Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
448 Full
Caricato da
Sonnymon A. SobrevillaTitolo originale
Copyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
448 Full
Caricato da
Sonnymon A. SobrevillaCopyright:
Formati disponibili
REVIEW ARTICLES
THE PHYSICAL DEVELOPMENT OF CHILDREN
A Guide to Interpretation of Growth-charts and Development
Assessments;and a Commentary on Contemporary
and Future Problems
Frank Falkner, M.R.C.S. (Eng); L.R.C.P. (London)
The Child Development Unit, University of Louisville Medical School
I N THE TITLE Of this essay the traditional quantity of data, charts and grids concern
partner of development—growth-—is ing growth that have appeared in the last
missing. We have been taught that growth 20 years. This is not surprising and not the
refers to tile multiplication of cells and size fault of physicians. It is perhaps an irritat
changes, while development concerns the ing fact that development and its allied
maturation of such structures and their con problems cannot be discussed without a
comitant functions. Today we realize that basic, simple knowledge of biometiy. The
the whole process—call it what you will reader can be assured that the knowledge
is extremely complex and a mass of proc he requires is not complicated and will
esses interacting upon each other. Because, stand him in good stead in many branches
in addition, there is no dividing line be of his scientific art. Because some persons
tween the two terms, it seems desirable to have perfectly adequate knowledge of this
drop an unnecessary and rather false divi subject as applied to medicine, this infor
sion and use but one of the two good words. mation has been placed in the Appendix.
It is vital to ask what extent may we use
PART I. A GUIDE TO THE INTERPRETA norm.s or standards of any measurement?
TION OF GROWTH-CHARTS AND Our whole basis of the concept of normal
DEVELOPMENT ASSESSMENTS ity in child health seems to be tile ever at
The pediatrician is confronted today with tendant norm. And surely there was never a
many aspects of development. Are babies more dangerous companion. Norms de
who are fed two different regimens grow scribe whether a child is big or small;
ing comparably? Is a patient receiving whether he is anemic or polycythemic;
steroids being stunted? Or does an anabolic whether he has many teeth or few teeth
hormone hasten epiphysial closure to the usually all these examples being related to
extent that it causes premature arrest of his age. But the pediatrician wants to ap
growth? Before interest can be taken in praise his individual patient. The norm
such questions, and in the problems of does not say whether these descriptions are
identifying true disturbances in develop desirable or undesirable. If the norms are
mental patterns, the basic principles of coupled to a background involving other
human development, of present methods, areas of study, then and only then can they
and the resources available must be criti evaluate. This kind of information is very
cally reviewed. sparse. How then, can we use the norm to
The pediatrician and his ancillary col better advantage? Normal individual chil
leagues may well be overwhelmed by the dren will deviate either side of the norm
Dr. Falkner is a Markle Scholar in Medical Science.
ADDRESS: 323 East Chestnut Street, Louisville 2, Kentucky.
PEDIATRICS, March 1962
448
Downloaded from www.aappublications.org/news by guest on May 11, 2019
REVIEW ARTICLES 449
(average)with muchfrequency,as any receiving the physician's interest should
doctor, or parent, or indeed child, knows. come from a similar group of children to
How far, though, can they deviate without that which produced the data from which
any of these three important groups of the ranges are derived. In other words, the
people becoming anxious? After learning original sample should be homogenous and
the norm, we must also know the range of the individual child fit into its characteris
average limits. tics. In practice this is rarely achieved to an
Before proceeding to practical considera ideal degree. But it is important to note the
tions, two important points must be made: characteristics of the sample being used
whenever a large sample of children is for comparison. At least the sample itself
studied for, say, height at certain ages, the must be homogenous in age, sex and basic
results can be, and usually are, presented race. If in a sample of English boys aged
as the average height of these children at 10 years, there are some Southern Japanese
each age. This curve will naturally absorb children, the resultant data will not be too
the individual patterns of each child and helpful—nor if the child himself is Japanese
will be a smooth curve with few dramatic and is being fitted into standards of white
peaks or changes. The widely used Iowa Mid-western Americans. It is a well, too,
Growth Charts afford one such good ex to note the date of the investigation. We
ample. Many individual children will show should use with reservation standards
such peaks and changes, and, of course, compiled from data collected some time
will be growing perfectly normally on their ago. Children are maturing earlier and get
own individual curve. A good example of ting bigger for their age each 2
this is given in Figure 7 (Appendix), show modern standards should be used where
ing that when gains in height are plotted possible. This also points to the necessity
this effect can be very noticeable. of constantly renewing and polishing the
The second point is that there is no standards we use in child health.
clear-cut place where abnormality starts Most of the growth standards in use rely
and normality ends. Figure 6 (Appendix) upon height and weight data, and it is these
shows a purposely imaginary and exag two measures that the pediatrician accepts
gerated example. Are the children in the as useful. Weighing must be easily the most
hatched “¿common-ground― area very big common procedure in child health. Yet,
dwarfs or very, very small normal chil while height is more bothersome to meas
dren? ure, it is a highly stable indicator of devel
The range of average limits gives points opment; weight, on the other hand, is in
within which we should expect a healthy fluenced by a great many factors and may
child's measurements to fall. This range is fluctuate greatly—especially in the early
of much more use than the norm by itself. days of life. This is not to say it is an un
Traditionally these limits are the 95th and reliable measurement for use in the assess
5th percentiles; or ±2 standard deviations ment of development, but its interpretation
of the mean (see Appendix for clarification is more difficult. Is it beneficial to reach a
of terms). A child's measurement falling at heavier weight more quickly in the new
either of these outer limits (of a distribution born period? What does the weight repre
curve), or outside, should cause suspicion sent? Is is water, muscle, bone or fat? Or
and careful appraisal. We cannot go further is it a combination of these basic compo
than that. As the child is growing his prog nents? Weight can be lost—an ability not
ress will be watched with advantage, and shared by height—normally and physiologi
it is here where the available data can be cally, in disease, malnutrition or dieting.
most useful. In health the patterns of weight and height
One important point: an individual child development are very similar, and together
Downloaded from www.aappublications.org/news by guest on May 11, 2019
450 PHYSICAL DEVELOPMENT
they give good indications of size. When as YEARS
sessing a weight measurement alone it is 2 4 6 8 0 2 4 6
important to remember its instability—an
instability which after search of cause, and
evaluation, can be useful.
55
The Rate of Growth
50
Cl)
If an individual child is seen more than w
@ 45
once and measured both times, the differ U
HEIGHT FOR AGE
ence between the measurements tells how 40 OF ONE BOY
much he has increased or decreased over 35
a certain time period. This is an increment. 30
It can be a negative increment—in the case,
25
for instance, of weight. If a child were
measured on all his birthdays up to 20
year of age, two valuable curves could be
plotted. Height is here used as an example.
A curve showing the height status at each
age—that is, the distance reached along the
ANNUAL GAINS
path toward final adult height. Hence, this U) OF SAME BOY
w
is a distance curve. The very great majority I
0
of standards and charts in common use in
ternationally today are of this type. They
can describe the size of a patient by mdi
cating his corresponding position on one of
the curves, or in one of the tables, which
have been derived from averages of large
numbers of children measured at various 2 4 6 8 10 I2 14 16 18 20
ages. The children at each age forming these YEARS
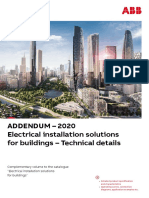
samples are usually different individuals, Fry. 1A. Curves showing (above) height of a boy
since the study is done within a short time. at various ages (distance) and (below) annual gains,
This is a cross-sectional study. plotted from first curve (velocity).
A curve showing, at each age, how much
the child grew, for example, in the preced It is simply analogous to a fast but rapidly
ing year. These will be annual increments. braking motor-car. Then between 3 and 10
This is his growth rate for successive years. years the child grows, comparatively, at a
It is therefore a velocity or rate curve. We steady nate and will often reach the slowest
need both types of curves, for one shows period of all just before the start of puberty.
the size of the child, and the other the rate When this phase is reached a sudden spurt
at which he is growing. Figures 1A and lB (the adolescent growth spurt) occurs, and
show the progress in height of one imagi marked acceleration occurs for the only
nary normal child throughout his growing time in postnatal life. °After a sharp peak,
life. an equally marked deceleration occurs, fin
It is at once obvious how important it is ishing at zero when adult status has been
to realize the quite normal great variation reached.
in rate of growth at the various ages of an Information on rate of growth is scarce.
individual. Although in the first 2 years of
* This statement is made in a broad sense. There
life the baby is growing very rapidly in
is, for example, in some children, a slight “¿mid
deed, the growth is also rapidly decelerat growth spurt―and a growth spurt after a severe
ing. This concept is often difficult to grasp. illness.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
REVIEW ARTICLES 451
age
Birth 1mo 3 no. 6mo. 9mo. lyr. yr.
boys03 years
0
.
-C 40H •¿ —¿â€”
U
C
38,
@ 37
z
:‘:
/f/ 0
-C
U
C
.C
U
C
N.tS—S@@
range s f,.m Itli 0150 psrssst$I..
,,.. as,.,,.
Fic. lB. Height for same boy (Fig. 1A) in first 3 years of life, plotted on a chart for use in this age span.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
452 PHYSICAL DEVELOPMENT
It can be derived only from measuring therefore necessary to adjust increments so
groups of children at various ages and then that they become annual—before compari
measuring the same children again, say, one son with annual rate standards. This is a
year later. This is a longitudinal study. simple procedure wherein an assumption of
Well-known examples@ are the studies regular ( linear) rate of growth is made.
founded at Harvard, Denver and Berkeley. Ranges of average limits are of more use
Though such studies are obviously time than means in using incremental data, just
consuming, expensive and administratively as in distance curves. There are two ob
difficult to run, the needed data can be ob stacles in the way of giving these ranges:
tamed only in this way. Using cross-section First, they have not been published for the
ally obtained data to produce rate curves whole age range in childhood; second, such
(withoutverylargesamplesandcompli limits would be very wide and not have too
cated statistical procedures) is not permis much meaning—especially in adolescence
sible, because the same children are not where there is such a very large spread in
being followed up. In the whole develop average-range. There are, though, other
mental age range of children there are few factors that may be turned to, and a pro pos
published data available on rates of growth. of this a discussion on maturation can now
(It mayalsoberemarked
that,in thepast, follow.
findings from some good longitudinal stud
ies have been reported only cross-section Maturity: General
ally.) Having pointed out the importance At final adult size we reach an inevitable
of this concept of development, it was dis 100% level of morphologic maturation. Sup
appointing to have to tell the physician that pose that one child has been followed for
it was difficult for him to find reliable tables his whole growing life. By referring to his
or curves that he might use for such stand final stature, for instance, we could then see
ards. Now, at least, information is becoming what percentage of his final height he had
more and more available on this facet. In reaciled at each age. Since height is a good
the past the physician has been somewhat stable indicator of maturity, an indication
loath to advance into such areas with his of his maturity status at various ages would
patients, or his research, for he has believed be available. It is precisely this which
longitudinal studies to be difficult and com has been described5 in a sample of children
plex. But each time he measures his patient, who had been so followed in an excellent
after a time interval, he is, of course, doing longitudinal study. At the same time they
a longitudinal study—on one child certainly, presented biometric data for clinical use.
but he has data on rate recorded. He may A very important logical aproach to the
therefore be encouraged to plot his patient's appraisal of children's growth has come
path both in distance and rate and reap a from this work: namely, that a normal child
useful aid in assessing developmental prog may be either an average, late or early ma
ress. turer. In practice, roughly before 7 years
One word of warning: increments are of age, this is of not too great importance;
small measures in amount compared to total but later if he is compared to standards
size measures (e.g., height may be 50.0 in.; wherein all children are lumped together,
the annual increment may be 2.0 in.). then he may appear far “¿behind―
or “¿ahead,―
Therefore the actual measurements must be when in fact he is growing quite properly
done carefully (on two occasions, where on Ins own normal curve.
errors could be compounded) and accu Girls, on an average, reach physical ma
rately lest the error of measurement exceed
* For example, suppose that an adolescent is
the increment.4 Obviously in a busy practice
seen after a 10-month interval and the 10-month
a physician cannot always see his patient increment is 2.0 inches. The annual increment (for
exactly one year from the last visit, should comparison to annual rate standards) = (2.0 x
he wish to find his annual increment. It is 12) ÷ 10= 2.4 inches.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
REVIEW ARTICLES 453
turity about 2% years before boys and are Recently Stuart et al.6 have published
finally some 6 in. shorter. So separate curves some results of their longitudinal study,
or tables are always needed when dealing and this confirms the general principles of
with maturity factors. Average curves have Bayer and Bayley.5
been produced5 that were derived from
grouping the children into different cate Maturity: Skeletal
gonies of maturity status—namely, early, In the concept of maturation of the grow
average and late. This then showed that ing child a most important indicator of this
there are six groups of children commonly status is the maturity of the skeleton. Ana
seen, and an individual child may be placed tomically, in reducing the whole process to
in one group and compared to that group. its simplest level, bone is formed from carti
In problems of growth this concept is most lage. The primary centers of ossification in
important, in everyday practice it is no less this cartilage lead to prenatal bone forma
important, but if standard curves are used tion, while after birth further ossification
along more traditional lines, and being starts from secondary centers of the carti
averages of all groups, then it must be re lage. When we measure a child's height,
membered that an individual starting to ex and his rate of height growth, we are meas
hibit a different pattern than previously uning, basically, his growth in cartilage at
may merely be maturing “¿early― the growing ends of his bones. Ossification
or “¿late.―
Group 1 consists of average-maturing is a sequential event and eventually will
children who will closely approximate the have completely ossffied these ends. Growth
common mean curve for height and weight has then ceased. It is very much a one-way
at stated ages. Group 2 consists of early process. In anatomic terms, when the epi
maturing children who are tall in childhood physes have fused, that bone can grow no
solely due to the fact that they are advanced further. ( This apparently is not strictly true
in time over average children; their data in some bones for some interesting reasons,8
will fall above the average curve, but not but is virtually so.) Skeletal maturation as
exaggeratedly so. Group 3 consists of early sessments aim at estimating the degree to
maturing children who are also “¿geneti which this process ( which has been termed
cally―(mainly) tall from early childhood and osteogenesis as opposed to chondroplasia
who continue to mature rapidly; these chil cartilage growth) has progressed. If one
dren will reach adult status in advance of process is sequential upon the other and
the average and will be tall adults. Their correlated intimately, surely there is little
data will fall well above the mean curve. point in separating them and measuring
Groups 4 and 5 are similar to Groups 2 and both? In health the two processes are
3, but they are late maturers, with or with nearly always linked and run parallel,
out genetic shortness, who will fall below though their rates may differ. But suppos
the mean curve in the same fashion. ing, as an example, the ossification process
Group 6 is indefinite and is met more was under a different endocrine control to
often than was first thought, particularly that of cartilage growth (as it is probably
by physicians approached for a “¿growth in the rat7) and dissociation occurred. Then
problem.― It consists of children in whom were the ossification processes to be stimu
the start of puberty occurs much earlier, lated much more than cartilage growth,
or later, than one would have expected. initially a child could be large for his age.
The spurt may occur suddenly and unex Soon, however, the more rapid ossification
pectedly early, or be a muted gradual proc would overwhelm the cartilage growth and
ess when the child is delayed. Since he has the child would ultimately be stunted.
been growing steadily for a longer or shorter There was not a normal amount of time for
total “¿growthlife― he may well become growth before the epiphyses closed. An ex
much taller or shorter as an adult than ample of this patterning can occur in the
would have been thought. adrenogenital syndrome and also during
Downloaded from www.aappublications.org/news by guest on May 11, 2019
454 PHYSICAL DEVELOPMENT
the use of certain so-called growth stimu poses and do have some disadvantages
lators. Methyltestosterone accelerates both (e.g.,theypresuppose
afixedpatternofde
processes, but ossification relatively more velopment of all bones). A point system15
so; hence it may act finally as a stunting in in which certain clear-cut indicators (using
fluence.° appearances of centers and shape changes)
Since adult height is dependent upon the are awarded points, is probably a method
speed of linear (cartilage) growth and by that will yield the best information. A sys
the duration, and this is a function of skeie tem could be worked out for the whole age
tal maturity, it follows that this subject is range, and then standards would need to
related to the breakdown of children into be made for different populations. Tanner16
different types of maturers. Thus its whole is engaged upon this endeavor at present.
importance, especially in growth problems, Garn and Rohmannl7 have shown that the
must be realized. various centers of ossification followed over
The snag is that skeletal maturity is hard a period of time do not relate too well in
to measure. There are various methods,1° general with maturation of other centers
but so far not a specific technique that and that some are better than others. This
allows of truly objective very accurate meas further complicates and challenges.
urement. In research this is a serious im Whatever system is used, if a reasonable
pedance, but in general and clinical use assessment of skeletal maturity is available,
much help is to be found by using one of the very real possibility of predicting final
several “¿atlases―
available. Here the princi adult height becomes apparent. Other in
ple is to compare the radiograph of a given 819 with a longitudinal sample,
child's joint area ( hand and wrist com have produced tables with use of skeletal
monly) with a standard set of films, which maturity status and height for this predic
each represent an average child of a par tion.
ticular age. There are also descriptions of Skeletal maturation may, then, be use
individual bones (maturity indicators) so fully assessed and used as a maturity mdi
that a given film may be fitted quite ac cator for the purposes of aiding the proper
curately into its proper comparative place. labeling of a child's over-all position regard
When the nearest matching film has been ing maturity, and in growth problems.
found the child may be then designated
having a “¿bone
age―as opposed to his chron Other Maturity Indicators
ologic age. The best and most widely used Maturity indicators range from the state
Atlas is that of Greulich and Pylehl for use of permanent dentition to the excretion
with North American children. The hand of the urinary 17 ketosteroids; but the phy
and wrist is extensively used because it con sician will derive the greatest benefit in
tains so many centers of ossification. But, practice from attention to height pattern,
as an example, because so little is changing skeletal maturity status and the state of
rapidly in the early months of life in this puberty. This implies careful attention to
area, another excellent atlas is that of Pyle the presence (or absence) of the secondary
and Hoerr,12 which uses the knee joint. In sexual characteristics when puberty may be
discussing this subject an excellent example conveniently divided into certain stages.
of how important it is to use standards of Descriptions of these have been pub
growth formed from similar children is lished.1' 4,20
afforded by the fact that African babies on Since the menarche in females is such
average are more mature in this factor (and a clear-cut event, this alone will be singled
others, too13) than European or American out for special mention, as lack of knowl
white infants. Atlases, therefore, would be edge about its usual timing may lead to con
needed for widely differing groups of chil fusion in some growth problems, or the as
dren.14 The Atlas methods may be some sessment of the effect of certain drugs upon
what lacking in precision for research pun growth. The menarche occurs in the very
Downloaded from www.aappublications.org/news by guest on May 11, 2019
REVIEW ARTICLES 455
great majority of female children after the us. We do not know why we grow; nor
maximum point of rate of growth in the what makes us stop growing—and, com
adolescent growth spurt phase. A tall and paratively speaking, very suddenly too;
anxious girl is often presented as having a nor why an individual's complex patterns of
growth problem, with the phrase, “¿she is growth produce a particular form of adult;
so tall now and has not yet started her nor why children are maturing earlier and
puberty.― This has often meant that her earlier each 2 and whether there
menarche has not occurred. Frequently is any end to this trend. These are the
these children are on their final and de closed doors. Since the complexities are ob
celerating descent of puberty growth, and vious to all of us, it seems clear, too, that
an assessment of true puberty status and of solution will come only by a combining of
skeletal maturity will often enable the re widely diverse disciplines and studying of
assurance that, in fact, she will soon finish the many separate factors. Great activity
her growth and not be abnormally tall. exists in the field today, and we may expect
exciting results in the future. What is there
Summary to work with in the meantime? The prob
It is important to be aware of normal lems and place of skeletal maturation have
development patterns before individual de been discussed. Consideration will now be
velopment and pertinent factors can truly given to other areas.
be assessed. Simple basic biometric con
siderations have to be grasped and applied. Development of Tissues
Height-and-weight-for-age standards, in the The physician will be interested particu
form of tables or charts—which may take larly in the growth of the three main body
many forms—are useful for assessments, tissue components—fat, muscle and bone
provided ranges of average limits are used, fat particularly, for obesity and allied dis
rather than averages alone. Standards orders are common. These three tissues
should reasonably match the individual's grow at different rates and at different pen
race, background, geographic location and ods, and therefore a knowledge of this pat
generation. Such standards should be eval terning is useful.
uated critically in the light of this discus Fat development may be measured by
sion. The rate of growth is a useful measure, various methods, but none is entirely satis
and its assessment, practical use and rela factory at present. Because approximately
tionships are discussed. Maturity indicators half the body fat is present in the subcu
are important for the physician and par taneous tissue layers, measurement of this
ticularly when abnormal or unusual devel layer with skin-fold calipers* at various
opment is encountered. Skeletal maturation representative sites reflects to some degree
is a good measure, and its assessment is the “¿fatness―
or “¿leanness―
of an individual.
discussed. Puberty status is an important Data obtained from such methods are in
evaluation particularly in growth problems clined to be controversial because of the
in this area. Assessment of all or some of techniques and the different possible ways
the above measures should lead to clarifica of manipulating the data. Soft-tissue radi
tion of developmental status in individual ography at convenient sites (e.g., upper
children provided the basic patterns are arm and thoracic cage) is a useful research
known and biometric considerations ac method of measuring adipose tissue with
cepted. techniques designed to allow of accurate
measurement of the shadows on the
PART II. A COMMENTARY ON CON
film.1'21'22 Such methods give good relative
TEMPORARY AND FUTURE
indications of the growth patterns of fat.
PROBLEMS
There are the important and deep ques * There are many designs of such calipers, and
tions relating to growth itself which stymie their protagonists are rather individualistic.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
456 PHYSICAL DEVELOPMENT
The skin-fold caliper, which is a practical relative tissue measurements, it is impor
instrument,23 probably indicates total body tant to relate each tissue's measure to the
fat in an individual as well as anything else. others' in successive measurements in order
Standards in this measurement are lacking to determine the true picture of growth of
but are being produced slowly but that tissue. A good example is afforded by
surely.24_26 the sophisticated radiographic method
The general fat growth pattern is one of where, assuming the limb is a cylinder, the
rapid gain up to about 9 months of age, tissue diameters can be converted into
with a peak at 3 months. From 1 year on cross-sectional areas.
ward there is a steady small loss, and stabili
zation occurs at 7 years. In many children Body Composition
there appears to be a pre-puberty fat spurt While the previous discussion showed it
occurring before the true spurt when bone is possible to measure relative amounts of
and muscle growth occurs so rapidly. This some basic tissues reasonably simply, and
“¿puppy-fat―
phase may go onto an actual to determine relative growth patterns from
loss of fat during true adolescence, espe these, do such truly represent the more
cially in boys, leading to a final adult equi important total measures such as “¿total
libnium. Thus the chubby 11-year-old child body fat―? The short answer is : “¿We do
rarely has “¿somethingwrong with his not yet know.―
glands,― and will lose his plumpness natu If we were able to break down the body
rally. In girls the gain is more steady and into, and measure, the basic components
leads to the well-known greater amount of of fat, muscle, bone and water—both extra
fat present in the adult female. cellular and intracellular—protein and bone
Bone growth (not considering skeletal mineral, then a major contribution would
maturation) may be assessed of course by be presented to the many disciplines in
height measurements, by caliper measure volved in the study of growth.
ment of rigid bony diameters easily felt Total body density may be estimated by
(e.g., humeral bicondylar axis), or actual such methods as under-water weighing,29
measurement of the long bones in radio air displacement in a closed container,30
graphs—an accurate method for research helium concentration in a similar appara
purposes.27 Maresh28 showed that individual tus,31'32 water disp1acment,@@ and stereo
bones in a child may grow at widely dif photogrammetry.@@ If such measures are
ferent rates—an important factor in final then related to body weight, the specific
body proportions. The general pattern of gravity of fat and the estimation of total
bone development is naturally that of body water,35 it is possible to break down
stature. body weight into its “¿fat― and “¿lean―
frac
Muscle development is measured anthro tion—a valuable contribution.36 Some ex
pometnically by determining circumferences amples of further detailed work on body
of limbs—usually the upper arm and calf; composition are offered by investigations
or, again, by radiography. Development is on total body fat by whole-body scintilla
closely similar to the over-all pattern of tion content of potassium-40,37 total body
bone growth, but of all the tissues muscle biochemical contents (sodium, potassium,
is the one, especially in the male, which is ch1oride),@8 and bone and bone-mineral.@@
heavily laid down in the puberty phase. The recent work of Fniis-Hansen4° is an
The relationship of exercise to muscle mass example of such basic research contributing
is a controversial subject, and an open sci to knowledge of developmental patterns,
entific mind calls for objective methods of which concern the pediatrician in several
investigation before much can be truly ways. Specifically, in investigating the body
known. water compartments in children, he shows
In an individual, when determining these that characteristic changes occur (during
Downloaded from www.aappublications.org/news by guest on May 11, 2019
REVIEW ARTICLES 457
growth) starting with, for instance, a rapid desirability of determining the type.
decrease in relative total body—and extra In their original stimulating work Shel
cellular water volumes during the first year don@4 and Hooton45 first hypothesized that
of life. the body was made up of three continu
The actual accuracy of some of these ously distributed components; they de
body composition measures and their rela scnibed photogrammetnic or anthroscopic
tionships to each other have caused some to methods for their evaluation. Others, in
pause for thought,41 but active and impor similar studies, have since tried to improve
tant work is progressing. Suffice it to say upon these principles. Tanner43 has sug
that the studies are made harder in child gested a refinement using a combination of
hood because of the constantly changing x-ray and anthropometric measures, with a
and growing total organism, the wide in resultant classification using four orthogonal
dividual variations found, and technical (independent of one another) and physio
difficulties. logically based components. There are, too,
The whole subject could be put together the concepts of Macy and Kelly46 of “¿chemi
by the theoretical possibility of finding cal anthropology― as a new approach in
measures from suitable somatometnic or studying child development; and Williams'@7
radiographic techniques which will give “¿biochemicalindividuality,― postulating that
reliable measures of the important basic individual patterns of biochemical devel
components of the total composition of the opment exist. Much can be learned from
body. studying the farm animals, according to ex
If we move into the question of control of pert research workers@8 who highlight a
these growth patterns by endocrines, en great need in our research into child
zymes and the biochemical considerations growth. This must be investigated in terms
involved we may start to reel from the of body composition by a combination of
potential complexities; but we will also reliable biochemical and physical methods,
emphasize the already stated need for the both longitudinally (when chemical changes
truly multi-disciplinary approach and the must be assessed while they may be causing
possibility of opening many important doors changes in size of tissues and organs—and
leading to vital corridors in our work. Al some problems can be studied only on a
ready, working with human growth hor birth to maturity basis) and cross-section
mone, Shepard et al.42 have affected a linear ally (by giving information on body compo
spurt in growth of a hypo-pituitary dwarf sition at certain ages). This is a mammoth
by administration of human growth hor task, but no great advance will come with
mone. Tanner et al.@3in an important publi out facing it. Correlation between morphol
cation on steroid excretion suggested that ogy, disease, physiology, and normal and
excretion of l7-ketosteroids is related posi abnormal growth patterns with these meas
tively to bone growth, while the 17-keto ures must ultimately be of concern to the
genic steroids are similarly so to muscle physician.
mass. The stimulation provided by these
findings for further work along these chan Heredity and Environment
nels is obvious. Experienced physicians always regard the
A desirable goal is to know the pattern parents of small, large or obese children, for
of growth of all the components and to be they realize that the hereditary background
able to assess composition usefully. There of a child has a great influence on his
are the interesting problems of the relation growth and final size. This influence has
ship of physique to temperament, of mor been estimated to be as much as 80% of all
phology to disease. That certain body types influences. Garn49 has shown thatmeasur
are clearly morphologically, biologically and ing the parents as well as the individual
socially important and different leads to the child adds greatly to the assessment of the
Downloaded from www.aappublications.org/news by guest on May 11, 2019
458 PHYSICAL DEVELOPMENT
child's development status. Indeed he they be modified by the physician? Here,
makes a plea for growth charts incorporat again, there is an added need for their in
ing this factor. It is timely to teach and vestigation.
accept that an influence on development is To study genetic influences it is natural
not either genetic ( hereditary) or environ and useful to study a group of identical
mental—for this implies two neat pigeon (singleovum)andfraternal(doubleovum)
holes, into only one of which must be twins, ideally on a longitudinal basis and
placed a particular influence. The two fac not restrospectively. By assessing differ
tons are cleanly quite inseparable and inter ences between identical twins, relating such
act constantly. The relationship of phenyl changes to environment, and comparing
ketonuna to mental deficiency is a classic these results with fraternal twins, useful
example. The disease is hereditary, but in knowledge should be gained concerning ( so
order for it to develop, the environment of far) vague mainly genetic possible influ
certain foodstuffs in the diet is necessary. ences. If these studies start at birth, it will
We should think and speak, therefore, of be clear that unless information on the pne
the possible weightings of these factors. It natal environment is available, there will
is quite proper, for example, to say that a be a serious gap in the potentialities of such
certain influence is largely one in which a study.
the genetic weighting is heavy. Prenatal environment is of course notoni
Because of the obvious importance of ously difficult to study and assess, but it
genetic influences they must be measured, must be, and is being, objectively attempted
as indeed must the environmental factors. in some studies. Fetal activity, position, and
Two studies are pertinent to this discussion. maternal influences may be investigated,
Tanner et al.'°were able to find and follow and that monument of prenatal environ
up a group of children (now adult) whose ment—the placenta. Benirschke5@ has al
physical growth had been longitudinally ready demonstrated arteniovenous deep
followed for their first 5 years. Their meas shunts in monochonionic twin placentae re
urements as adults showed that while there suiting in one identical twin nearly ex
was virtually no relationship between size sanguinating the other. Clearly there can be
at birth and adulthood, it increased reaching all degrees of such vascular factors. Aside
a significant maximum (in these first 5 years from these, why is one identical twin so
of life) at 3 years. They also showed that commonly much heavier at birth than the
rate of growth and size appeared interest other? Is it important? Dependence on the
ingly independent. Falkner,― in a detailed same plancenta poses the question—are the
study on the first 3 years of life, confirmed available enzymes, iron, oxygen, et cetera
the resulting conclusion that at birth the equally shared? Differing uterine environ
baby's immediate growth is heavily influ ment may have significantly different ef
enced by peninatal and maternal factors. fects upon each twin. An unravelling of
These recede in influence, and by 2 to 3 these factors, and their relative importance,
years the child is on his own largely ge by biologic methods is certainly timely in
netically weighted curve of growth. But the field of development.
sonic of these peninatal factors may influence The study of chromosomes, and their
permanently. Holt5' and Falknen et al.5' place in human development, is only just
showed that high calony feeding in the pre beginning; yet already, from the very great
mature results in a more rapid weight gain activity in the field, comes a great advance
and thus an earlier hospital discharge. But in our knowledge in some problematical
since this “¿weight―
is probably largely fat, areas. It is in the area of developmental
is this to the ultimate advantage of the pre genetics that the second general important
mature infant? What true long-term handi advances are hoped for in the field of hu
caps persist for the premature baby? Can man biology.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
REVIEW ARTICLES 459
APPENDIX series of measures. If five rats' tails measured 3,
5, 7, 9 and 11 centimeters, the middle points is 7
Statisticians are suspected by many physicians cm—i.e., the median (in this case, also the mean).
as being close relatives of a witch doctor. Medical
If six rats' tails measured 1, 3, 5, 7, 9 and 11 cm
men need be neither overwhelmed nor overly fin the median is 6 cm (still also the mean). But if
pressed by their place in biology, for biometry is seven rats' tails measured 1, 3, 5, 7, 9, 11 and 22
of great use in medical science and essential in the
cm, the median is 7 cm (mean, 8.3 cm). Thus the
field of human growth.
median tells more about the central tendency, es
Some of the numerous branches of statistics
pecially when there are some measures in the
can be easily grasped and will be of great help. group far removed from the middle way out at
one end. This leads to a discussion on distribution.
General Statistics
The mean, or average, is the sum of a series of
Frequency Distribution
measurements divided by the number of measure Frequency distribution simply denotes how a
ments concerned. Statistical abbreviations would set of measures are distributed or displaced about
show thisas: the middle or central tendency. A distribution
k (themean) curve will show us (Fig. 2).
The vertical left-hand axis is often scaled as
@ —¿ (the sum of x (individual measures)
“¿percentageof total cases―; the result is, of course,
—¿ N (the number in the sample)
the same. The horizontal axis is a scale of the
If we measured the height, or hemoglobin level, measurement being used. Often class-intervals are
of every 6-year-old boy in Iceland we could find employed; they are simply regular rises in the
the mean for the population of 6-year-old Ice measurement scale, and the individual measure
landic boys. Obviously we rarely can do this, and ment is fitted into the appropriate ‘¿interval―.
(In
a sample of 6-year-old boys is used. If the sample Figure 2 it is 1.0 cm. An actual measurement would
is large enough, and representative enough, for the be placed in the appropriate intervals; e.g., if it
purpose of the study, then conclusions about the were 47.2 cm, the intervals being every 1 .0 cm, it
population may be made. There is no particular would be in the 47.0-to-48.O cm class-interval. One
magic about very large numbers. Representation chooses consistently either the highest or lowest
and homogeneity, for example, are often much value, should the measure be exactly, for instance,
more important. 47.0 cm.)
The sample may be random (choosing individ The curve shown in Figure 2 is roughly sym
uals from a list with shut eyes and a pin) or metrical and is known as a normal distribution (or
strati/led (with representatives from various groups Gaussian) curve. This means that working from
of the population; for example, social groups). the middle point (the central tendency) there are
Thus the obtained mean could be different from as many individuals below in measurement as
the true mean (is usually unknown) and is influ above it. (There are two extremes, one high and
enced clearly by sampling errors. There are sta one low.) The measurements may be said to be
tistical ways of estimating these errors (usually by balanced.
giving their possible limits) but in any case sam
ples must always be described so that their suita Ranges of Measurements
bility for various conclusions to be drawn can be The physician is clearly interested in central
estimated. tendency; but he usually wants to know what is
the range of average measurements he may ex
“¿Average― pect so that he can see whether a particular meas
The quotation marks about the word “¿average― ured patient will fall in it or not. If the patient
indicate that this term can be used loosely, and it falls outside this range, the physician will know to
may not be clear what is truly meant. It is usually look for a cause. These ranges are demonstrated
taken to imply the arithmetic mean. We have dis and obtained from the formation of the distribu
cussed the mean. Any group of measures can pro tion curve, which of course gives these ranges. So
duce it. It is easy to calculate. We all “¿knowwhat we really want to have an idea of how any set of
it represents.― But do we? If the “¿average―
hemo measurements in a sample are dispersed or dis
globin level of two babies is 12.5 gm/100 ml, we tributed around the central point—in a word
might have one baby with 5.0 gm/100 ml and measures of dispersion. We commonly use for this
one with 20.0 gm/100 ml. If there were three purpose percentiles or standard deviations.
babies, one with a very extreme value will influ
Percentiles
ence the mean greatly. Therefore, we must look
to the median as another measure of central tend Clearly the above-mentioned “¿middle
point― will
ency. This simply denotes the middle point in a have 50%of the individuals above it and 50% be
Downloaded from www.aappublications.org/news by guest on May 11, 2019
460 PHYSICAL DEVELOPMENT
No. of
babies
20
18 CLASS __j___
INTERVAL I
(1cm) I
16
14
12
10
6
ARITHMETIC I
MEAN I MEDIAN
4 (50.3 cm) I (50.6 cm)
2
I1@
46 47 48 49 50 51 52 53 54 55
Length in cm
Fic. 2. A distribution curve of birth lengths of 100 male babies (class interval = 1.0 cm.).
low. It is, in fact, the 50th percentile; it is also, as a measure that tells how much a certain measure
we know, the median (and where the distribution ment “¿deviates―
about the mean point. Just like
curve is absolutely Gaussian, also the mean). So the percentile, it can go to either side of the mean,
that if we say the 50th percentile is 50.6 cm (Fig. smaller or larger, and hence it always should have
2), we mean simply that 50% of the babies in this a plus or minus sign in front of it, for it can be
sample will fall above this measurement and 50% either.
below. It is calculated from the basic formula:
This is not a range though. But if we could say, /@X2 @x 2
below a certain measurement (point) only 5% of ±1S.1).= 4/ -.@-—(-@-)
the sample will measure less, and above another
measurement (point) only 5% measure more, these where 2@x'signifies the sum of each individual
end-points would be useful as ranges. When we measurement in the sample squared; (ix)' is the
quote the 5th and 95th percentiles as specific fig square of the sum of all the measurements; N is
ures of measurement we mean exactly that. We the number in the sample.
also mean that 90% of the sample will fall between Clearly, when you calculate the ± 1 S.D. for
these two end-points. Hence the 5th and the 95th your sample, it will be in whatever unit of meas
percentiles are often accepted as being indicative urement you are working (inches, grams, etc.)—an
of a “¿rangeof normality.― In lay language, not obvious point but one not always fully understood.
many individuals will fall outside these points. Traditionally one reads: “¿126
malnourished boys
(Some scientists might use the 10th and 90th per had a mean hemoglobin level of 8.1 gm/100 ml
centiles. Here, just in the same way, 80% of the (S.D. = 1.2)―;it should be written, and really sig
sample will fall between, and 10% outside at either nifies: 1 S.D. = ± 1.2 gm/100 ml. Adding the
end.) Figure 3 shows the curve of Figure 2 with necessary and missing symbols is not being pe
two percentiles added. dantic but helpful.
A method of calculating percentiles is demon If we subtract 1 S.D. from the mean, and add
strated in Table I. 1 S.D. to it, we have a range of measurements
from —¿1
S.D. to +1 S.D. In a normal distribution
Standard Deviations of the Mean
(see later) this will include 67% of cases. If we use
Standard Deviations are often frightening, seem ±2 S.D.s, then this will include a little more than
ing to be magic, complicated symbols. It helps to 90% of the cases. In other words, using the range
remember, if not to use, the correct full term, ±2 S.D. about the mean is almost the same thing
“¿standard
deviation of the mean―(simply, it is the as the 5th to the 95th percentile. And this ±2 S.D.
root mean square deviation from the mean). It is range is generally accepted by scientists to indicate
Downloaded from www.aappublications.org/news by guest on May 11, 2019
REVIEW ARTICLES 461
No. of
babies 50th PERCENTILE
(same as median)
20
5th PERCENTILE (50.6 cm) 95th PERCENTILE
(47.2 cm) (53.8 cm)
18
I I
16 I I
14
12
10
4
MEAN MEDIAN
46 47 48 49 50 51 52 53 54 55
Lengthincm
Fic. 3. The same curve as in Figure 2, with 5th and 95th percentiles added.
TABLE I the limits of expected findings in “¿normality.―
METHOD OF CALCULATING PERCENTILES* Figure 4 shows the distribution curve with
standard deviations in place. Notice how plus and
minus 2 S.D. from the mean gives a similar type
fit Btcumftx —¿-N of range as the 5th and 95th percentiles, but this
10056.010055.09954.09710 range (±2 S.D.) extends a little further away on
each side from the mean, and thus is a wider
range of “¿average.―
But why use standard deviations when they are
calculated by a rather bothersome looking for
mula, and when percentiles tell us just as much,
4—95.053.08714
Px= [{@N_fO} (i)]+b@
5@.07315
where x = percentile required ; N = number of subjects;
51.05818 fo=the sum of the number of subjects below the point
4—50.050.04015 where x/100 N falls; fm= the number of subjects in the
interval of measurement where x/100 N falls; i=the
interval of measurement chosen (class interval) ; b = the
49.0@513 lower boundary of measurement below the point where
x/100 N falls;
48.01@9 Example: for 50th percentile, in the above sample of
5.047.0S2 —¿ babies birth length:
(_@- 100—40
46.0I45.0 100 18 (1) +50.0=50.555 cm.
f fi= number ofsubjects in each classinterval; B = the
scale of measurements in centimeters increasing by
* Formula for calculating percentiles: class intervals of 1.0. cm; cum f= the cumulative fre
(See ad/olningcolumn) quency (of the subjects).
Downloaded from www.aappublications.org/news by guest on May 11, 2019
462 PHYSICAL DEVELOPMENT
No. of
babies
@ 50th
20
2 S.D. 1 S.D. 1 S.D. -@-2S.D.
(46.5 cm 148.4 cm) (52.2 cm) (54.1 cm)
18
16
14
@ 5th t),@(,.)hI@ 95th
12 I I
I I
10
4
I MEAN MEDIAN
2
46 47 48 49 50 51 52 53 54 55
Lengthincm
Fic. 4. The same curve as in Figures 2 and 3, with standard deviations of the mean (± 1 and 2 S.D.)
placed in.
and are more meaningful to the average physician? Luckily, most measures that are likely to be
Before answering this, it is admirable for the physi used by physicians seem to be normally distrib
cian to use percentiles by themselves and leave it uted. Interestingly enough, weight in some sam
at that. However, if he or an investigator wishes ples is quite skewed—there being a tendency for
to work with his data further and employ such there to be more heavy people than light.
useful measures as the standard error, the coefji
cient of correlation, analysis of variance and many Further Points on Ranges
tests of significance, then the standard deviation
Having just suggested that the limits of the 5th
is used in calculating all of them; hence its use
to 95th percentiles and ±2S.D.s will serve as use
fulness and necessity.
ful indicators of “¿usual
range,―what do we do if
There is one disadvantage of standard devia
a child, for instance, has a measurement outside
tions. They are not appropriate where the distni
this range? Clearly we should look for a cause;
bution is very skewed.
and this brings us to an important point about
Already we know that one standard deviation, be
“¿normal―
populations and “¿abnormal―
ones.
it plus or minus, is a rigid numerical sum. Suppose,
Figure 6 shows a purposefully exaggerated and
as in Figure 5, a distribution curve is by no means
imaginary graph of two distribution curves to
Bell-shaped (non-Gaussian). Here there are more gether. One is a large curve of “¿normal
healthy―
students getting low marks than high. Such a curve
children; one is a smaller skewed curve of dwarfs.
is termed skewed. Here there is a long “¿tail―
to
Is the child whose measurements are found to be
the left. If we subtract and add the 2 standard
in the hatched area at the overlap either a very,
deviations from and to the mean—being an un
very small healthy child, or a giant dwarf? It is
alterable sum—as a means of telling us how many
important, then, to keep this factor in mind when
of the class are included in the range (90% approxi
using such statistical aids and to use them as aids
mately, we said earlier), it shows a completely
and nothing more. The inset shows how a bi-mo
different picture, according to which side of the
diii curve can be formed from two such samples.
mean you are. Note that percentiles are not rigid
It is, then, very important to look for such possi
and always tell you what percentage of the sam
ble underlying “¿divisions―
whenever a bi-modal
ple will fall above or below a certain point. Note
curve is encountered.
in Figure 5 that whereas —¿2 S.D. is not too far
from the 5th percentile, +2 S.D. is much further
out; and that no consistent range is given, mean Use of Tables and Curves
ing different things according to which end is ob When comparing measurements of an individ
served. ual child with a curve of growth, or a set of mean
Downloaded from www.aappublications.org/news by guest on May 11, 2019
No. of
Freshmen
30
25
20
15
10
11 13 16 19 22 25 28 31 34 37 40
Number of Correct Answers
Fic. 5. Distribution curve of marks obtained in human growth examination by a Freshman class. Total
possible points = 40; class interval = points; 1 S.D. = ±6.1 points.
Number of
Children
in samples
Units of Height Measurement
Fic. 6. Overlapping distribution curves of height in two samples of children at a certain age. Note that,
as the top right hand inset demonstrates, if all the children in both samples had been grouped together,
a bi-modal curve results. In measuring the human for any measure it is very important to examine any
resulting bi-modal curve and question whether one should be making two separate curves, and whether
there a hidden “¿abnormal―
or very different sample existant.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
464 PHYSICAL DEVELOPMENT
Unitsof
Measurement
Annual
Gainsin
Height
10 11 12 13 14 15 16 17 18
Age in Years
Fic. 7. Curves of gains (annual) in height of three individual boys—A, B and C. The dotted line shows
the mean annual gain of the three boys.
values, a very simple fact is often forgotten : the where x = the individual measurement, x = the
means calculated to plot such curves are usually mean, and S.D. = ±1 standard deviation of the
from large numbers of children—say height at cer mean.
tam ages. Especially when dealing with gains of So having found suitable standards, we may find
height, it will be noticed how smooth and “¿flat―
that an individual, for his age, is +2.0 standard
these curves tend to be. This is because the mean scores (SC) in weight; —¿1.2SCs in height; and
“¿contains―
both children who are growing very —¿2.5 SCs in hemoglobin concentration. He is
fast and very slowly, and hence the resultant curve clearly a very heavy short child who is grossly
“¿neutralizes―
these extremes. An individual child's anemic.
own curve will be, and should be, much “¿wilder.―
Figure 7 shows this. Three individuals growing at Correlation
the normal fast accelerating rate of adolescence
Measures of correlation are for the purpose of
when plotted as a mean curve do not show at all
showing the degree of relationship between two
a likely curve for an individual boy.
factors or variables. We must be very careful not
to relate causation with correlation, for if two
Standard Scores
variables are closely correlated, it does not neces
In the complexities of growth we do often want sarily mean that one causes the other to alter. In
to assess a child's position, as regards “¿averageness― terpretation must be careful and depend on the
in several different factors—weight; height; hemo circumstances. The correlation-coefficient, then, as
globin concentration; intelligence, perhaps. All it is called, is commonly expressed in texts as r
these factors are measured in different units. The (The Pearsonian r); r is simply the mean cross
standard deviation of the mean is useful here, for product of the standard scores of any two varia
we can use it to calculate, very simply, the stand bles. An r of +1 means that when variable A in
ard score. We take the difference between the in creases 1 standard score, so will variable B. If
dividual's measurement and a mean of a sample r = —¿1,
it shows that as variable A increases 1
to which we are comparing this individual as a standard score, variable B will drop exactly 1. So
“¿standard.―
This difference is divided by 1 stand when r = ±1.0 we have a perfect correlation. If
ard deviation for this sample. r = 0, there is no correlation whatever. Tradition
x—@ ally r's of 0.00 to 0.39 are said to be “¿low―;
0.40 to
Or, the standard score = 0.79, “¿moderate―;
and 0.80 to 1.0, “¿high.―
Downloaded from www.aappublications.org/news by guest on May 11, 2019
REVIEW ARTICLES 465
@AB show how biometry will serve physicians in many
@—¿â€”(MA)(MB)
branches of medicine and human biology.
r(SI@)(SI)l@)
where @AB= the sum of the pairs of individual REFERENCES
measures, A and B, multiplied together; MA and 1. Tanner, J. M. : Growth at Adolescence. Black
MB = means of A and B; N = total number of well, Oxford, 1955.
pairs; S.D. = standard deviation. 2. London County Council: Report on the
Heights and Weights of School Pupils in the
Tests of Significance County of London in 1954. London, L.C.C.,
Chance is always present in any experiment. If 1955.
we wish to determine whether a set of measures 3. Tanner, J. M. : Studies of Child Growth in the
in one sample is truly, and in an over-all way, United States. Lancet, 1 :663, 1949.
different from another set, we must assess whether 4. Falkner, F. : The measurement of physical
this could have occurred by chance alone. We can growth in the pediatrician's office. Pediat.
not ever do this, and so we compromise by quot Clin. N. Amer., 8:13, 1961.
ing betting odds that the “¿oddsare so and so that 5. Bayer, L. M., and Bayley, N. : Growth Diag
this difference could have occurred by chance.― nosis. Chicago, Univ. Chicago Press, 1959.
There are many such tests, but the one we most 6. Stuart, H. C. Ct al: Longitudinal Studies of
commonly see used (and strictly it should only be Child Health and Development: Series II.
so when the measures we are comparing are nor Pr@nIAmIcs (Supplement), 24:875, 1959.
mally distributed) is called the “¿Students'
t test.― 7. Evans, H. M., et al.: Growth and differentia
(“Student―was the signature of an anonymous tion of the skeleton in thyroidectomized
mathematician.) Here hypophysectomized rats, treated with thy
—¿ MA—MB roxin, growth hormone and the combination.
J. Bone Joint Surg., 36A:94, 1954.
/r NA S.D@A+NB S.l)2B
-Jr NA+NB 8. Stuart, H. C. : Personal Communication, 1959.
V L NA+NB—2 JL NANB 9. Sobel, E. H. : The use of methyl testosterone
where MA and MB = the means of the two sam to stimulate growth. J. Clin. Endocr., 16:241,
pies to be compared N = the number of subjects 1956.
in the sample; S.D. = standard deviation. 10. Falkner, F. : Skeletal maturation: an appraisal
There is now a confusing part, for the resultant of concept and method. Amer. J. Phys.
“¿t―
figure is rarely quoted in an article; the reason Anthrop., 16:381, 1958.
being that when it has been calculated, a table of 1 1. Greulich, W. W., and Pyle, S. I. : Radiographic
t values is applied in any statistical
textbook,and Atlas of Skeletal Development of the Hand
a p figure read off. and Wrist. Stanford, Calif., Stanford Univ.
This p figure gives the odds and is a confidence Press, 1959.
level. Often given are the figures p = 0.05, or 12. Pyle, S. I., and Hoerr, N. L.: Radiographic
p = 0.01, for instance. These mean, respectively, Atlas of Skeletal Development of the Knee.
that the odds are but 1 in 20 (5% level) or 1 in 100 Springfield, Thomas, 1955.
(1% level), that the difference between two samples 13. Falkner, F., et al.: Some international com
could have occurred by chance. The actual level parisons of physical growth in the first two
chosen to be designated as “¿significant―
depends years of life. Courtier (Paris), 8:1, 1958.
entirely on the particular worker or problem. The 14. Mackay, D. H.: Skeletal maturation in the
symbols > (greater than) and <(smaller than) hand: a study of East African children.
often are used thus; Trans. Roy. Soc. Trop. Med. Hyg., 46:135,
1952.
p= <0.05>0.01,
15. Acheson, R. M.: A method of assessing skeletal
meaning that the odds lay between the 5% and 1% maturity from radiographs. J. Anat., 88:488,
level. This range is quite often traditionally used 1954.
as a suggestive or significant level. We must always 16. Tanner, J. M.: 4th Conference of Centre In
remember, though, that even at levels as low as 1%, ternational de l'Enfance Growth Studies,
chance can still have been a factor in our results. Brussels, C.I.E., Paris, 1958.
17. Cam, S. M., and Rohmann, C. G.: Communali
Note ties of the ossification centers of the hand
This appendix is intended to serve only as a and wrist. Amer. J. Phys. Anthrop., 17:319,
basis for understanding commonly met terms in 1959.
scientific reading; to show how a basic knowledge 18. Bayley, N.: Tables for predicting adult height
of biometry is necessary for a good grasp of the from skeletal age and present height. J.
highly complex problems of human growth; and to Pediat., 28:49, 1946.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
466 PHYSICAL DEVELOPMENT
19. Bayley, N., and Pinneau, S. R. : Tables for pre composition: III. J. Biol. Chem. 158:685,
(lictmg adult height from skeletal age: re 1945.
vised for use with the Greulich-Pyle hand 36. Behnke, A. R., et al.: Lean body mass. Arch.
standards. J. Pediat., 40:423, 1952. Intern. Med., 91 :585, 1953.
20. Falkner, F. : The somatic measurements. Chapt. 37. Forbes, G. B., et a!.: Estimation of total body
VI in Child Development, Vol. V, of Mod fat from potassium-40 content. Science, 133:
em Problems in Pediatrics, Karger, Basel, 101, 1961.
1960. 38. Forbes, G. B., and Lewis, A. : Total sodium,
21. Garn, S. M. : Comparison of pinch-caliper and potassium and chloride in nlafl. j. Clin.
x-ray measurements of skin plus subcutane Invest., 35:596, 1956.
ous fat. Science, 124:178, 1956. 39. Trotter, M.: A preliminary study of estimation
22. Garn, S. M. : Roentgenogrammetnc determi of the weight of the skeleton. Amer. J. Phys.
nations of body composition. Hum. Biol., 29: Anthrop., 12:537, 1954.
3.37,1957. 40. Fniis-Hansen, B. : Body water compartments
23. Edwards, D. A. W., et al: Design and ac in children: changes during growth and re
curacy of skinfold calipers. Brit. J. Nutr., 9: lated changes in body composition. PEDI
133, 1955. ATRICS,28:169, 1961.
24. Pett, L. B., and Ogilvie, G. F. : The Canadian 41. Tanner, J. M. : The measurement of body fat
weight-height survey. Hum. Biol., 28:177, in man. Proc. Nutr. Soc., 18: 148, 1959.
1956. 42. Shepard, T. H., et al.: Human growth hor
25. Fry, E. I. : Subcutaneous tissue in Polynesian mone: II. Further study of its effect on
children from Rarotonga, Cook Islands. growth in dwarfism. J. Pediat. 57:363, 1960.
Hum. Biol., 32:239, 1960. 43. Tanner, J. M., et al: The relation of body
26. Hammond, W. H. : Measurement and interpre build to the excretion of 17-ketosteroids and
tation of subcutaneous fat, with norms for 17-ketogenic steroids. J. Endocr., 19:87,
children and young adult males. Brit. J. Soc. 1959.
Med., 9:201, 1955. 44. Sheldon, W. H. : Varieties of Human Physique.
27. Day, R., and Silverman, W. A.: Growth of the New York, Harper, 1940.
fibula of premature infants as estimated in 45. Hooton, E. A. : Handbook of Body Types in
roentgen films. Neo-natal Studies, 1:114, the U.S. Army. Cambridge, Flarvard Univ.
1953. Press, 1951.
28. Maresh, M. M.: Linear body proportions:a 46. Macy, I. G., and Kelly, H. J. : Chemical An
roentgenographic study. J. Dis. Child., 98: thropology. Chicago, Univ. Chicago Press,
27, 1959. 1957.
29. Behnke, A. R.: Specific gravity of healthy men. 47. Williams, R. J.: Biochemical Individuality.
J. A.M.A., 118:495, 1942. New York, Wiley, 1956.
30. Collins, D. M.: An Evaluation of the Present 48. Barnicoat, C. R., and Shoreland, F. B.: Chemi
Methods for the Determination of Specific cal composition of edible tissues. New Zeal.
Gravity and Total Body Volume of Human J. Sci. Technol., 33:16, 1952.
Subjects; and a Suggested Modffication of 49. Cam, S. M.: Parental Size and Influence on
One of These Methods. National Phi Deita Offspring: Seminar on Growth in the First
Epsilon Medal Essay, 1958-1959, Washing Three Years of Life. C.I.E., Zurich, 1960,
ton, 1958. Karger, Basel, 1961 (in press).
31. Sin, W. E.: Body composition from fluid spaces 50. Tanner, J. M., et al.: The Aberdeen growth
and density: analysis of methods. Donner study: I. Arch. Dis. Child., 31:372, 1956.
Lab. Report. UCAL 3349, Berkeley, 1956. SE. Falkner, F.: Some physical measurements in
32. Fomon, S.: Body volume estimation in infancy. the first three years of life. Arch. Dis. Child.,
Personal communication, 1960. 33:1, 1957.
33. Zook, D. E.: Physical growth of boys: a study 52. Snyderman, S. E., and Holt, E. L.: The effect
by means of water displacement. Amer. J. of high caloric feeding on the growth of
Dis. Child., 43:1347, 1982. premature infants. J. Pediat., 58:237, 1961.
34. Hertzberg, H. T. E., et al.: Stereophotogram 53. Falkner, F., Cruise, M. 0., and Steigman,
metry as an Anthropometric Tool. WADC A. J. S.: Physical growth of the premature.
Techn. Rep. 58-67. ASTIA Doc. No. AD J. Pediat. To be published.
1509964, 1958. 54. Benirschke, K.: IXth International Congress
35. Pace, N., and Rathbun, E. N.: Studies on body of Pediatrics. Montreal, 1959.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
THE PHYSICAL DEVELOPMENT OF CHILDREN: A Guide to Interpretation of
Growth-charts and Development Assessments; and a Commentary on Contemporary
and Future Problems
Frank Falkner
Pediatrics 1962;29;448
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/29/3/448
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or in its
entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on May 11, 2019
THE PHYSICAL DEVELOPMENT OF CHILDREN: A Guide to Interpretation of
Growth-charts and Development Assessments; and a Commentary on Contemporary
and Future Problems
Frank Falkner
Pediatrics 1962;29;448
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://pediatrics.aappublications.org/content/29/3/448
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
been published continuously since 1948. Pediatrics is owned, published, and trademarked by the
American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.
Copyright © 1962 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on May 11, 2019
Potrebbero piacerti anche
- Therapist's Guide to Pediatric Affect and Behavior RegulationDa EverandTherapist's Guide to Pediatric Affect and Behavior RegulationNessuna valutazione finora
- Jurnal AnakDocumento11 pagineJurnal AnakRoery ImoetNessuna valutazione finora
- Being Well-Born An Introduction to EugenicsDa EverandBeing Well-Born An Introduction to EugenicsNessuna valutazione finora
- Failure To ThriveDocumento11 pagineFailure To ThriveFiraFurqaniNessuna valutazione finora
- The Importance of Cognition in LearningDa EverandThe Importance of Cognition in LearningNessuna valutazione finora
- Shortstaturearchdischild 2013 304829.fullDocumento7 pagineShortstaturearchdischild 2013 304829.fullrhhacker57Nessuna valutazione finora
- Parental Monitoring of Adolescents: Current Perspectives for Researchers and PractitionersDa EverandParental Monitoring of Adolescents: Current Perspectives for Researchers and PractitionersNessuna valutazione finora
- FTT Current Clinical Concepts, PedinRev 2011Documento11 pagineFTT Current Clinical Concepts, PedinRev 2011naynaNessuna valutazione finora
- Failure To Thrive:: Current Clinical ConceptsDocumento9 pagineFailure To Thrive:: Current Clinical ConceptsRodolfo Soto VeraNessuna valutazione finora
- Reflection Commentary Final Print VersionDocumento10 pagineReflection Commentary Final Print VersionHailane BragaNessuna valutazione finora
- The GP Curriculum and Cerebral PalsyDocumento9 pagineThe GP Curriculum and Cerebral PalsyFiaNessuna valutazione finora
- Developmental Assessment of ChildrenDocumento10 pagineDevelopmental Assessment of Childrendrpankajyadav05Nessuna valutazione finora
- Challenges of Finding and Filling A Gap in The LiteratureDocumento3 pagineChallenges of Finding and Filling A Gap in The LiteratureAbdul Maroof KochiNessuna valutazione finora
- Challenges of Finding and Filling A Gap in The Literature: EditorialDocumento3 pagineChallenges of Finding and Filling A Gap in The Literature: EditorialAbdul Maroof KochaiNessuna valutazione finora
- 2010 31 364-367 Timothy Wilks, R. Jason Gerber and Christine Erdie-LalenaDocumento6 pagine2010 31 364-367 Timothy Wilks, R. Jason Gerber and Christine Erdie-LalenaLuisa Maria LagosNessuna valutazione finora
- Clinical Review: Developmental Assessment of ChildrenDocumento9 pagineClinical Review: Developmental Assessment of ChildrenThuzar HlaingNessuna valutazione finora
- Early Detection of Developmental and Behavioral Problems: Pediatrics in Review September 2000Documento10 pagineEarly Detection of Developmental and Behavioral Problems: Pediatrics in Review September 2000annaNessuna valutazione finora
- CPG For Assessment of Children and AdolescentsDocumento18 pagineCPG For Assessment of Children and AdolescentsSarwar BaigNessuna valutazione finora
- Thesis Statement Against Designer BabiesDocumento9 pagineThesis Statement Against Designer Babiesowynqovcf100% (1)
- Odi Irawan JurnalDocumento7 pagineOdi Irawan JurnalOdi IrawanNessuna valutazione finora
- Assessment of Behavioral Adjustment and Behavioral StyleDocumento14 pagineAssessment of Behavioral Adjustment and Behavioral StyleFanni ForgácsNessuna valutazione finora
- Questions:: Exercise 4. Bioethical Dilemma of Gene TherapyDocumento2 pagineQuestions:: Exercise 4. Bioethical Dilemma of Gene Therapyrjay manaloNessuna valutazione finora
- DSM Pediatrics in Review-2010-Gerber-267-77Documento13 pagineDSM Pediatrics in Review-2010-Gerber-267-77BrunoNessuna valutazione finora
- Parenting of Children With Autism Spectrum DisordeDocumento15 pagineParenting of Children With Autism Spectrum DisordePollyanne AlcantaraNessuna valutazione finora
- Developmental Milestones:: Motor DevelopmentDocumento13 pagineDevelopmental Milestones:: Motor Developmenthazell_aseronNessuna valutazione finora
- Si Codaste PR1 Week3Documento8 pagineSi Codaste PR1 Week3Maris CodasteNessuna valutazione finora
- Effective Discipline To Raise Healthy Children: Policy StatementDocumento12 pagineEffective Discipline To Raise Healthy Children: Policy StatementJesse M. MassieNessuna valutazione finora
- Research in Nursing Health - 2017 - Kearney - Challenges of Finding and Filling A Gap in The LiteratureDocumento3 pagineResearch in Nursing Health - 2017 - Kearney - Challenges of Finding and Filling A Gap in The LiteratureIhab Al-AnabousiNessuna valutazione finora
- Developmental MilestoneDocumento17 pagineDevelopmental MilestoneRafael MarvinNessuna valutazione finora
- Functional Constipation in Children: Challenges and SolutionsDocumento9 pagineFunctional Constipation in Children: Challenges and SolutionsJihan FaadhilahNessuna valutazione finora
- Developmental Issues For Young Children in Foster CareDocumento8 pagineDevelopmental Issues For Young Children in Foster CarePedroPocasNessuna valutazione finora
- 01 Careers in Human DevelopmentDocumento26 pagine01 Careers in Human Developmentfrankie cemaniaNessuna valutazione finora
- Developmental MilestonesDocumento17 pagineDevelopmental MilestonesSardono WidinugrohoNessuna valutazione finora
- An Approach To Failure To Thrive': GrowthDocumento5 pagineAn Approach To Failure To Thrive': GrowthJayantiNessuna valutazione finora
- Sternberg 2000Documento18 pagineSternberg 2000sariatul jannahNessuna valutazione finora
- Problem Identification and ClarificationDocumento19 pagineProblem Identification and ClarificationchristinemfranciaNessuna valutazione finora
- Responding and Identifying To Developmental Delay in ChildrenDocumento13 pagineResponding and Identifying To Developmental Delay in ChildrenInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Cognitive and Social DevelopmentDocumento5 pagineCognitive and Social DevelopmentPANI78Nessuna valutazione finora
- Important Considerations in The Initial Clinical Evaluation of The Dysmorphic NeonateDocumento5 pagineImportant Considerations in The Initial Clinical Evaluation of The Dysmorphic NeonateKaroo_123Nessuna valutazione finora
- Greenspan 2008Documento5 pagineGreenspan 2008Jose Alonso Aguilar ValeraNessuna valutazione finora
- Adolescence FinalDocumento110 pagineAdolescence FinalAlexa Nicole GayosoNessuna valutazione finora
- Understanding Technology Use Throughout Development What Erik Erikson Would Say About Toddler Tweets and Facebook FriendsDocumento11 pagineUnderstanding Technology Use Throughout Development What Erik Erikson Would Say About Toddler Tweets and Facebook FriendselaineNessuna valutazione finora
- Study Guide For Pathophysiology The Biological Basis Disease in Adults and Ebook PDF VersionDocumento58 pagineStudy Guide For Pathophysiology The Biological Basis Disease in Adults and Ebook PDF Versionalfred.jessie484100% (38)
- Ordinary Magic:: Lessons From Research On Resilience in Human DevelopmentDocumento5 pagineOrdinary Magic:: Lessons From Research On Resilience in Human Developmentdaniela .lomnicziNessuna valutazione finora
- Developmental Milestones Motor Development - Peds Rev 2010Documento13 pagineDevelopmental Milestones Motor Development - Peds Rev 2010Carolina SanchezNessuna valutazione finora
- The Impact of Racism On Child and Adolescent Health: Policy StatementDocumento16 pagineThe Impact of Racism On Child and Adolescent Health: Policy StatementGloria StahlNessuna valutazione finora
- Failure To Thrive - AAPDocumento11 pagineFailure To Thrive - AAPAlexNessuna valutazione finora
- Milestone and RedflagDocumento5 pagineMilestone and RedflagPutri Zatalini SabilaNessuna valutazione finora
- Cognitive Development PDFDocumento6 pagineCognitive Development PDFsri noviyanty yusufNessuna valutazione finora
- NIH Public Access: Author ManuscriptDocumento11 pagineNIH Public Access: Author ManuscriptRicardo Vio LeonardiNessuna valutazione finora
- 10th Life Science Carol Lilliam Muñoz Avila 2: Identify Desired Results (Stage 1)Documento8 pagine10th Life Science Carol Lilliam Muñoz Avila 2: Identify Desired Results (Stage 1)Carol LilliamNessuna valutazione finora
- AAP Obesity Policy StatementDocumento13 pagineAAP Obesity Policy StatementSonia HaNessuna valutazione finora
- Meta AnalysisDocumento16 pagineMeta AnalysisSabu Joseph100% (1)
- Chapter 1 3 ThesisDocumento21 pagineChapter 1 3 ThesisJohn Patriarca0% (1)
- Peds 2022057010Documento23 paginePeds 2022057010hb75289kyvNessuna valutazione finora
- Coming To Understand The Child Has Autism: A Process Illustrating Parents' Evolving Readiness For Engaging in CareDocumento14 pagineComing To Understand The Child Has Autism: A Process Illustrating Parents' Evolving Readiness For Engaging in CareRojaNessuna valutazione finora
- File JURNAL-5 3d26b5a6Documento4 pagineFile JURNAL-5 3d26b5a6Surya DimastiarNessuna valutazione finora
- Educ10 Module3Documento3 pagineEduc10 Module3carceroleunamNessuna valutazione finora
- Parenting Care Model Is A Rehabilition For Learning Disabled ChildDocumento5 pagineParenting Care Model Is A Rehabilition For Learning Disabled Childaloysia_007Nessuna valutazione finora
- Matrix TFN BascoDocumento7 pagineMatrix TFN BascoChristine Jane BascoNessuna valutazione finora
- THE FIELD SURVEY PARTY ReportDocumento3 pagineTHE FIELD SURVEY PARTY ReportMacario estarjerasNessuna valutazione finora
- IELTS Materials ReadingDocumento9 pagineIELTS Materials ReadingßläcklìsètèdTȜè0% (1)
- Lesson Plan - Organization and ManagementDocumento5 pagineLesson Plan - Organization and ManagementBilly Joe80% (15)
- Guidance UDI Compliance DatesDocumento13 pagineGuidance UDI Compliance DatesGigi EssegiNessuna valutazione finora
- Xiaopan OS: DescriptionDocumento1 paginaXiaopan OS: DescriptionMan SavliNessuna valutazione finora
- Text Ranslation and TradicitonDocumento283 pagineText Ranslation and TradicitonSCAF55100% (4)
- Recovering The Snorra Edda On Playing Gods, Loki, and The Importance of HistoryDocumento17 pagineRecovering The Snorra Edda On Playing Gods, Loki, and The Importance of HistoryM SNessuna valutazione finora
- Heating Curve Lab Report - Ava MonizDocumento7 pagineHeating Curve Lab Report - Ava Monizapi-533828039Nessuna valutazione finora
- Irjet V3i7146 PDFDocumento6 pagineIrjet V3i7146 PDFatulnarkhede2002Nessuna valutazione finora
- Russian Sec 2023-24Documento2 pagineRussian Sec 2023-24Shivank PandeyNessuna valutazione finora
- ESUR Guidelines 10.0 Final VersionDocumento46 pagineESUR Guidelines 10.0 Final Versionkon shireNessuna valutazione finora
- 7th Nani Palkhiwala Research Paper CompetitionDocumento31 pagine7th Nani Palkhiwala Research Paper CompetitionhridhaykhuranaNessuna valutazione finora
- Sullair VARIABLE SPEED - 1800-2200-1800V-1809V-2200V-25-30HPDocumento70 pagineSullair VARIABLE SPEED - 1800-2200-1800V-1809V-2200V-25-30HPJose MontielNessuna valutazione finora
- Sagittarius ProfileDocumento3 pagineSagittarius ProfileWAQAS SHARIFNessuna valutazione finora
- Net June 2013Documento22 pagineNet June 2013Sunil PandeyNessuna valutazione finora
- Pengaruh Promosi Dan Brand Image (Citra Produk) Terhadap Loyalitas Pembelian Produk Pepsodent Di Ramayana Plaza, Jalan Aksara, Medan Dita AmanahDocumento13 paginePengaruh Promosi Dan Brand Image (Citra Produk) Terhadap Loyalitas Pembelian Produk Pepsodent Di Ramayana Plaza, Jalan Aksara, Medan Dita AmanahAhmad HerdandiNessuna valutazione finora
- 1422-Article Text-3684-1-10-20211104Documento57 pagine1422-Article Text-3684-1-10-20211104f.kpobi1473Nessuna valutazione finora
- D904 - D906 - D914 - D916 - D924 - D926 - 8718458 - 04092008 - v02 - enDocumento218 pagineD904 - D906 - D914 - D916 - D924 - D926 - 8718458 - 04092008 - v02 - enАлексей89% (18)
- Competency #14 Ay 2022-2023 Social StudiesDocumento22 pagineCompetency #14 Ay 2022-2023 Social StudiesCharis RebanalNessuna valutazione finora
- Combustion FundamentalsDocumento30 pagineCombustion FundamentalsPrem SagarNessuna valutazione finora
- FPI - Study Permit Application GuideDocumento9 pagineFPI - Study Permit Application GuideKian Mark DarioNessuna valutazione finora
- Unit 2: TransducerDocumento24 pagineUnit 2: TransducerROYAL GAMER YTNessuna valutazione finora
- 3.6 A 40Nm Cmos Highly Linear 0.4-To-6Ghz Receiver Resilient To 0Dbm Out-Of-Band BlockersDocumento3 pagine3.6 A 40Nm Cmos Highly Linear 0.4-To-6Ghz Receiver Resilient To 0Dbm Out-Of-Band Blockershaoyue huangNessuna valutazione finora
- The "Kind Martin" Strategy - Official Olymp Trade BlogDocumento7 pagineThe "Kind Martin" Strategy - Official Olymp Trade BlogGopal NapoleonNessuna valutazione finora
- Budgetary Quote HPE AMD 128cores For DNDSSGDocumento7 pagineBudgetary Quote HPE AMD 128cores For DNDSSGglalit kumarNessuna valutazione finora
- Low Voltage Alternator - 4 Pole: 25 To 60 kVA - 50 HZ / 31.5 To 75 kVA - 60 HZ Electrical and Mechanical DataDocumento12 pagineLow Voltage Alternator - 4 Pole: 25 To 60 kVA - 50 HZ / 31.5 To 75 kVA - 60 HZ Electrical and Mechanical DataDjamel BeddarNessuna valutazione finora
- B - ELSB - Cat - 2020 PDFDocumento850 pagineB - ELSB - Cat - 2020 PDFanupamNessuna valutazione finora
- My TestDocumento18 pagineMy TestBlessmore Chitanha100% (1)
- Glorious Mysteries 1Documento5 pagineGlorious Mysteries 1Vincent safariNessuna valutazione finora
- Markov Decision Processes For Path Planning in Unpredictable EnvironmentDocumento8 pagineMarkov Decision Processes For Path Planning in Unpredictable EnvironmentVartolomeiDumitruNessuna valutazione finora