Potrebbero piacerti anche
- Persistence and Evolution of Sars-Cov-2 in An Immunocompromised HostDocumento3 paginePersistence and Evolution of Sars-Cov-2 in An Immunocompromised HostIsro AlhaqiNessuna valutazione finora
- Surgical Treatment of Secondary Peritonitis: A Continuing ProblemDocumento6 pagineSurgical Treatment of Secondary Peritonitis: A Continuing ProblemAstutikNessuna valutazione finora
- 1 SMDocumento6 pagine1 SMVenus BoacNessuna valutazione finora
- Allegranzi-Benedetta HH Escmid PDFDocumento92 pagineAllegranzi-Benedetta HH Escmid PDFNishanth.sNessuna valutazione finora
- Znad 019Documento2 pagineZnad 019Daniel ŘehákNessuna valutazione finora
- Suppression o F Interferon Production by Vitamin A: (Accepted 22 March 1976)Documento5 pagineSuppression o F Interferon Production by Vitamin A: (Accepted 22 March 1976)shailendraraviNessuna valutazione finora
- Neutralization of The Sars-Cov-2 Mu Variant by Convalescent and Vaccine SerumDocumento3 pagineNeutralization of The Sars-Cov-2 Mu Variant by Convalescent and Vaccine SerumSuwandi ChangNessuna valutazione finora
- Quiz 3 MicroeconomicsDocumento3 pagineQuiz 3 MicroeconomicsNguyễn Đức ThắngNessuna valutazione finora
- 2016-A Prospective Evaluation of Acute Toxicity From Proton Therapy For Targets of The Parotid RegionDocumento6 pagine2016-A Prospective Evaluation of Acute Toxicity From Proton Therapy For Targets of The Parotid Regionabidabatoolmunir4Nessuna valutazione finora
- Kali Carbonicum 6cH Controls Malassezia PachydermaDocumento8 pagineKali Carbonicum 6cH Controls Malassezia Pachydermamounir5025Nessuna valutazione finora
- Figura 3 PDFDocumento28 pagineFigura 3 PDFE Yamelie MartínezNessuna valutazione finora
- Management of Hypercoagulable State During Pregnancy. Prophylactic Usage of Low Molecular Weight Heparin (LMWH)Documento7 pagineManagement of Hypercoagulable State During Pregnancy. Prophylactic Usage of Low Molecular Weight Heparin (LMWH)Aita AladianseNessuna valutazione finora
- Tuberculosis in Developing Countries: Dilemmas: Erik Post, MD MSC Royal Tropical Institute AmsterdamDocumento23 pagineTuberculosis in Developing Countries: Dilemmas: Erik Post, MD MSC Royal Tropical Institute Amsterdamgaruda unriNessuna valutazione finora
- Mechanism of Action of Methotrexate in Rheumatoid Arthritis, and The Search For BiomarkersDocumento12 pagineMechanism of Action of Methotrexate in Rheumatoid Arthritis, and The Search For BiomarkersFaMe TanapornNessuna valutazione finora
- 0850 Adam MED BdImYaK YG - OipkDocumento66 pagine0850 Adam MED BdImYaK YG - OipkFlaviusNessuna valutazione finora
- Singanayagam Et Al 2020Documento5 pagineSinganayagam Et Al 2020JefersonMatosdeColaresNessuna valutazione finora
- Palm Fisting, Thrombophlebitis, IV Cannulated Patient, VIP Score (Visual Infusion Phlebitis)Documento8 paginePalm Fisting, Thrombophlebitis, IV Cannulated Patient, VIP Score (Visual Infusion Phlebitis)Manashi SenguptaNessuna valutazione finora
- Dead Recovered Confirmed Tested Hotline: Situation Report NoDocumento12 pagineDead Recovered Confirmed Tested Hotline: Situation Report NoSusan ArafatNessuna valutazione finora
- Predictive Value of IL-28B rs12979860 Variants For peg-IFN, Sofosbuvir Plus Ribavirin Treatment of HCV Infection in Pakistani PopulationDocumento8 paginePredictive Value of IL-28B rs12979860 Variants For peg-IFN, Sofosbuvir Plus Ribavirin Treatment of HCV Infection in Pakistani PopulationThanh PhongNessuna valutazione finora
- Perioperative Management For A Patient With Severe Congenital Factor V Deficiency Undergoing Cochlear ImplantationDocumento3 paginePerioperative Management For A Patient With Severe Congenital Factor V Deficiency Undergoing Cochlear ImplantationInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Chapter 16: Tetanus: I. Disease DescriptionDocumento7 pagineChapter 16: Tetanus: I. Disease DescriptionTina MorleyNessuna valutazione finora
- Multiple Choice Questions: ST RDDocumento6 pagineMultiple Choice Questions: ST RDAbdulrab SaeedNessuna valutazione finora
- J. Mech. Phys. SolidsDocumento5 pagineJ. Mech. Phys. SolidsLeonardo Fernandes PinheiroNessuna valutazione finora
- Jama Wang 2020 LD 200077 1597432994.04794Documento2 pagineJama Wang 2020 LD 200077 1597432994.04794LyonTrioréNessuna valutazione finora
- Original Article: A Clinical and Microbial Study of Otomycosis: An Original StudyDocumento9 pagineOriginal Article: A Clinical and Microbial Study of Otomycosis: An Original StudywennyrhyNessuna valutazione finora
- A Comparative Study of Propofol and Thiopentone With Local Anaesthetic Spray As Inducing Agents For I-Gel InsertionDocumento6 pagineA Comparative Study of Propofol and Thiopentone With Local Anaesthetic Spray As Inducing Agents For I-Gel InsertionIJAR JOURNALNessuna valutazione finora
- Research PaperDocumento6 pagineResearch Papersajanagamage95Nessuna valutazione finora
- Rashighi 2014Documento11 pagineRashighi 2014DORIS Z.Nessuna valutazione finora
- CDD 2014117Documento11 pagineCDD 2014117Soumia ZtNessuna valutazione finora
- Identification of A Molnupiravir-Associated Mutational Signature in SARS-CoV-2 Sequencing DatabasesDocumento14 pagineIdentification of A Molnupiravir-Associated Mutational Signature in SARS-CoV-2 Sequencing Databaseshansley cookNessuna valutazione finora
- Leu 201323Documento10 pagineLeu 201323haemophilicNessuna valutazione finora
- The Potential of Triterpenoids in The Treatment of MelanomaDocumento35 pagineThe Potential of Triterpenoids in The Treatment of MelanomaValentina D BrunaNessuna valutazione finora
- Growth and Investment: 25000 5000 6000 7000 New Cases (7 Day MA) Total Deaths (RHS)Documento16 pagineGrowth and Investment: 25000 5000 6000 7000 New Cases (7 Day MA) Total Deaths (RHS)Rk SunnyNessuna valutazione finora
- Thromboembolic Disease During Tuberculosis: A Series of 47 CasesDocumento6 pagineThromboembolic Disease During Tuberculosis: A Series of 47 CasesIJAR JOURNALNessuna valutazione finora
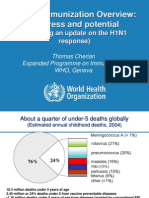
- Global Immunization Overview: Progress and PotentialDocumento36 pagineGlobal Immunization Overview: Progress and PotentialPrabir Kumar ChatterjeeNessuna valutazione finora
- Mecan 1 - Marcado TotalDocumento6 pagineMecan 1 - Marcado TotalVictor RoticivNessuna valutazione finora
- Cancer Nature OtimoDocumento20 pagineCancer Nature OtimoGlauce L TrevisanNessuna valutazione finora
- Muhammad Faez Othman - 2021340765 - Extended - AbstractDocumento4 pagineMuhammad Faez Othman - 2021340765 - Extended - Abstract9fc58h9qvvNessuna valutazione finora
- Statistical Report Name School Date ProfessorDocumento8 pagineStatistical Report Name School Date ProfessoraraceliNessuna valutazione finora
- Session 538 PDFDocumento34 pagineSession 538 PDFMed MedNessuna valutazione finora
- Bechat (5), Andrews (6) and Others: Printed N U.S.ADocumento4 pagineBechat (5), Andrews (6) and Others: Printed N U.S.AAldhy D'souljaNessuna valutazione finora
- Tratamientos AlveolitisDocumento3 pagineTratamientos AlveolitisMAR�A JOS� CASTILLO MORALESNessuna valutazione finora
- Glioblastoma Educational Needs SurveyDocumento8 pagineGlioblastoma Educational Needs Surveyapi-52940597Nessuna valutazione finora
- Padda2020 Article TheNeurologicalComplexitiesAndDocumento12 paginePadda2020 Article TheNeurologicalComplexitiesAndSebastian Tabares RodriguezNessuna valutazione finora
- Beir Lant 2010Documento7 pagineBeir Lant 2010Taniya SahaNessuna valutazione finora
- Slides ENG For Session 673Documento70 pagineSlides ENG For Session 673joelccmmNessuna valutazione finora
- Who Bangladesh Covid 19 Sitrep 13 20200525 PDFDocumento12 pagineWho Bangladesh Covid 19 Sitrep 13 20200525 PDFmk mayen kurishyNessuna valutazione finora
- Antimicrobial Agents and Chemotherapy-1986-Agnelli-1108.fullDocumento2 pagineAntimicrobial Agents and Chemotherapy-1986-Agnelli-1108.fullHusna MorradNessuna valutazione finora
- Burney 1975Documento4 pagineBurney 1975Candra YogiswaraNessuna valutazione finora
- Coronavirus World 27.04.2020Documento15 pagineCoronavirus World 27.04.2020jayNessuna valutazione finora
- Coronavirus Update 21.04.2020Documento20 pagineCoronavirus Update 21.04.2020jayNessuna valutazione finora
- Mamas 2Documento6 pagineMamas 2DIOGENESNessuna valutazione finora
- Hepatocarcinoma 2Documento23 pagineHepatocarcinoma 2NaraMayhumiDeBelenMerinoOrtizNessuna valutazione finora
- Nosocomial Infections in EgyptDocumento47 pagineNosocomial Infections in Egyptlordoftheweb100% (1)
- Domingo Chiva2017Documento4 pagineDomingo Chiva2017alyssa azzahraNessuna valutazione finora
- Baricitinib Frena La Desregulación Inmunitaria en Pacientes Con COVID-19 GraveDocumento8 pagineBaricitinib Frena La Desregulación Inmunitaria en Pacientes Con COVID-19 GraveByron VarasNessuna valutazione finora
- PAHO - Recurring Waves and Outbreaks of COVID-19 - 9 October 2020Documento11 paginePAHO - Recurring Waves and Outbreaks of COVID-19 - 9 October 2020tomaspont7743Nessuna valutazione finora
- Lessons From The Coronavirus Disease 2019 Pandemic: Will Virtual Patient Management Reshape Uro-Oncology in Germany?Documento5 pagineLessons From The Coronavirus Disease 2019 Pandemic: Will Virtual Patient Management Reshape Uro-Oncology in Germany?Ion CorbuNessuna valutazione finora
- 10.1038@s41590 019 0578 8Documento15 pagine10.1038@s41590 019 0578 8Rodrigo RicoNessuna valutazione finora
- Ketamina IntranasalDocumento14 pagineKetamina IntranasalFederico García VillagómezNessuna valutazione finora
- Iota ScandalDocumento124 pagineIota ScandalFederico García VillagómezNessuna valutazione finora
- Commonalities and Differences in The Research On Children's Effortful Control and Executive Function A Call For An Integrated Model of Self-RegulationDocumento10 pagineCommonalities and Differences in The Research On Children's Effortful Control and Executive Function A Call For An Integrated Model of Self-RegulationFederico García VillagómezNessuna valutazione finora
- The Health Effects of Cannabis and Cannabinoids (2017)Documento395 pagineThe Health Effects of Cannabis and Cannabinoids (2017)Cannabis Israel100% (3)
- Inhibitory Control Over Action and MemoryDocumento11 pagineInhibitory Control Over Action and MemoryMaryam TaqaviNessuna valutazione finora
- Laboratory Manual of Biopharmaceutics and Pharmacokinetics - 1 PDFDocumento167 pagineLaboratory Manual of Biopharmaceutics and Pharmacokinetics - 1 PDFkdk;lkd33% (3)
- Phytochemistry (Introduction, Plant Metabolites and PhytochemicalDocumento48 paginePhytochemistry (Introduction, Plant Metabolites and Phytochemicalanisahanifatinr100% (1)
- 1 s2.0 S1319562X19300968 MainDocumento11 pagine1 s2.0 S1319562X19300968 MainRobert TriarjunetNessuna valutazione finora
- Cell Disruption Extracting Target Product: Location of Biological ProductsDocumento88 pagineCell Disruption Extracting Target Product: Location of Biological ProductsRoshan jaiswalNessuna valutazione finora
- Treatment Knowledge Ramadhan SeriesDocumento2 pagineTreatment Knowledge Ramadhan SeriesAbrisha Agung WicaksonoNessuna valutazione finora
- Glycogenesis and GlycogenolysisDocumento55 pagineGlycogenesis and Glycogenolysisclear mindNessuna valutazione finora
- Anas Muaamar Jeff Ludovico BIOL 1406.SL7 EnzymesDocumento5 pagineAnas Muaamar Jeff Ludovico BIOL 1406.SL7 Enzymesblackrose0Nessuna valutazione finora
- Sylvia Wynter & Katherine Mckittrick - On-Being-Human-As-Praxis PDFDocumento66 pagineSylvia Wynter & Katherine Mckittrick - On-Being-Human-As-Praxis PDFfirexcracker100% (1)
- Chang2013 Morphometric Analysis of The Cranial Base in AsiansDocumento8 pagineChang2013 Morphometric Analysis of The Cranial Base in Asianssolodont1Nessuna valutazione finora
- General Anatomy Syllabus PDFDocumento3 pagineGeneral Anatomy Syllabus PDFSara SultanaNessuna valutazione finora
- G10 Nervous System DLPDocumento5 pagineG10 Nervous System DLPBAD-E, JUSTINE ALEXIS BALBUENANessuna valutazione finora
- Lab Report # 1 - HOMEOSTASISDocumento17 pagineLab Report # 1 - HOMEOSTASISLaw Light50% (4)
- Form InspeksiDocumento8 pagineForm Inspeksiichsan syahputraNessuna valutazione finora
- Si RNADocumento29 pagineSi RNALuis MonteroNessuna valutazione finora
- UCSP Graded Recitation QuestionsDocumento4 pagineUCSP Graded Recitation QuestionsDarrel Susaya100% (1)
- (1479683X - European Journal of Endocrinology) MECHANISMS IN ENDOCRINOLOGY - Autoimmune Thyroid Disease - Old and New PlayersDocumento12 pagine(1479683X - European Journal of Endocrinology) MECHANISMS IN ENDOCRINOLOGY - Autoimmune Thyroid Disease - Old and New PlayersIoana BodescuNessuna valutazione finora
- Exercise PhysiologyDocumento37 pagineExercise PhysiologyAndre Christian Sopacua67% (3)
- Spermatogenesis PPTDocumento42 pagineSpermatogenesis PPTInsatiable CleeNessuna valutazione finora
- Allometry Proposal 1.1 - RevisedDocumento11 pagineAllometry Proposal 1.1 - RevisedAnonymous 7BpT9OWPNessuna valutazione finora
- Grouping Living OrganismsDocumento8 pagineGrouping Living OrganismsOsmany MadrigalNessuna valutazione finora
- Molsoft Icm Quarterly: How To Perform Ligand-Based Screening Using Atomic Property FieldsDocumento4 pagineMolsoft Icm Quarterly: How To Perform Ligand-Based Screening Using Atomic Property FieldsMolSoftNessuna valutazione finora
- M.04 Modes of Inheritance and Pedigree AnalysisDocumento4 pagineM.04 Modes of Inheritance and Pedigree Analysisno veNessuna valutazione finora
- MT DNA AND SEQUENCINGDocumento2 pagineMT DNA AND SEQUENCINGNived K KNessuna valutazione finora
- AriaMx Launch Data Sheet - 5991-5151ENDocumento2 pagineAriaMx Launch Data Sheet - 5991-5151ENSadar JayaNessuna valutazione finora
- Enzymes PDFDocumento13 pagineEnzymes PDFPaul MarloweNessuna valutazione finora
- Science: Second Quarter - Module 2Documento30 pagineScience: Second Quarter - Module 2Mujeres Virglius Pablius89% (9)
- SOL BIO Anatomical Evidence of Evolution Henry PriceDocumento7 pagineSOL BIO Anatomical Evidence of Evolution Henry PriceHenry PriceNessuna valutazione finora
- On The Equilibrium of Living Beings by Means of Reciprocal Destruction by Lorenzo CameranoDocumento30 pagineOn The Equilibrium of Living Beings by Means of Reciprocal Destruction by Lorenzo Cameranodiego_griffonNessuna valutazione finora
- Hematology and Coagulation Controls: Your Quality Goals RealizedDocumento15 pagineHematology and Coagulation Controls: Your Quality Goals RealizedBenn BasilNessuna valutazione finora