Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Professional Service ProjectDocumento2 pagineProfessional Service Projectapi-428652649Nessuna valutazione finora
- Right Submandibular GlandDocumento1 paginaRight Submandibular Glandapi-428652649Nessuna valutazione finora
- Electron CompDocumento3 pagineElectron Compapi-428652649Nessuna valutazione finora
- Detail 11504 2117910Documento5 pagineDetail 11504 2117910api-428652649Nessuna valutazione finora
- 1 StfallevalDocumento5 pagine1 Stfallevalapi-432489466Nessuna valutazione finora
- Larynx CertificateDocumento1 paginaLarynx Certificateapi-428652649Nessuna valutazione finora
- Tally 1Documento2 pagineTally 1api-428652649Nessuna valutazione finora
- Limb SarcomaDocumento3 pagineLimb Sarcomaapi-428652649Nessuna valutazione finora
- Zabdominal ImrtDocumento3 pagineZabdominal Imrtapi-431732695Nessuna valutazione finora
- Zabdominal ImrtDocumento3 pagineZabdominal Imrtapi-431732695Nessuna valutazione finora
- Lymphoma CompDocumento3 pagineLymphoma Compapi-428652649Nessuna valutazione finora
- Conformal Lung With BoostDocumento3 pagineConformal Lung With Boostapi-428652649Nessuna valutazione finora
- Zabdominal ImrtDocumento3 pagineZabdominal Imrtapi-431732695Nessuna valutazione finora
- Research Organization DocumentDocumento7 pagineResearch Organization Documentapi-428652649Nessuna valutazione finora
- Para-Aortic CompDocumento3 paginePara-Aortic Compapi-428652649Nessuna valutazione finora
- RoilsDocumento3 pagineRoilsapi-428652649Nessuna valutazione finora
- Reserach PaperDocumento14 pagineReserach Paperapi-428652649Nessuna valutazione finora
- Service EmployerDocumento5 pagineService Employerapi-428652649Nessuna valutazione finora
- Para-Aortic CompDocumento3 paginePara-Aortic Compapi-428652649Nessuna valutazione finora
- Case LogDocumento2 pagineCase Logapi-428652649Nessuna valutazione finora
- Practice Problems Weeks 1 2 For StudentsDocumento1 paginaPractice Problems Weeks 1 2 For Studentsapi-337168367Nessuna valutazione finora
- SclavDocumento3 pagineSclavapi-428652649Nessuna valutazione finora
- Proknow Prostate PlanDocumento9 pagineProknow Prostate Planapi-428652649Nessuna valutazione finora
- Prostate With NodesDocumento3 pagineProstate With Nodesapi-428652649Nessuna valutazione finora
- H N CompDocumento3 pagineH N Compapi-428652649Nessuna valutazione finora
- Case Log Semester 1Documento2 pagineCase Log Semester 1api-428652649Nessuna valutazione finora
- Interstitial BrachyDocumento3 pagineInterstitial Brachyapi-428652649Nessuna valutazione finora
- IntracavDocumento3 pagineIntracavapi-428652649Nessuna valutazione finora
- Affective Eval 3Documento3 pagineAffective Eval 3api-428652649Nessuna valutazione finora
- Pelvis Gyn CanvasDocumento2 paginePelvis Gyn Canvasapi-428652649Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Physics Part-2Documento14 paginePhysics Part-2Thor hmNessuna valutazione finora
- PART 74 Weldolet Sweepolet Something About WeldoletDocumento9 paginePART 74 Weldolet Sweepolet Something About Weldoletravindra_jivaniNessuna valutazione finora
- Dometic-Varc - 72 Instal ManualDocumento48 pagineDometic-Varc - 72 Instal Manualstefan tulucNessuna valutazione finora
- HVAC Course PDFDocumento273 pagineHVAC Course PDFliliNessuna valutazione finora
- "Enron Energy Scandal": Assignment ONDocumento11 pagine"Enron Energy Scandal": Assignment ONDarshan GohilNessuna valutazione finora
- Purple Line Traction Power Study Report-Rev4Documento38 paginePurple Line Traction Power Study Report-Rev4曾乙申100% (3)
- ABB - OPR Lightning - p31-p31Documento1 paginaABB - OPR Lightning - p31-p31Indra WanNessuna valutazione finora
- Free Energy GeneratorDocumento2 pagineFree Energy GeneratorAamir ShaikhNessuna valutazione finora
- SAPPHIRE® PLUS 70-BarDocumento2 pagineSAPPHIRE® PLUS 70-BarAyhan ÖZKALNessuna valutazione finora
- Developments in Thermal Desalination Processes PDFDocumento14 pagineDevelopments in Thermal Desalination Processes PDFG.DNessuna valutazione finora
- 0111 SunSwitch - OFFER FOR - 1 KVA TO 8 KVA Solar Hybrid PCUDocumento8 pagine0111 SunSwitch - OFFER FOR - 1 KVA TO 8 KVA Solar Hybrid PCUGaurav KhannaNessuna valutazione finora
- Kush Nir 2019Documento6 pagineKush Nir 2019Gustavo FloresNessuna valutazione finora
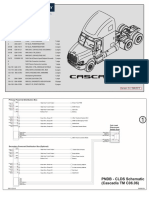
- Cascadia PrtPak 09AUG13Documento44 pagineCascadia PrtPak 09AUG13Raul LunaNessuna valutazione finora
- Encorp Group ServicesDocumento26 pagineEncorp Group ServicesVinay NowalNessuna valutazione finora
- Fundamentals of HV Circuit-BreakersDocumento22 pagineFundamentals of HV Circuit-BreakersBastian OspinaNessuna valutazione finora
- Sugar ManufacturingDocumento55 pagineSugar Manufacturingamrialifa100% (3)
- Assignment#2, Potential, Capacitors, Magnetic Force and FieldDocumento5 pagineAssignment#2, Potential, Capacitors, Magnetic Force and FieldBilal KhalidNessuna valutazione finora
- Vijay Singh CVDocumento2 pagineVijay Singh CVVijay ChauhanNessuna valutazione finora
- ABB Inverter ACS 150Documento130 pagineABB Inverter ACS 150Joe Electricneutron100% (1)
- Prepared By: Mr. Harsh PanchalDocumento46 paginePrepared By: Mr. Harsh PanchalKáûshàl PãtëlNessuna valutazione finora
- Target MonetaryDocumento9 pagineTarget MonetaryKuldeep RupareliaNessuna valutazione finora
- CH 1Documento6 pagineCH 1Dineshsingh ThakurNessuna valutazione finora
- Measuring The Pour Point of Crude Oils: Manual MethodDocumento1 paginaMeasuring The Pour Point of Crude Oils: Manual MethodSamuel OlonadeNessuna valutazione finora
- Survey Questionnaire On Transforming Recycled Cooking Oil Into A Sustainable Butane Alternative For Stove FuelDocumento2 pagineSurvey Questionnaire On Transforming Recycled Cooking Oil Into A Sustainable Butane Alternative For Stove Fueljohnphilipcornelio04Nessuna valutazione finora
- KAT0815-0001-E Single Pole Insulated Conductor RailDocumento36 pagineKAT0815-0001-E Single Pole Insulated Conductor RailirinaNessuna valutazione finora
- Jahn-Teller Distortion and Coordination Number FourDocumento15 pagineJahn-Teller Distortion and Coordination Number FourAldi JonataNessuna valutazione finora
- Evolution Spas Manual ENG-19 PDFDocumento44 pagineEvolution Spas Manual ENG-19 PDFAnonymous 0aFzcZ100% (1)
- Investigation of Technical and Economic Aspects For Methanol Production Through CO2 Hydrogenation PDFDocumento13 pagineInvestigation of Technical and Economic Aspects For Methanol Production Through CO2 Hydrogenation PDFCarlosNessuna valutazione finora
- 2 Stroke Diesel Engine Components-1Documento72 pagine2 Stroke Diesel Engine Components-1EdemNessuna valutazione finora
- N468190, DCD996Documento60 pagineN468190, DCD996Luís A. BlancoNessuna valutazione finora