Potrebbero piacerti anche
- Regaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryDa EverandRegaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryNessuna valutazione finora
- Img 0527Documento2 pagineImg 0527Beatrice KoesmarsonoNessuna valutazione finora
- PDocumento1 paginaPbryan.zabala.mnlNessuna valutazione finora
- Chap 23Documento25 pagineChap 23Ghazian AdliNessuna valutazione finora
- Surgery of The AppendixDocumento5 pagineSurgery of The AppendixJoseph De JoyaNessuna valutazione finora
- Jurnal OG 1Documento6 pagineJurnal OG 1Wa Ode Meutya ZawawiNessuna valutazione finora
- FP 34 08 33Documento3 pagineFP 34 08 33ZakiNessuna valutazione finora
- AN - Fistula in Ano PDFDocumento27 pagineAN - Fistula in Ano PDFGiana DeviNessuna valutazione finora
- (AI) Exploratory CeliotomyDocumento8 pagine(AI) Exploratory CeliotomyCASANDRA ELIABETH PONCE VAZQUEZNessuna valutazione finora
- INGUINAL HERNIAS - Short Surgery PresentationDocumento11 pagineINGUINAL HERNIAS - Short Surgery Presentationq6hzqsf2hfNessuna valutazione finora
- Slide Hernia 2003Documento24 pagineSlide Hernia 2003anfaNessuna valutazione finora
- Undescended Testes: What General Practitioners Need To KnowDocumento4 pagineUndescended Testes: What General Practitioners Need To KnowRizka Desti AyuniNessuna valutazione finora
- (Surgery) Midterms PediatricsDocumento5 pagine(Surgery) Midterms Pediatricsalmira.s.mercadoNessuna valutazione finora
- Testicular Torsion, Peds Cases NotesDocumento1 paginaTesticular Torsion, Peds Cases NotesdzalhcNessuna valutazione finora
- Intussusception TransDocumento4 pagineIntussusception TransJames Maravillas100% (1)
- Patent Omphalomesenteric Duct: Sectioning The UnexpectedDocumento2 paginePatent Omphalomesenteric Duct: Sectioning The UnexpectedpratiwifatmasariNessuna valutazione finora
- Ajcr 2010 1 4Documento3 pagineAjcr 2010 1 4Muhammad Bilal MirzaNessuna valutazione finora
- Tuberculous Peritonitis Presenting As An Acute Abdomen: A Case ReportDocumento4 pagineTuberculous Peritonitis Presenting As An Acute Abdomen: A Case ReportDumitru RadulescuNessuna valutazione finora
- Intestinal ObstructionDocumento59 pagineIntestinal ObstructionGeorge GuruNessuna valutazione finora
- Backup of LO 2 DD HERNIA - Id.en-2Documento3 pagineBackup of LO 2 DD HERNIA - Id.en-2dianNessuna valutazione finora
- Paeds Bilious VomitingDocumento2 paginePaeds Bilious Vomitingsinghurvashi365Nessuna valutazione finora
- 1 s2.0 S0749072015307350 MainDocumento10 pagine1 s2.0 S0749072015307350 Mainsapryh24Nessuna valutazione finora
- Hand InfectionDocumento5 pagineHand InfectionElhamNessuna valutazione finora
- Impaired Urinary EliminationDocumento2 pagineImpaired Urinary EliminationSiafei RabeNessuna valutazione finora
- Eop 4Documento6 pagineEop 4ayunisallehNessuna valutazione finora
- 4 Artículo Revisión - Hernias Inguinales en NiñosDocumento6 pagine4 Artículo Revisión - Hernias Inguinales en NiñosNICOLLE ENAMORADO ENCISONessuna valutazione finora
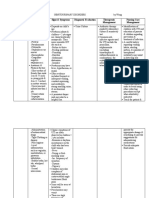
- Name: Gerald Age: 3 Years Old Current Diagnosis: Imperforate Anus Nursing Care Plan Cues/Clues Nursing Diagnosis Planning Nursing Intervention Rationale EvaluationDocumento2 pagineName: Gerald Age: 3 Years Old Current Diagnosis: Imperforate Anus Nursing Care Plan Cues/Clues Nursing Diagnosis Planning Nursing Intervention Rationale EvaluationKyle VargasNessuna valutazione finora
- Nursing Care Plan For Peritonitis NCPDocumento2 pagineNursing Care Plan For Peritonitis NCPyamie sulongNessuna valutazione finora
- Power Doppler Sonographic Diagnosis of Torsion in A Wandering SpleenDocumento3 paginePower Doppler Sonographic Diagnosis of Torsion in A Wandering SpleendenisegmeloNessuna valutazione finora
- 6 SURGERY II 6 - Pediatric UrologyDocumento6 pagine6 SURGERY II 6 - Pediatric UrologyDeann RoscomNessuna valutazione finora
- 7.6 Undescended Testis Inguinal HerniaDocumento7 pagine7.6 Undescended Testis Inguinal HerniaΜατθαίος ΠαππάςNessuna valutazione finora
- Gastroenterology Colon CancerDocumento1 paginaGastroenterology Colon CancerNour SamadNessuna valutazione finora
- Rare Foreign Bodies in Lower Urinary Tract and Management Poster - USICON 2021Documento1 paginaRare Foreign Bodies in Lower Urinary Tract and Management Poster - USICON 2021Somanath SharmaNessuna valutazione finora
- Gynecological Assessment: DateDocumento4 pagineGynecological Assessment: Dateanne laureNessuna valutazione finora
- GenitoDocumento12 pagineGenitofatima_antonioNessuna valutazione finora
- Annsurg01229 0099 PDFDocumento4 pagineAnnsurg01229 0099 PDFDiego ReyNessuna valutazione finora
- Parurethral CystsDocumento3 pagineParurethral CystsIoannis ValioulisNessuna valutazione finora
- Surgery Subspecialty - Peds First DayDocumento2 pagineSurgery Subspecialty - Peds First DayJonathan AiresNessuna valutazione finora
- Gastrointestinal System DiseasesDocumento6 pagineGastrointestinal System DiseasesHazel ConjeNessuna valutazione finora
- HERNIA Dr. Medina 1 PDFDocumento4 pagineHERNIA Dr. Medina 1 PDFKaren ChristiaansNessuna valutazione finora
- (Aganglionic Megacolon) : Hirschsprung'S DiseaseDocumento2 pagine(Aganglionic Megacolon) : Hirschsprung'S DiseaseLalisaM ActivityNessuna valutazione finora
- Vesico Vaginal FistulaDocumento6 pagineVesico Vaginal Fistulaapi-3705046Nessuna valutazione finora
- Obstetrics - Neoplastic Disease of The Ovary (Epithelial) 2014 FinalDocumento3 pagineObstetrics - Neoplastic Disease of The Ovary (Epithelial) 2014 FinalJonathanNessuna valutazione finora
- Ureteroureterostomy For Reflux Duplex SystemsDocumento5 pagineUreteroureterostomy For Reflux Duplex Systemsjithin rNessuna valutazione finora
- Delay in Diagnosis of Congenital Anal ST PDFDocumento4 pagineDelay in Diagnosis of Congenital Anal ST PDFJimi Kalvin SarareniNessuna valutazione finora
- Pediatric Surg TransDocumento4 paginePediatric Surg TransSven OrdanzaNessuna valutazione finora
- Anorectal MalformationDocumento4 pagineAnorectal MalformationFawzia Haznah Nurul ImaniNessuna valutazione finora
- HirschprungDocumento13 pagineHirschprungfitra hayatiNessuna valutazione finora
- 2.4.5.2.3.a Bowel ObstructionDocumento35 pagine2.4.5.2.3.a Bowel ObstructionProject ByNessuna valutazione finora
- Intestine ObstructionDocumento37 pagineIntestine ObstructionGoesti YudistiraNessuna valutazione finora
- Diagnosis and Correction of Uterine Torsion in Cattle and BuffaloesDocumento7 pagineDiagnosis and Correction of Uterine Torsion in Cattle and BuffaloesGovind Narayan PurohitNessuna valutazione finora
- 6255 24879 1 PBDocumento2 pagine6255 24879 1 PBSyafatesia nicky pratiwiNessuna valutazione finora
- Abdominal Assessment HA LectureDocumento44 pagineAbdominal Assessment HA LectureKatrina BeltranNessuna valutazione finora
- GynecoDocumento3 pagineGynecoanne laureNessuna valutazione finora
- Intestinal Obstruction 2019Documento8 pagineIntestinal Obstruction 2019olakasturiNessuna valutazione finora
- Hirschprung's DiseaseDocumento26 pagineHirschprung's DiseaseAbdur RaqibNessuna valutazione finora
- Suh 2016Documento4 pagineSuh 2016Christian Leonardo Molina HinojosaNessuna valutazione finora
- Pelvic Organ ProlapseDocumento5 paginePelvic Organ Prolapsecgao30Nessuna valutazione finora
- (Surg3b) Pediatric Surgery (Resurreccion) - PauzkiDocumento13 pagine(Surg3b) Pediatric Surgery (Resurreccion) - PauzkiAra CasalsNessuna valutazione finora
- Examination of A StomaDocumento3 pagineExamination of A StomaChloe100% (1)
- JurnalDocumento6 pagineJurnalnao thaNessuna valutazione finora
- Jadwal Kepaniteraan Klinik Neuroemergency Nov-Des PDFDocumento4 pagineJadwal Kepaniteraan Klinik Neuroemergency Nov-Des PDFnao thaNessuna valutazione finora
- Jadwal Kepaniteraan Klinik Neuroemergency Nov-Des PDFDocumento4 pagineJadwal Kepaniteraan Klinik Neuroemergency Nov-Des PDFnao thaNessuna valutazione finora
- 27 34 PDFDocumento8 pagine27 34 PDFMusdah MulyaNessuna valutazione finora
- What Is New in API 610 11th EdDocumento6 pagineWhat Is New in API 610 11th EdAnonymous 1XHScfCINessuna valutazione finora
- Commissioning Valve Product BrochureDocumento14 pagineCommissioning Valve Product BrochureblindjaxxNessuna valutazione finora
- Supplier S Documentation of Equipment PDFDocumento32 pagineSupplier S Documentation of Equipment PDFzhangjieNessuna valutazione finora
- Interzinc 2280 Product BrochureDocumento4 pagineInterzinc 2280 Product BrochureAshish Raul CIENessuna valutazione finora
- Marshall Abby - Chess Cafe - The Openings Explained - 1-63, 2015-OCR, 682pDocumento682 pagineMarshall Abby - Chess Cafe - The Openings Explained - 1-63, 2015-OCR, 682pArtur MałkowskiNessuna valutazione finora
- Learn Horse Riding: at HPRCDocumento16 pagineLearn Horse Riding: at HPRCAkashNessuna valutazione finora
- Fuel Tank Truck Afd-091005-058Documento40 pagineFuel Tank Truck Afd-091005-058cascade1100% (1)
- HP 300s+ Scientific Calculator: Sophisticated Design Ideal For Math and Science StudentsDocumento3 pagineHP 300s+ Scientific Calculator: Sophisticated Design Ideal For Math and Science StudentsgemaNessuna valutazione finora
- Drugs and Tinnitus - Neil Bauman PHD - April '09Documento2 pagineDrugs and Tinnitus - Neil Bauman PHD - April '09DownTheTheRabbitHole108Nessuna valutazione finora
- Technical Datasheet: ENGUARD™ BP 75 ARF Multi Purpose Bonding Paste With FibresDocumento2 pagineTechnical Datasheet: ENGUARD™ BP 75 ARF Multi Purpose Bonding Paste With FibresFernando Cesar PérezNessuna valutazione finora
- Feeg2003 L21Documento9 pagineFeeg2003 L21jiales225Nessuna valutazione finora
- Ficha Tecnica p501Documento4 pagineFicha Tecnica p501LizbethNessuna valutazione finora
- Sound Healing For Health and Well - BeingDocumento36 pagineSound Healing For Health and Well - Beingtormenta7azul6225100% (9)
- Hearst Tower - New York City: Frank J. Dimauro Envs 662-660 Richard W. Berman Project: BuildingsDocumento6 pagineHearst Tower - New York City: Frank J. Dimauro Envs 662-660 Richard W. Berman Project: BuildingsMohamed FawzyNessuna valutazione finora
- Daniel Madison - BreachDocumento8 pagineDaniel Madison - Breachmrbookman3Nessuna valutazione finora
- Pediatric Airway ManagementDocumento2 paginePediatric Airway ManagementSilvy AmaliaNessuna valutazione finora
- 0900-9914 I1 201012 PDFDocumento132 pagine0900-9914 I1 201012 PDFIvan Arjona50% (2)
- Mat11 PDFDocumento13 pagineMat11 PDFRaquel Martins E SilvaNessuna valutazione finora
- Polymer Structures: Issues To Address..Documento34 paginePolymer Structures: Issues To Address..Eugene Embalzado Jr.Nessuna valutazione finora
- 2nd Round Selected StudentsDocumento1 pagina2nd Round Selected StudentsSiri KRNessuna valutazione finora
- Role of BisoprololDocumento43 pagineRole of BisoprololFidel Martua Marpaung67% (3)
- Biochemistry - Syllabus Marks EtcDocumento8 pagineBiochemistry - Syllabus Marks EtcshahzebNessuna valutazione finora
- Handwriting Analysis EbookDocumento154 pagineHandwriting Analysis EbookG.100% (5)
- R K Konodia Civil Gate Previous Year - by EasyEngineering - Net 1 PDFDocumento214 pagineR K Konodia Civil Gate Previous Year - by EasyEngineering - Net 1 PDFDaante VermaNessuna valutazione finora
- R0221120 - Salsabilla Cindy Pratama - Daily ActivityDocumento15 pagineR0221120 - Salsabilla Cindy Pratama - Daily Activitysalsabilla cindy pratamaNessuna valutazione finora
- Laura Gentile Letter On Hampden County CourthouseDocumento6 pagineLaura Gentile Letter On Hampden County CourthouseMassLiveNessuna valutazione finora
- Patel, Anita - Super Indian Snack and Street Food Recipes PDFDocumento117 paginePatel, Anita - Super Indian Snack and Street Food Recipes PDFBella ImèneNessuna valutazione finora
- MH2732-Robotics Lab ManualDocumento50 pagineMH2732-Robotics Lab Manualramzi ayadiNessuna valutazione finora
- Baño - Griferia - KOHLER - K-74013M+0.50GPMDocumento3 pagineBaño - Griferia - KOHLER - K-74013M+0.50GPMGiordano Tuanama YapoNessuna valutazione finora
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 3.5 su 5 stelle3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4 su 5 stelle4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDa EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningValutazione: 4 su 5 stelle4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nessuna valutazione finora
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerDa EverandGut: the new and revised Sunday Times bestsellerValutazione: 4 su 5 stelle4/5 (393)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- The Marshmallow Test: Mastering Self-ControlDa EverandThe Marshmallow Test: Mastering Self-ControlValutazione: 4.5 su 5 stelle4.5/5 (58)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (328)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDa EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingValutazione: 4 su 5 stelle4/5 (1138)
- Troubled: A Memoir of Foster Care, Family, and Social ClassDa EverandTroubled: A Memoir of Foster Care, Family, and Social ClassValutazione: 4.5 su 5 stelle4.5/5 (27)