Potrebbero piacerti anche
- A Study Guide for Denise Levertov's "A Tree Telling of Orpheus"Da EverandA Study Guide for Denise Levertov's "A Tree Telling of Orpheus"Nessuna valutazione finora
- Cardiovascular Pathology: Professor Mircea BuruianDocumento174 pagineCardiovascular Pathology: Professor Mircea BuruianDiana PopoviciNessuna valutazione finora
- The Casting Director: by Kate McclanaghanDocumento3 pagineThe Casting Director: by Kate McclanaghanmaniNessuna valutazione finora
- Eng DramaDocumento76 pagineEng DramaAndy AngelNessuna valutazione finora
- Dotnet FrameworkDocumento60 pagineDotnet FrameworkHarishNessuna valutazione finora
- PolaroidDocumento117 paginePolaroidcbanNessuna valutazione finora
- An Inspector CallsDocumento121 pagineAn Inspector CallsJeberouyusufNessuna valutazione finora
- WaldenDocumento32 pagineWaldennjb2808Nessuna valutazione finora
- Notes: 1. Roots and ContextsDocumento39 pagineNotes: 1. Roots and Contextsmimo72Nessuna valutazione finora
- 123 ScriptDocumento113 pagine123 ScriptGabe GirsonNessuna valutazione finora
- SKMBT C45221051211580Documento49 pagineSKMBT C45221051211580Κατερίνα ΜαρούδηNessuna valutazione finora
- Official High School Thespian Point SystemDocumento2 pagineOfficial High School Thespian Point Systemapi-262302841Nessuna valutazione finora
- Willhebop StandardDocumento72 pagineWillhebop StandardCole BuzbeeNessuna valutazione finora
- Samuel French Sample Perusal: WWW - Samuelfrench.co - UkDocumento42 pagineSamuel French Sample Perusal: WWW - Samuelfrench.co - UkpanchkapunchNessuna valutazione finora
- Diagnostic Imaging: Medical RadiologyDocumento299 pagineDiagnostic Imaging: Medical RadiologyEdith CroitoruNessuna valutazione finora
- Call Sheet UtaDocumento308 pagineCall Sheet Utaakemi babyNessuna valutazione finora
- Margolin Deb Oh, I WillDocumento13 pagineMargolin Deb Oh, I WillLjubisa MaticNessuna valutazione finora
- Textbook of Neuroimaging PDFDocumento403 pagineTextbook of Neuroimaging PDFAli Radhi MutarNessuna valutazione finora
- Scarlet Script PDFDocumento74 pagineScarlet Script PDFSarahNessuna valutazione finora
- A Figment by Ron Weaver ScriptDocumento7 pagineA Figment by Ron Weaver ScriptcheshiecNessuna valutazione finora
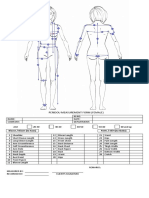
- Peridou Measurement Form (Female) : Blouse / Blazer (Sa Itaas) Pants / Skirt (Sa Ibaba)Documento1 paginaPeridou Measurement Form (Female) : Blouse / Blazer (Sa Itaas) Pants / Skirt (Sa Ibaba)tt324Nessuna valutazione finora
- Uganda Local NamesDocumento40 pagineUganda Local NamesAiuba SuleimanaNessuna valutazione finora
- Fundaments of Video SignalsDocumento5 pagineFundaments of Video SignalsMonique DeleonNessuna valutazione finora
- History of Television CondensedDocumento4 pagineHistory of Television CondensedAndreea KiddoNessuna valutazione finora
- Creating A Role PDFDocumento296 pagineCreating A Role PDFEledir SantosNessuna valutazione finora
- Dead Mans Cell Phone AnalysisDocumento4 pagineDead Mans Cell Phone Analysisapi-272640625Nessuna valutazione finora
- CardiovascularDocumento80 pagineCardiovascularhajarhaniyahNessuna valutazione finora
- Chest XrayDocumento31 pagineChest XrayBiscuits and milkNessuna valutazione finora
- Chest RadiologyDocumento129 pagineChest RadiologyNadiya SafitriNessuna valutazione finora
- Cardiac Interpretation of Pediatric Chest X-Ray: Key FactsDocumento19 pagineCardiac Interpretation of Pediatric Chest X-Ray: Key FactsTry ArieNessuna valutazione finora
- Cor Radiology (Kuliah Cardiovascular) 2011Documento51 pagineCor Radiology (Kuliah Cardiovascular) 2011athayafebNessuna valutazione finora
- Medicine 2:: Phase IIIADocumento53 pagineMedicine 2:: Phase IIIAMatyie SmkasNessuna valutazione finora
- Cardiovascular Pathology FINALDocumento45 pagineCardiovascular Pathology FINALIanNessuna valutazione finora
- BF - PJB - Yaf Mel Tia NiaDocumento20 pagineBF - PJB - Yaf Mel Tia NiaRoberto HutapeaNessuna valutazione finora
- Cardiovascular ImagingDocumento97 pagineCardiovascular ImagingWai Kwong ChiuNessuna valutazione finora
- SMJ 59 279Documento5 pagineSMJ 59 279Faradiba MaricarNessuna valutazione finora
- Cardiac Imaging-AnatomyDocumento27 pagineCardiac Imaging-AnatomyfatimaNessuna valutazione finora
- Normal ChestDocumento82 pagineNormal ChestMonica CherladyNessuna valutazione finora
- Physiologic Considerations in CHD: Cardiac ProblemsDocumento2 paginePhysiologic Considerations in CHD: Cardiac ProblemszhwahNessuna valutazione finora
- Cardiac RadiologyDocumento17 pagineCardiac Radiologytam meiNessuna valutazione finora
- Topic 10 CVSDocumento10 pagineTopic 10 CVSSneha GaneshNessuna valutazione finora
- Cor PulmonaleDocumento42 pagineCor PulmonaleNym Angga SantosaNessuna valutazione finora
- Kuliah Radiologi Cardiorespiratory 2Documento99 pagineKuliah Radiologi Cardiorespiratory 2Muhammad Sandy Ali YafieNessuna valutazione finora
- Kuliah 16 Cor PulmonaleDocumento41 pagineKuliah 16 Cor PulmonalecaturwiraNessuna valutazione finora
- X-Ray CVSDocumento67 pagineX-Ray CVSmdjohariNessuna valutazione finora
- 14 08 11.CV Anatomy Histology - Gundogan.Documento6 pagine14 08 11.CV Anatomy Histology - Gundogan.allisonNessuna valutazione finora
- Cardiovascular DiseasesDocumento49 pagineCardiovascular DiseasesSHAMENI VINODNessuna valutazione finora
- Chest Imaging IDocumento173 pagineChest Imaging Ikathi raja sekharNessuna valutazione finora
- Congestive Heart FailureDocumento11 pagineCongestive Heart Failurepvs5155Nessuna valutazione finora
- X Ray SchemeDocumento6 pagineX Ray SchemeIdiAmadouNessuna valutazione finora
- Congenital Heart Disease: MashuriDocumento31 pagineCongenital Heart Disease: MashuriAlvienz SaputraNessuna valutazione finora
- Cardiovascular ImagingDocumento64 pagineCardiovascular Imagingfitrah fajrianiNessuna valutazione finora
- 1.conginital Cardiac DefectsDocumento39 pagine1.conginital Cardiac DefectsJõsëph Jåy MîthNessuna valutazione finora
- Döş TopografiDocumento56 pagineDöş TopografiMahammad UsbaliyevNessuna valutazione finora
- Cardiovascular ExaminationDocumento127 pagineCardiovascular Examinationwakemeup143Nessuna valutazione finora
- Congenital Heart DiseaseDocumento13 pagineCongenital Heart DiseaseRaja86% (7)
- Atrial and Ventral Septal DefectDocumento3 pagineAtrial and Ventral Septal DefectJessica Carmela CasugaNessuna valutazione finora
- Cardiac Congenital DiseaseDocumento27 pagineCardiac Congenital Diseasenovitafitri123Nessuna valutazione finora
- PA Projection AP ProjectionDocumento64 paginePA Projection AP ProjectionMiaMDNessuna valutazione finora
- Micros 1Documento20 pagineMicros 1api-19916399Nessuna valutazione finora
- Tropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaDocumento95 pagineTropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaadystiNessuna valutazione finora
- 10 Tahapan Pidi - 16042016Documento1 pagina10 Tahapan Pidi - 16042016adystiNessuna valutazione finora
- Cutaneous Larval MigransDocumento24 pagineCutaneous Larval MigransadystiNessuna valutazione finora
- Erythrosquamous Diseases / Papulosquamous DiseasesDocumento38 pagineErythrosquamous Diseases / Papulosquamous DiseasesadystiNessuna valutazione finora
- Dermatomycosis 2009Documento29 pagineDermatomycosis 2009adystiNessuna valutazione finora
- House Dust Mites DLLDocumento32 pagineHouse Dust Mites DLLadystiNessuna valutazione finora
- Poisoning DecontaminationDocumento14 paginePoisoning DecontaminationadystiNessuna valutazione finora
- Peripheral Arterial Occlusive DiseaseDocumento49 paginePeripheral Arterial Occlusive DiseaseadystiNessuna valutazione finora
- Peripheral Arterial Occlusive DiseaseDocumento43 paginePeripheral Arterial Occlusive DiseaseadystiNessuna valutazione finora
- Venom (Insect Bite, Snake Bite, Dog Bite)Documento23 pagineVenom (Insect Bite, Snake Bite, Dog Bite)adystiNessuna valutazione finora
- Tobacco LectureDocumento36 pagineTobacco LecturesenoNessuna valutazione finora
- Vaccine Preventable Diseases (VPDS) : Ida Safitri Laksono Dept of Child Health Infectious Disease Sub DivisionDocumento26 pagineVaccine Preventable Diseases (VPDS) : Ida Safitri Laksono Dept of Child Health Infectious Disease Sub DivisionadystiNessuna valutazione finora
- Vasculer Imaging 2012 PDFDocumento72 pagineVasculer Imaging 2012 PDFadystiNessuna valutazione finora
- Amblyopia Inter Blok 22Documento30 pagineAmblyopia Inter Blok 22adystiNessuna valutazione finora
- Drug AllergyDocumento61 pagineDrug Allergyadysti100% (1)
- Peripheral Arterial Occlusive DiseaseDocumento43 paginePeripheral Arterial Occlusive DiseaseadystiNessuna valutazione finora
- VTE Prophylaxis in The Hospital: Johan KurniandaDocumento35 pagineVTE Prophylaxis in The Hospital: Johan KurniandaadystiNessuna valutazione finora
- AFP - Blok 3.4. IndoDocumento36 pagineAFP - Blok 3.4. IndoadystiNessuna valutazione finora
- Dermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDocumento34 pagineDermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityadystiNessuna valutazione finora
- 1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesDocumento67 pagine1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesadystiNessuna valutazione finora
- Fever in Children 2010Documento27 pagineFever in Children 2010adystiNessuna valutazione finora
- Genito Urinary Problems in Children: Bagian Ilmu Kesehatan Kulit & Kelamin Fakultas Kedokteran UGM YogyakartaDocumento78 pagineGenito Urinary Problems in Children: Bagian Ilmu Kesehatan Kulit & Kelamin Fakultas Kedokteran UGM YogyakartaadystiNessuna valutazione finora
- Immunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityDocumento35 pagineImmunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityadystiNessuna valutazione finora
- Imunol InfeksiDocumento26 pagineImunol InfeksiadystiNessuna valutazione finora
- Patient Autonomy: Competent and Incompetent Patient and Research Participant To ConsentDocumento27 paginePatient Autonomy: Competent and Incompetent Patient and Research Participant To ConsentadystiNessuna valutazione finora
- Alrg 10 PDFDocumento59 pagineAlrg 10 PDFadystiNessuna valutazione finora
- Oportunistic in ElderlyDocumento19 pagineOportunistic in ElderlyadystiNessuna valutazione finora
- Eritro ADocumento40 pagineEritro AadystiNessuna valutazione finora
- Aging and Endocrine DisordersDocumento23 pagineAging and Endocrine DisordersadystiNessuna valutazione finora
- BasicImmunol PDFDocumento56 pagineBasicImmunol PDFadystiNessuna valutazione finora
- 5090 w13 Ms 62 PDFDocumento5 pagine5090 w13 Ms 62 PDFJotaro kujoNessuna valutazione finora
- Creativity Sphere - 84Documento5 pagineCreativity Sphere - 84prudhvitapmiNessuna valutazione finora
- JurnalkuDocumento5 pagineJurnalkuAgis CliquersNessuna valutazione finora
- Physiology of Weight Regulation: Louis Chaptini and Steven PeikinDocumento4 paginePhysiology of Weight Regulation: Louis Chaptini and Steven PeikinjonruNessuna valutazione finora
- Circulatory SystemDocumento25 pagineCirculatory SystemadnanNessuna valutazione finora
- A Study of Efficiency of Breathing Exercises To Improve Pulmonary FX in SCi PtsDocumento6 pagineA Study of Efficiency of Breathing Exercises To Improve Pulmonary FX in SCi PtsMarion AtienzaNessuna valutazione finora
- The Difficult or Failed Airway: Pat Melanson, MDDocumento28 pagineThe Difficult or Failed Airway: Pat Melanson, MDMinorC3Nessuna valutazione finora
- C2 - Anatomy of The Pain Processing SystemDocumento9 pagineC2 - Anatomy of The Pain Processing SystemFabricio BorbaNessuna valutazione finora
- Abdominal Distention inDocumento45 pagineAbdominal Distention inArif Rahman DmNessuna valutazione finora
- Hands OnDocumento3 pagineHands Onapi-26135524Nessuna valutazione finora
- Fermentation Lesson Plan 1Documento3 pagineFermentation Lesson Plan 1api-571580523Nessuna valutazione finora
- Nurse EcmoDocumento124 pagineNurse EcmoSalvatore Cimino100% (5)
- Typhoid FeverDocumento23 pagineTyphoid FeverMaden Jayona HaliliNessuna valutazione finora
- Prevalance of Smoking Among Male Medical Students of Sheikh Zayed Medical College Rahim Yar KhanDocumento32 paginePrevalance of Smoking Among Male Medical Students of Sheikh Zayed Medical College Rahim Yar KhanHamza RoohaniNessuna valutazione finora
- Muscle: Duchenne Muscular DystrophyDocumento13 pagineMuscle: Duchenne Muscular DystrophyMicke RodriguezNessuna valutazione finora
- How Do You Sleep EbookDocumento68 pagineHow Do You Sleep Ebookgabitor100% (1)
- Lab. Ing. Genética 5Documento12 pagineLab. Ing. Genética 5Jose MaresNessuna valutazione finora
- 16 Respiratory AlkalosisDocumento28 pagine16 Respiratory AlkalosisJoel Topf100% (2)
- Algoritma CHFDocumento1 paginaAlgoritma CHFdiany astutiNessuna valutazione finora
- Care of Client in Mechanical VentilatorDocumento11 pagineCare of Client in Mechanical VentilatorVignesh Viggy100% (4)
- 2020 08 10 Sanjay Pandarbale Yogesh Nerkar Sufala MalnekarDocumento4 pagine2020 08 10 Sanjay Pandarbale Yogesh Nerkar Sufala MalnekarYogesh NerkarNessuna valutazione finora
- Apiculture - CH 1 - 9Documento127 pagineApiculture - CH 1 - 9Mll HaileNessuna valutazione finora
- Zly106 CA Questions & Answers by Evans Kelly & DiligeceDocumento40 pagineZly106 CA Questions & Answers by Evans Kelly & DiligeceSHERIFF BAKARENessuna valutazione finora
- Philips Heartstart XL Plus Defibrillator ManualDocumento235 paginePhilips Heartstart XL Plus Defibrillator ManualvikasNessuna valutazione finora
- Radiologi SinusitisDocumento42 pagineRadiologi SinusitisMonic GultomNessuna valutazione finora
- Motility Disorders of EsophagusDocumento44 pagineMotility Disorders of EsophagusmackieccNessuna valutazione finora
- Essential Newborn CareDocumento5 pagineEssential Newborn CareJig PirameNessuna valutazione finora
- Healing of Bone and Cartilage FracturesDocumento36 pagineHealing of Bone and Cartilage Fracturescatharinam100% (1)
- Practice Questions BBCDocumento3 paginePractice Questions BBCBT20CME033 Gautam TahilyaniNessuna valutazione finora
- Surgical Case Study: CranioplastyDocumento50 pagineSurgical Case Study: Cranioplastyrhia casinillo100% (8)