebastianNessuna valutazione finora
- Management of Intravascular Devices To Prevent Infection: LinicalDocumento5 pagineManagement of Intravascular Devices To Prevent Infection: LinicalCristianMedranoVargasNessuna valutazione finora
- Drug Cards CNSDocumento23 pagineDrug Cards CNSChristine Schroeder100% (2)
- Chemotherapy Protocol: RegimenDocumento6 pagineChemotherapy Protocol: RegimenAlexandra AndronescuNessuna valutazione finora
- Swedish Medical Center Patient LetterDocumento2 pagineSwedish Medical Center Patient LetterMichael_Lee_RobertsNessuna valutazione finora
- Hemolytic UremicsyndromeDocumento60 pagineHemolytic UremicsyndromeMuhammad AleemNessuna valutazione finora
- Con TovaDocumento2 pagineCon Tovasheik muhtasimNessuna valutazione finora
- Caries Risk AssessmentDocumento33 pagineCaries Risk AssessmentSomya Jain100% (1)
- Kidney DiseaseDocumento51 pagineKidney DiseaseRoland IntudNessuna valutazione finora
- POZ 2022 HIV Drug Chart HighDocumento5 paginePOZ 2022 HIV Drug Chart HighManuel S PlasenciaNessuna valutazione finora
- University of Delaware College of Health and Nursing Sciences - Hepatitis B Vaccine Declination Form Students)Documento2 pagineUniversity of Delaware College of Health and Nursing Sciences - Hepatitis B Vaccine Declination Form Students)DonnaNessuna valutazione finora
- Krok 1 Anatomy 6Documento1 paginaKrok 1 Anatomy 6Sandeep KumarNessuna valutazione finora