Potrebbero piacerti anche
- Dr. H. Soekimin, Sppa: Bagian Patologi Anatomi Fakultas KedokteranDocumento45 pagineDr. H. Soekimin, Sppa: Bagian Patologi Anatomi Fakultas KedokteranRommy Kurniawan DeskyNessuna valutazione finora
- Pathology ReviewDocumento26 paginePathology ReviewSafiya James100% (1)
- Inflammation: Deske MuhadiDocumento36 pagineInflammation: Deske MuhadiYUSMAWATI YUSRANNessuna valutazione finora
- Patologi AnatomiDocumento26 paginePatologi AnatomiNia AnestyaNessuna valutazione finora
- Inflammation PPT - OdpDocumento82 pagineInflammation PPT - OdpBhanu PraseedhaNessuna valutazione finora
- WaaazzzzzzDocumento21 pagineWaaazzzzzzSydjad Karl Ursal MiraflorNessuna valutazione finora
- Chronic Inflammation and RepairDocumento44 pagineChronic Inflammation and RepairFu Xiao Shan100% (1)
- InflammationDocumento2 pagineInflammationAndrew BonusNessuna valutazione finora
- Handouts - 6BIOM002W.2 - Inflammation 2018-9 PDFDocumento66 pagineHandouts - 6BIOM002W.2 - Inflammation 2018-9 PDFFatima HusseinNessuna valutazione finora
- Inflammation and RepairDocumento5 pagineInflammation and RepairDENILLE AIRA NOGOYNessuna valutazione finora
- Patho A 1. 3 Inflammation and Repair (Dy-Quiangco, 2015)Documento13 paginePatho A 1. 3 Inflammation and Repair (Dy-Quiangco, 2015)kristineNessuna valutazione finora
- Inflammation Inflammatory Response and FeverDocumento5 pagineInflammation Inflammatory Response and FeverPrincess Denice OrtalezaNessuna valutazione finora
- Muhammad Usman: Associate Professor of Pathology Consultant PathologistDocumento89 pagineMuhammad Usman: Associate Professor of Pathology Consultant PathologistSmithNessuna valutazione finora
- Chapter 2 - Acute and Chronic InflammationDocumento12 pagineChapter 2 - Acute and Chronic InflammationAgnieszka WisniewskaNessuna valutazione finora
- Physiology: Anatomy LectureDocumento4 paginePhysiology: Anatomy Lecturewesrdftyghuijkol wasedrftgyhuijkolNessuna valutazione finora
- Acute InflmmationDocumento39 pagineAcute InflmmationBean GemboelzNessuna valutazione finora
- Pathology 2 PDFDocumento18 paginePathology 2 PDFfadoNessuna valutazione finora
- InflammationDocumento8 pagineInflammationGhazi Uddin AhmedNessuna valutazione finora
- Patho Unit 4.1Documento20 paginePatho Unit 4.1Lily ChouNessuna valutazione finora
- 01.inflammation 1Documento30 pagine01.inflammation 1Shameena KnNessuna valutazione finora
- Inflammation & Wound Healing Part 1Documento2 pagineInflammation & Wound Healing Part 1Julia Rae Delos SantosNessuna valutazione finora
- 03 InflammationDocumento10 pagine03 InflammationAlexa UyNessuna valutazione finora
- Acute InflammationDocumento25 pagineAcute Inflammationa194801Nessuna valutazione finora
- Acute InflammationDocumento76 pagineAcute InflammationOmor faruk HridoyNessuna valutazione finora
- Inflammation & Repair: Tim Dosen PatologiDocumento32 pagineInflammation & Repair: Tim Dosen PatologiNdaru SetyaningrumNessuna valutazione finora
- Histopathology - c3 - Acute and Chronic Inflammation - MasterDocumento28 pagineHistopathology - c3 - Acute and Chronic Inflammation - MasterGhinescu AdrianNessuna valutazione finora
- Inflammation 2Documento21 pagineInflammation 2Umar'Farouq OniNessuna valutazione finora
- Sirs 2013Documento96 pagineSirs 2013wildan acalipha wilkensiaNessuna valutazione finora
- Acute InflammationDocumento55 pagineAcute InflammationMohammad_Islam8790% (10)
- In Ammation, Immunity and Allergy: Learning ObjectivesDocumento6 pagineIn Ammation, Immunity and Allergy: Learning ObjectivesJavier VeraNessuna valutazione finora
- Concept of Inflammatory and Immune SystemDocumento15 pagineConcept of Inflammatory and Immune SystemUchiha Dominic100% (1)
- Acute InflammationDocumento51 pagineAcute InflammationNayela AkramNessuna valutazione finora
- 2.INFLAMMATION AND ITS IMPLICATIONS ..... FinalDocumento81 pagine2.INFLAMMATION AND ITS IMPLICATIONS ..... Finalsaloni singhNessuna valutazione finora
- Inflammation, Wound Healing and Foreign Body ResponseDocumento22 pagineInflammation, Wound Healing and Foreign Body Responseharry potterNessuna valutazione finora
- Acute InflammationDocumento71 pagineAcute Inflammationsi_miaomiao100% (1)
- His To PathologyDocumento7 pagineHis To PathologyDessa MartinezNessuna valutazione finora
- Harsh Mohan Quick Review InflammationDocumento23 pagineHarsh Mohan Quick Review InflammationTanaya PujareNessuna valutazione finora
- II Inflam-PatoDocumento27 pagineII Inflam-Patozenitha firdausNessuna valutazione finora
- Inflammation. Etiology. Vascular Changes. Cellular Events in Inflammation. Acute Inflammation. Morphologic PatternsDocumento57 pagineInflammation. Etiology. Vascular Changes. Cellular Events in Inflammation. Acute Inflammation. Morphologic PatternsZauzaNessuna valutazione finora
- Histopathology - c4 - Adaptations of Cellular Growth and Differentiation - MasterDocumento25 pagineHistopathology - c4 - Adaptations of Cellular Growth and Differentiation - MasterGhinescu AdrianNessuna valutazione finora
- Appendicitis Meningitis: Vascular Cellular Response The Inflammatory Process RepairDocumento10 pagineAppendicitis Meningitis: Vascular Cellular Response The Inflammatory Process RepairYaff DthNessuna valutazione finora
- Pathophysiology Notes - Inflammation and HealingDocumento6 paginePathophysiology Notes - Inflammation and HealingKateNessuna valutazione finora
- Inflammation and RepairDocumento34 pagineInflammation and RepairJoshua HonoridezNessuna valutazione finora
- Anti-Inflammatory Properties of Local Anesthetics and Their Present and Potential Clinical ImplicationsDocumento18 pagineAnti-Inflammatory Properties of Local Anesthetics and Their Present and Potential Clinical ImplicationsXavierLuqueNessuna valutazione finora
- 07 InflammationDocumento69 pagine07 InflammationSangameswaran B.BNessuna valutazione finora
- PathoLec InflammationDocumento10 paginePathoLec InflammationMiguel Cuevas DolotNessuna valutazione finora
- 1 PATHO 2a - Inflammation - Dr. BailonDocumento12 pagine1 PATHO 2a - Inflammation - Dr. BailontonNessuna valutazione finora
- Lecture 3Documento56 pagineLecture 3w2tz2qrqxdNessuna valutazione finora
- 7.2 Muscular System: Human Anatomy and Physiology With Pathophysiology LectureDocumento3 pagine7.2 Muscular System: Human Anatomy and Physiology With Pathophysiology LectureRamea LamanoNessuna valutazione finora
- Pathology Week 5 - 6 FKHDocumento15 paginePathology Week 5 - 6 FKHAnna TohNessuna valutazione finora
- Unit 4.1Documento8 pagineUnit 4.1Bloody MarieNessuna valutazione finora
- INFLAMAATIONDocumento6 pagineINFLAMAATIONSabbir AhmedNessuna valutazione finora
- Care of Preschoolers With Health ProblemsDocumento5 pagineCare of Preschoolers With Health ProblemsmajoodhNessuna valutazione finora
- Robbins Pathology - Chapter 3 TransDocumento18 pagineRobbins Pathology - Chapter 3 Transnath nath100% (7)
- 10 - Body Defense MechanismDocumento6 pagine10 - Body Defense MechanismPrince Mark BadilloNessuna valutazione finora
- Week 1 Study GuideDocumento16 pagineWeek 1 Study GuideKateNessuna valutazione finora
- UntitledDocumento4 pagineUntitledSushmitha GandhiNessuna valutazione finora
- GenpathDocumento10 pagineGenpathNatural Science BiologyNessuna valutazione finora
- #27 - Aisha A. Macapundag 4Cmt TMC ACTIVITY: Other Major Blood Group SystemsDocumento5 pagine#27 - Aisha A. Macapundag 4Cmt TMC ACTIVITY: Other Major Blood Group SystemsRachel ManaloNessuna valutazione finora
- 4C-Mt TMC Rapid Plasma Reagin (RPR) TestDocumento3 pagine4C-Mt TMC Rapid Plasma Reagin (RPR) TestRachel ManaloNessuna valutazione finora
- QUALITY CONTROL (Last Day)Documento5 pagineQUALITY CONTROL (Last Day)Rachel ManaloNessuna valutazione finora
- Activity:: Summative Assessment (By Pair)Documento7 pagineActivity:: Summative Assessment (By Pair)Rachel ManaloNessuna valutazione finora
- Blood ComponentsDocumento5 pagineBlood ComponentsRachel ManaloNessuna valutazione finora
- Abo PanelDocumento2 pagineAbo PanelRachel ManaloNessuna valutazione finora
- CASE 1: A Patient Was Seen in The Emergency Room and A Crossmatch Was Ordered. The ABO Forward and Reverse Grouping Results Are As FollowsDocumento3 pagineCASE 1: A Patient Was Seen in The Emergency Room and A Crossmatch Was Ordered. The ABO Forward and Reverse Grouping Results Are As FollowsRachel ManaloNessuna valutazione finora
- Other Blood Group SystemsDocumento2 pagineOther Blood Group SystemsRachel ManaloNessuna valutazione finora
- 04 - (Second Half) Nitric Oxide in Cellular Adaptation and Disease PDFDocumento11 pagine04 - (Second Half) Nitric Oxide in Cellular Adaptation and Disease PDFRachel ManaloNessuna valutazione finora
- 05 - Cellular Adaptations - SimpleMed - Learning Medicine, SimplifiedDocumento7 pagine05 - Cellular Adaptations - SimpleMed - Learning Medicine, SimplifiedRachel ManaloNessuna valutazione finora
- 04 - (Second Half) Nitric Oxide in Cellular Adaptation and Disease PDFDocumento11 pagine04 - (Second Half) Nitric Oxide in Cellular Adaptation and Disease PDFRachel ManaloNessuna valutazione finora
- 05 - Cellular Adaptations - SimpleMed - Learning Medicine, SimplifiedDocumento7 pagine05 - Cellular Adaptations - SimpleMed - Learning Medicine, SimplifiedRachel ManaloNessuna valutazione finora
- CELLSDocumento8 pagineCELLSRachel ManaloNessuna valutazione finora
- A Review On Plant-Based Rutin Extraction Methods and Its Pharmacological ActivitiesDocumento13 pagineA Review On Plant-Based Rutin Extraction Methods and Its Pharmacological ActivitieswahyuniNessuna valutazione finora
- Manual of Definitive Surgical Trauma CareDocumento256 pagineManual of Definitive Surgical Trauma Carebovine splendor100% (3)
- Indomethacin 392Documento17 pagineIndomethacin 392Mahadie Hasan JahadNessuna valutazione finora
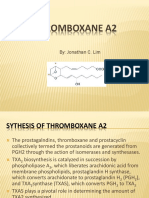
- Thromboxane A2Documento16 pagineThromboxane A2Concepcion R. Aquino0% (1)
- Induction of C-Fos by Prostaglandin F in Human Ciliary Smooth Muscle CellsDocumento9 pagineInduction of C-Fos by Prostaglandin F in Human Ciliary Smooth Muscle Cellsanandhamide81Nessuna valutazione finora
- Pathology Week 2 p1-18Documento18 paginePathology Week 2 p1-18zeroun24100% (1)
- Lotus Notes Bleeding Letting For ClinicalDocumento26 pagineLotus Notes Bleeding Letting For ClinicalMatthieu Decalf100% (2)
- PainoxiaDocumento66 paginePainoxiaOmar WahbiNessuna valutazione finora
- Prostaglandins and LeukotrienesDocumento40 pagineProstaglandins and LeukotrienesParul SinghNessuna valutazione finora
- Understanding Turmeric Anti-In Ammatory Effects and Its Clinical UseDocumento19 pagineUnderstanding Turmeric Anti-In Ammatory Effects and Its Clinical UseBilly JamesNessuna valutazione finora
- Lipids 31 2012 NotesDocumento20 pagineLipids 31 2012 Notesapi-178321548Nessuna valutazione finora
- Chapter: One: Introduction and Aim of The ThesisDocumento12 pagineChapter: One: Introduction and Aim of The ThesislichenresearchNessuna valutazione finora
- The Logic of Chemical SynthesisDocumento462 pagineThe Logic of Chemical SynthesisJohnny KrazeNessuna valutazione finora
- EicosanoidsDocumento4 pagineEicosanoidsFrancis GathiraNessuna valutazione finora
- Nonsteroidal Anti-Inflammatory Drugs: DR Tarek M Nasrallah Al - AzharDocumento97 pagineNonsteroidal Anti-Inflammatory Drugs: DR Tarek M Nasrallah Al - AzharTarek NasrallahNessuna valutazione finora
- Non Steroidal Anti Inflammatory Drugs: NsaidsDocumento58 pagineNon Steroidal Anti Inflammatory Drugs: NsaidsmahamoudNessuna valutazione finora
- Topic 2. Pharmacology For Pain and Inflammation RDocumento52 pagineTopic 2. Pharmacology For Pain and Inflammation RKendrick GalosoNessuna valutazione finora
- Aspectos Fisiopatologicos Da InflamaçãoDocumento25 pagineAspectos Fisiopatologicos Da InflamaçãoMaria das Dores BarretoNessuna valutazione finora
- Prostaglandin: Continued DonationsDocumento27 pagineProstaglandin: Continued DonationsrajeevmkNessuna valutazione finora
- Screenshot 2022-06-13 at 16.29.48Documento34 pagineScreenshot 2022-06-13 at 16.29.48Indira NoormaliyaNessuna valutazione finora
- Burn UnitDocumento206 pagineBurn UnitJeisson Osorio Trujillo100% (1)
- Pharmacodynamics and PharmacokineticsDocumento99 paginePharmacodynamics and PharmacokineticsMAMA LALANessuna valutazione finora
- Pain Relievers TGDocumento26 paginePain Relievers TGLilis nurhayatiNessuna valutazione finora
- Fatty Acids and Polyketides PaperDocumento62 pagineFatty Acids and Polyketides PaperKarina Narciso100% (1)
- BylawsDocumento136 pagineBylawsdannyfiguracion45Nessuna valutazione finora
- Eicosanoids: (Prostaglandins, Thromboxanes, Leukotrienes)Documento26 pagineEicosanoids: (Prostaglandins, Thromboxanes, Leukotrienes)BOsch VakilNessuna valutazione finora
- Recent Advances in Anaesthesia and Intensive CareDocumento323 pagineRecent Advances in Anaesthesia and Intensive CaresurasuarezlopezNessuna valutazione finora
- Conservation Therapy (Celibacy)Documento9 pagineConservation Therapy (Celibacy)ShivamMishraNessuna valutazione finora
- Prostaglandins, Immunoglobulins: Prepared by Dr. Poonam MondalDocumento10 pagineProstaglandins, Immunoglobulins: Prepared by Dr. Poonam MondalPoonam MondalNessuna valutazione finora
- Inflammation and Inflammatory MediatorsDocumento40 pagineInflammation and Inflammatory MediatorsQuty Papa KannaNessuna valutazione finora