Potrebbero piacerti anche
- CDC IC Assessment Tool LTCFDocumento14 pagineCDC IC Assessment Tool LTCFIsna Kencana ParamoreNessuna valutazione finora
- CDC IC Assessment Tool OutpatientDocumento20 pagineCDC IC Assessment Tool OutpatientIsna Kencana ParamoreNessuna valutazione finora
- Infection Prevention and Control Assessment Tool For Outpatient SettingsDocumento22 pagineInfection Prevention and Control Assessment Tool For Outpatient SettingsVera IndrawatiNessuna valutazione finora
- Hospital Infection Check List PDFDocumento30 pagineHospital Infection Check List PDFRamayuNessuna valutazione finora
- Infection Prevention Checklist For Dental Setting - CDCDocumento20 pagineInfection Prevention Checklist For Dental Setting - CDCDewi Ratna Sari100% (1)
- DialysisDocumento17 pagineDialysisVera IndrawatiNessuna valutazione finora
- Infection Control Assessment ToolDocumento30 pagineInfection Control Assessment ToolPMNessuna valutazione finora
- Materi CSSD - Arlina - Cek List Rawat Jalan PpiDocumento8 pagineMateri CSSD - Arlina - Cek List Rawat Jalan PpiGulam ArsyadNessuna valutazione finora
- Influenza Pandemic Response Plan for Office BuildingsDa EverandInfluenza Pandemic Response Plan for Office BuildingsNessuna valutazione finora
- IMS Functional Requirements April 23Documento7 pagineIMS Functional Requirements April 23Lorenzo Daniel AntonioNessuna valutazione finora
- Special Edition From The Quality Assessment and Safety Committee Reducing Surgical Site Infection - Where Do I Look?Documento3 pagineSpecial Edition From The Quality Assessment and Safety Committee Reducing Surgical Site Infection - Where Do I Look?Qamar Hafeez KianiNessuna valutazione finora
- Ao2022-0035 Hiv GuidelinesDocumento14 pagineAo2022-0035 Hiv GuidelinesHSQMRAD MPINessuna valutazione finora
- Hps Manual Exp Plus Flu PortfolioDocumento72 pagineHps Manual Exp Plus Flu PortfolioManuel Adalid GameroNessuna valutazione finora
- N Ractice: Infection ControlDocumento12 pagineN Ractice: Infection ControlAnil SukumaranNessuna valutazione finora
- ISPC EH Plan For ASC - Sample PolicyDocumento8 pagineISPC EH Plan For ASC - Sample PolicyScottNessuna valutazione finora
- Sample Infection Control Risk AssessmentDocumento2 pagineSample Infection Control Risk AssessmentMj Celuler100% (1)
- Hisi Aug07Documento16 pagineHisi Aug07Nikesh ShahNessuna valutazione finora
- Occupational Health PhysicianDocumento4 pagineOccupational Health PhysicianNidhi Dhawan ChopraNessuna valutazione finora
- MSQH 5th Edition Draft Standard 5 - Prevention and Control of InfectionDocumento22 pagineMSQH 5th Edition Draft Standard 5 - Prevention and Control of InfectionEsmar A. Hamid Kenoh0% (1)
- Rapid Antigen TestingDocumento10 pagineRapid Antigen TestingKimkylkascie Ocampo TamayoNessuna valutazione finora
- 384 Health Risk Assessment PDFDocumento2 pagine384 Health Risk Assessment PDFditox100% (1)
- Functional RequirementsDocumento7 pagineFunctional RequirementsLorenzo Daniel AntonioNessuna valutazione finora
- BES 133 Basic Occupational Safety and HealthyDocumento9 pagineBES 133 Basic Occupational Safety and HealthyJaya Porsche Ignacio AlegarbesNessuna valutazione finora
- Draft Needlestick Injury Report, Version 6: Concept and JustificationDocumento15 pagineDraft Needlestick Injury Report, Version 6: Concept and JustificationSylvia TeresaNessuna valutazione finora
- Yang Dikirim KerryDocumento15 pagineYang Dikirim KerrySylvia TeresaNessuna valutazione finora
- Immunization Safety SurveillanceDocumento14 pagineImmunization Safety SurveillanceHIRA DASNessuna valutazione finora
- Apss VapDocumento14 pagineApss VapRoxanA BocaNessuna valutazione finora
- Basic Hospital Infection Control ProgramDocumento27 pagineBasic Hospital Infection Control ProgramChenii RoyNessuna valutazione finora
- Dr. Lavanya - Infection Control Risk Assessment (ICRA)Documento37 pagineDr. Lavanya - Infection Control Risk Assessment (ICRA)Lucas TobingNessuna valutazione finora
- Categorization Scheme For RecommendationsDocumento4 pagineCategorization Scheme For RecommendationsSisnita Venny OktaviaNessuna valutazione finora
- 08 Occupational HealthDocumento13 pagine08 Occupational Healthzenagit123456Nessuna valutazione finora
- Lectures SurveillanceDocumento36 pagineLectures Surveillancedileepkumar.duhs4817Nessuna valutazione finora
- Impact On Health Care Associated Infection Rates by Continuous Training of Nursing Staff in Our HospitalDocumento4 pagineImpact On Health Care Associated Infection Rates by Continuous Training of Nursing Staff in Our HospitalAnkush JainNessuna valutazione finora
- New Interventions Targeting Healthcare-Associated InfectionsDocumento15 pagineNew Interventions Targeting Healthcare-Associated InfectionsBrian DelgadoNessuna valutazione finora
- New Interventions Targeting Healthcare-Associated InfectionsDocumento15 pagineNew Interventions Targeting Healthcare-Associated InfectionsBrian DelgadoNessuna valutazione finora
- Guidelines On Infection Control Practice in The Clinic Setting Dec 2011Documento52 pagineGuidelines On Infection Control Practice in The Clinic Setting Dec 2011Just MahasiswaNessuna valutazione finora
- Article: PoliciesDocumento18 pagineArticle: PoliciesSA RAINessuna valutazione finora
- Removal of Sharp Object Patient SaftyDocumento6 pagineRemoval of Sharp Object Patient SaftyAlibaba AlihaihaiNessuna valutazione finora
- N Infection Control ManualDocumento49 pagineN Infection Control ManualAnnu RajeshNessuna valutazione finora
- 13 Patient Saefty and Quality ImprovementDocumento36 pagine13 Patient Saefty and Quality ImprovementShafiq Ur RahmanNessuna valutazione finora
- Patient Safety Thesis PDFDocumento6 paginePatient Safety Thesis PDFasiagroverprovo67% (3)
- Rapid Hospital Readiness Checklist For Covid-19Documento17 pagineRapid Hospital Readiness Checklist For Covid-19rommNessuna valutazione finora
- Pest Control ProgramDocumento3 paginePest Control ProgramhadzoibNessuna valutazione finora
- Functioning of Infection Control CommitteeDocumento3 pagineFunctioning of Infection Control Committeetummalapalli venkateswara raoNessuna valutazione finora
- Penerapan Pencegahan Dan Pengendalian Infeksi (PPI)Documento50 paginePenerapan Pencegahan Dan Pengendalian Infeksi (PPI)dyah poernomoNessuna valutazione finora
- Navigating The COVID-19 Pandemic: BackgroundDocumento5 pagineNavigating The COVID-19 Pandemic: BackgroundAries RHNessuna valutazione finora
- TAP Guide For Facility User 508Documento14 pagineTAP Guide For Facility User 508Somaya MostafaNessuna valutazione finora
- Lec - 7 Steps of An OE (1-3)Documento24 pagineLec - 7 Steps of An OE (1-3)Hussein Omar Ali 212-41-1419Nessuna valutazione finora
- Check List of Research Priority Area: National Health Challenge GrantsDocumento9 pagineCheck List of Research Priority Area: National Health Challenge GrantsMarfaa NaseemNessuna valutazione finora
- Needlestick InjuryDocumento24 pagineNeedlestick InjuryAli AlisonNessuna valutazione finora
- Assessing High-Risk Scenarios During An Assessment: Fact Sheet 14Documento2 pagineAssessing High-Risk Scenarios During An Assessment: Fact Sheet 14Ivan PavlovicNessuna valutazione finora
- Objectives of Infection ControlDocumento34 pagineObjectives of Infection ControlMoh Yousif100% (1)
- Root Cause Analysis Investigation Report TemplateDocumento3 pagineRoot Cause Analysis Investigation Report Templatebenaoumeur benounaNessuna valutazione finora
- Infection-Prevention-Control HDFDocumento15 pagineInfection-Prevention-Control HDFArlene AngelesNessuna valutazione finora
- Organization Name Occupational Health Service: OrganizatitionaDocumento16 pagineOrganization Name Occupational Health Service: OrganizatitionaSA RAINessuna valutazione finora
- Ohs and Inc. Acc ReportingDocumento37 pagineOhs and Inc. Acc Reportingkurt94764Nessuna valutazione finora
- WHO 2019 Ncov Hospital - Readiness - Checklist - Tool 2020.1 EngDocumento17 pagineWHO 2019 Ncov Hospital - Readiness - Checklist - Tool 2020.1 EngpertiwiNessuna valutazione finora
- In and OUTPATIENT Full Ward Audit Template May 2015Documento27 pagineIn and OUTPATIENT Full Ward Audit Template May 2015ibrahim helwaNessuna valutazione finora
- ICRADocumento13 pagineICRAevri liaNessuna valutazione finora
- Rekapitulasi Laporan Psikotropika: NO Nama Satuan Stok Awal Pemasukan PBFDocumento8 pagineRekapitulasi Laporan Psikotropika: NO Nama Satuan Stok Awal Pemasukan PBFFajarRachmadiNessuna valutazione finora
- Obat Expired Gudang Farmasi Tahun 2020Documento4 pagineObat Expired Gudang Farmasi Tahun 2020FajarRachmadiNessuna valutazione finora
- Pesanan Benang Rsud Cikalongwetan Ke CBR Benang KodeDocumento1 paginaPesanan Benang Rsud Cikalongwetan Ke CBR Benang KodeFajarRachmadiNessuna valutazione finora
- 05 Rekapitulasi Mei 2016Documento12 pagine05 Rekapitulasi Mei 2016FajarRachmadiNessuna valutazione finora
- Sop Cleaning Rev 06 - 2018 Rev Baru (Repaired)Documento20 pagineSop Cleaning Rev 06 - 2018 Rev Baru (Repaired)FajarRachmadiNessuna valutazione finora
- Change Control Form: Giva Olviana YudhistaDocumento4 pagineChange Control Form: Giva Olviana YudhistaFajarRachmadiNessuna valutazione finora
- Penyampelan Sanvita BDocumento2 paginePenyampelan Sanvita BFajarRachmadiNessuna valutazione finora
- Sodium Selenite - Sciencelab PDFDocumento6 pagineSodium Selenite - Sciencelab PDFFajarRachmadiNessuna valutazione finora
- Sodium Selenite - Sciencelab PDFDocumento6 pagineSodium Selenite - Sciencelab PDFFajarRachmadiNessuna valutazione finora
- PVP Sanmol ForteDocumento17 paginePVP Sanmol ForteFajarRachmadiNessuna valutazione finora
- Monthly Record Process Validation: Note: Red Font Is WPS/ACTUAL Date For Previous MonthDocumento31 pagineMonthly Record Process Validation: Note: Red Font Is WPS/ACTUAL Date For Previous MonthFajarRachmadiNessuna valutazione finora
- Sanfuliq PVP RegistrasiDocumento25 pagineSanfuliq PVP RegistrasiFajarRachmadiNessuna valutazione finora
- Safety Data Sheet: 1. Identification of The Material and Supplier Magnesium OxideDocumento6 pagineSafety Data Sheet: 1. Identification of The Material and Supplier Magnesium OxideFajarRachmadiNessuna valutazione finora
- Hyaluronic Acid - Science LabDocumento5 pagineHyaluronic Acid - Science LabFajarRachmadiNessuna valutazione finora
- Curcuminoid in Curcuma Xanthoriza PDFDocumento5 pagineCurcuminoid in Curcuma Xanthoriza PDFFajarRachmadiNessuna valutazione finora
- Rhetoflam 2.5% Gel SC9486 SC9484: 2016 - 2 Batch 3Documento3 pagineRhetoflam 2.5% Gel SC9486 SC9484: 2016 - 2 Batch 3FajarRachmadiNessuna valutazione finora
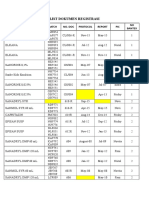
- List Dokumen Registrasi: Product Batch No. Doc Protocol PIC NO BantexDocumento3 pagineList Dokumen Registrasi: Product Batch No. Doc Protocol PIC NO BantexFajarRachmadiNessuna valutazione finora
- Montly RecordDocumento4 pagineMontly RecordFajarRachmadiNessuna valutazione finora
- Assessment Report On Glycyrrhiza Glabra L. And/or Fisch, RadixDocumento37 pagineAssessment Report On Glycyrrhiza Glabra L. And/or Fisch, RadixFajarRachmadiNessuna valutazione finora
- Diabetic Foot Infections - A Comprehensive OverviewDocumento12 pagineDiabetic Foot Infections - A Comprehensive OverviewAleEscobarNessuna valutazione finora
- 4.0 TherapyDocumento19 pagine4.0 TherapyKidu WrietaNessuna valutazione finora
- Medical Microbiology II Lecture 1Documento55 pagineMedical Microbiology II Lecture 1CarinaJongLeeNessuna valutazione finora
- Peter Mccullough Covid Spike Protein Lecture PDFDocumento14 paginePeter Mccullough Covid Spike Protein Lecture PDFKlaudiko Ilgabibich100% (1)
- Peanut PasteDocumento62 paginePeanut PasteOctavia Monica CakrawinataNessuna valutazione finora
- COVID-19 in Mexico From A Holistic Point of View: Analysis, Statistics and Trends (June 2020)Documento5 pagineCOVID-19 in Mexico From A Holistic Point of View: Analysis, Statistics and Trends (June 2020)Edrai ValdiviezoNessuna valutazione finora
- Microbiology & Parasitology Module 2 Part 2Documento15 pagineMicrobiology & Parasitology Module 2 Part 2BARRERAS Aubrey Eden Faye G.Nessuna valutazione finora
- Mushoku Tensei - Arc 19 - Young Man Period - Subordinates ChapterDocumento356 pagineMushoku Tensei - Arc 19 - Young Man Period - Subordinates ChapterMarc PasNessuna valutazione finora
- Istc & DotsDocumento67 pagineIstc & DotsNadilaNessuna valutazione finora
- HCV Persistence: Cure Is Still A Four Letter Word: See Article On Page 106Documento3 pagineHCV Persistence: Cure Is Still A Four Letter Word: See Article On Page 106bmnlthyukNessuna valutazione finora
- Hafnia AlveiDocumento5 pagineHafnia AlveiluisNessuna valutazione finora
- National Core Standards 2011 1Documento52 pagineNational Core Standards 2011 1yos_peace86Nessuna valutazione finora
- Innovation in HealthcareDocumento21 pagineInnovation in HealthcareFatima Khalid100% (1)
- Sop IsolationDocumento10 pagineSop IsolationROHI SINGHNessuna valutazione finora
- THE INDEPENDENT Issue 584Documento56 pagineTHE INDEPENDENT Issue 584The Independent MagazineNessuna valutazione finora
- Environmental Sampling: Microbiological Sampling of AirDocumento19 pagineEnvironmental Sampling: Microbiological Sampling of Airjtello8934Nessuna valutazione finora
- Faith Leader Letter To Governor WolfDocumento4 pagineFaith Leader Letter To Governor WolfSean DamonNessuna valutazione finora
- Nursing Care Plan For Master Shyne With AllDocumento17 pagineNursing Care Plan For Master Shyne With AllsreekalaNessuna valutazione finora
- Cirrhosis of Liver, Liver Cancer, HepatitisDocumento72 pagineCirrhosis of Liver, Liver Cancer, HepatitisBabita DhruwNessuna valutazione finora
- Mexico Covid 19 Case Study EnglishDocumento63 pagineMexico Covid 19 Case Study EnglishutahNessuna valutazione finora
- Virology: Herpesviruses II: Herpes SimplexDocumento4 pagineVirology: Herpesviruses II: Herpes SimplexJaz CNessuna valutazione finora
- HEM SOP Biological Safety v1Documento8 pagineHEM SOP Biological Safety v1Kaoru AmaneNessuna valutazione finora
- Urinary Tract InfectionsDocumento44 pagineUrinary Tract Infectionstummalapalli venkateswara rao100% (2)
- Upaya Pencegahan Terhadap Bahaya Infeksi Silang Saat Melakukan Perawatan Oleh Dokter Gigi Di MakassarDocumento5 pagineUpaya Pencegahan Terhadap Bahaya Infeksi Silang Saat Melakukan Perawatan Oleh Dokter Gigi Di MakassarrosaNessuna valutazione finora
- KPFBA Poultry Proteins+ Nov 2022 - Vol 2 Issue 11Documento12 pagineKPFBA Poultry Proteins+ Nov 2022 - Vol 2 Issue 11Arun DeshwalNessuna valutazione finora
- Anti-Infective Drugs: Jan Bazner-Chandler MSN, CNS, RN, CPNPDocumento85 pagineAnti-Infective Drugs: Jan Bazner-Chandler MSN, CNS, RN, CPNPralucaioana89100% (2)
- NCP FractureDocumento7 pagineNCP FractureMacris BondocNessuna valutazione finora
- DM 2020-0187 - Must Know Covid IssuancesDocumento18 pagineDM 2020-0187 - Must Know Covid IssuancesFranchise AlienNessuna valutazione finora
- Vibriosis in AquacultureDocumento12 pagineVibriosis in AquacultureRomi NovriadiNessuna valutazione finora
- Disaster and Emergency Management in Canada IntroductionDocumento30 pagineDisaster and Emergency Management in Canada Introductionopdebeeck.jaNessuna valutazione finora