Potrebbero piacerti anche
- Pharmacology of Sex SteroidsDocumento40 paginePharmacology of Sex Steroidsmus zaharaNessuna valutazione finora
- Estrogen and AndrogenDocumento32 pagineEstrogen and AndrogenkwennybiangNessuna valutazione finora
- Hormone Replacement TherapyDocumento6 pagineHormone Replacement TherapyDimpal Choudhary67% (3)
- Female Sex HormonesDocumento20 pagineFemale Sex HormonesAlina ShahNessuna valutazione finora
- Drugs 2 (Gyneac)Documento103 pagineDrugs 2 (Gyneac)Aman Shaikh100% (2)
- Male and Female HormonesDocumento26 pagineMale and Female HormonesZuha HundalNessuna valutazione finora
- Hormones and Related Drugs: Mechanism of ActionDocumento21 pagineHormones and Related Drugs: Mechanism of ActionaviraaworldNessuna valutazione finora
- Androgen-Antiandrogen - DR Asep SukoharDocumento61 pagineAndrogen-Antiandrogen - DR Asep SukoharLeon L GayaNessuna valutazione finora
- Contraception Lec 1Documento38 pagineContraception Lec 1fh2785519Nessuna valutazione finora
- Oral Contraceptives PDFDocumento24 pagineOral Contraceptives PDFSheema TabassumNessuna valutazione finora
- Dr. J. Schober PHPT 742 2012 618-650-5129: Joschob@siue - EduDocumento30 pagineDr. J. Schober PHPT 742 2012 618-650-5129: Joschob@siue - EduNik ShaughnessyNessuna valutazione finora
- Presentation 1Documento58 paginePresentation 1Kuch Bhi50% (2)
- HRTDocumento62 pagineHRTArpita ArpitaNessuna valutazione finora
- New Estrogen and ProgesteroneDocumento56 pagineNew Estrogen and ProgesteroneHBrNessuna valutazione finora
- Menstruation Disorders in Adolescents Medication - EDocumento8 pagineMenstruation Disorders in Adolescents Medication - Edr. Martinus Harrys Budi Poernama GiawaNessuna valutazione finora
- The Gonadal Hormones & InhibitorsDocumento41 pagineThe Gonadal Hormones & InhibitorsSaddamix AL OmariNessuna valutazione finora
- Gonadal HormonesDocumento40 pagineGonadal HormonesJoyce VillanuevaNessuna valutazione finora
- 01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)Documento46 pagine01 Lecture 9 Gonadal Hormones and Drugs (Pod Pharm DR Thatcher 2022)sahilaminNessuna valutazione finora
- Ovulation Induction: Embryo Clinic, Krasnodar, RussiaDocumento2 pagineOvulation Induction: Embryo Clinic, Krasnodar, RussiaAsh AmeNessuna valutazione finora
- Femara: (Letrozole Tablets) 2.5 MG Tablets RX Only Prescribing InformationDocumento28 pagineFemara: (Letrozole Tablets) 2.5 MG Tablets RX Only Prescribing InformationKirubakaranNessuna valutazione finora
- The Gonadal Hormones & Inhibitors: by M.H.Farjoo M.D., PH.DDocumento133 pagineThe Gonadal Hormones & Inhibitors: by M.H.Farjoo M.D., PH.DsajidNessuna valutazione finora
- AntiandrogensDocumento22 pagineAntiandrogenstheintrovNessuna valutazione finora
- Metabolic and Endocrine Pharmacology: Gonadol DrugsDocumento38 pagineMetabolic and Endocrine Pharmacology: Gonadol Drugstheintrov100% (1)
- Barrier Methods Hormonal Methods Oral Contraceptives Vaginal Rings Implants, Injectables Withdrawal and AbstinenceDocumento37 pagineBarrier Methods Hormonal Methods Oral Contraceptives Vaginal Rings Implants, Injectables Withdrawal and AbstinenceEm WalkerNessuna valutazione finora
- Recent Developments in Contraceptives: Dr.M.M.Misro Department of Reproductive BiomedicineDocumento57 pagineRecent Developments in Contraceptives: Dr.M.M.Misro Department of Reproductive BiomedicineLinguumNessuna valutazione finora
- Bazedoxifene Drugs Therapeutics CommitteeDocumento3 pagineBazedoxifene Drugs Therapeutics CommitteepiNessuna valutazione finora
- Anticancer Hormones & AntagonistsDocumento27 pagineAnticancer Hormones & AntagonistsBob MuneneNessuna valutazione finora
- K16 - Pharmacology of Hormonal ContraceptionDocumento51 pagineK16 - Pharmacology of Hormonal Contraceptiondhiyas100% (1)
- LoetteDocumento15 pagineLoetteHaque XiangNessuna valutazione finora
- Estrogens and AndrogensDocumento26 pagineEstrogens and AndrogensGwenny DumpNessuna valutazione finora
- Reproductive Pharmacology Lecturio ReflectionDocumento7 pagineReproductive Pharmacology Lecturio ReflectionNathaniel SolisNessuna valutazione finora
- Hormonal Advances OlufemiDocumento90 pagineHormonal Advances OlufemiDare Olalekan AnthonyNessuna valutazione finora
- Pharcomology of Oral ContraceptionDocumento22 paginePharcomology of Oral Contraceptioncana geel 2018Nessuna valutazione finora
- Type of ProgestinDocumento4 pagineType of ProgestinBrenda LiawNessuna valutazione finora
- Cheryl Burdette - Its Not The Hormone But Its Home 05072017 AZDocumento97 pagineCheryl Burdette - Its Not The Hormone But Its Home 05072017 AZtemp001bunnNessuna valutazione finora
- Comparative Efficacy of Cyproterone/EE Vs Desogestrel/EE On Acne in PCOD: A Hospital Based Study On 40 PatientsDocumento4 pagineComparative Efficacy of Cyproterone/EE Vs Desogestrel/EE On Acne in PCOD: A Hospital Based Study On 40 PatientsGayathriNessuna valutazione finora
- Induction and Maintenance of Amenorrhea in Transmasculine and Nonbinary AdolescentsDocumento6 pagineInduction and Maintenance of Amenorrhea in Transmasculine and Nonbinary AdolescentsdespalitaNessuna valutazione finora
- Hormone Therapy: The Basics: What Are Hormones and How Are They Used As Therapy?Documento4 pagineHormone Therapy: The Basics: What Are Hormones and How Are They Used As Therapy?Ubaidillah Romadlon AlfairuziNessuna valutazione finora
- Hormonal Contraception (Ahp)Documento46 pagineHormonal Contraception (Ahp)burhanNessuna valutazione finora
- Treatment Options January 2022 - 0 PDFDocumento11 pagineTreatment Options January 2022 - 0 PDFadenantNessuna valutazione finora
- CerazetteDocumento36 pagineCerazetteSuhazeli AbdullahNessuna valutazione finora
- Clinical Endocrinology - 2020 - Angus - A Systematic Review of Antiandrogens and Feminization in Transgender WomenDocumento10 pagineClinical Endocrinology - 2020 - Angus - A Systematic Review of Antiandrogens and Feminization in Transgender WomenGiuseppe NuciferoNessuna valutazione finora
- COCP ChoicesDocumento22 pagineCOCP ChoicesKarin ElenaNessuna valutazione finora
- Sex Hormones PDFDocumento54 pagineSex Hormones PDFmohsen mirdamadiNessuna valutazione finora
- Estrogen ProgesteronDocumento12 pagineEstrogen Progesterondokter wawanNessuna valutazione finora
- Estradiol Valerate + Dienogest PDFDocumento6 pagineEstradiol Valerate + Dienogest PDFJuan FernandezNessuna valutazione finora
- Male HormonesDocumento30 pagineMale Hormonesmjawadullah5Nessuna valutazione finora
- Treatment of Menopausal Symptoms With Hormone TherapyDocumento34 pagineTreatment of Menopausal Symptoms With Hormone TherapyJennifer estefania sigcha pujotaNessuna valutazione finora
- Menstrual Disorders and ContraceptionDocumento77 pagineMenstrual Disorders and ContraceptionRukaya AlshamiNessuna valutazione finora
- Drugs Used in Reproductive Health: Estrogen and ProgestinDocumento41 pagineDrugs Used in Reproductive Health: Estrogen and ProgestindrfatimarizNessuna valutazione finora
- 10.2478 - Enr 2019 0023Documento6 pagine10.2478 - Enr 2019 0023DNessuna valutazione finora
- Anderson 2002Documento10 pagineAnderson 2002GemiNessuna valutazione finora
- The Progestins All SimilarDocumento23 pagineThe Progestins All SimilarVladimir KljajevicNessuna valutazione finora
- Contraception 14 April 2014Documento74 pagineContraception 14 April 2014danielNessuna valutazione finora
- Gonadal enDocumento60 pagineGonadal enm7md TotiaNessuna valutazione finora
- CONTRACEPTIONDocumento38 pagineCONTRACEPTIONGopala HariNessuna valutazione finora
- Product Information Proviron: CH OH CHDocumento6 pagineProduct Information Proviron: CH OH CHDNessuna valutazione finora
- Selection of Oral Contraceptive PillsDocumento3 pagineSelection of Oral Contraceptive PillsbebytycoNessuna valutazione finora
- Animal Birth Control in Canine (Non-Surgical Interventions)Documento19 pagineAnimal Birth Control in Canine (Non-Surgical Interventions)Kirti JamwalNessuna valutazione finora
- Piis0002934317309324 PDFDocumento8 paginePiis0002934317309324 PDFRenato KaindoyNessuna valutazione finora
- Netics of Eye ColorDocumento2 pagineNetics of Eye ColorSergi Verdés FranquesaNessuna valutazione finora
- Making Yogurt at Home: What Is Yogurt? Health Benefits From ProbioticsDocumento4 pagineMaking Yogurt at Home: What Is Yogurt? Health Benefits From ProbioticsKeeranmayeeishraNessuna valutazione finora
- Review ArticleDocumento10 pagineReview ArticleKeeranmayeeishraNessuna valutazione finora
- How To Read Music Notes Qlcss Pp1 9 DunnDocumento9 pagineHow To Read Music Notes Qlcss Pp1 9 DunnMuhammad Sollehen MisnanNessuna valutazione finora
- How To Hand Wash PosterDocumento1 paginaHow To Hand Wash Posterzamkhual100% (1)
- Instructions-Menstrual Cup-Types and UsesDocumento2 pagineInstructions-Menstrual Cup-Types and UsesKeeranmayeeishraNessuna valutazione finora
- Bashh WartsDocumento19 pagineBashh WartsKeeranmayeeishraNessuna valutazione finora
- Example Icu CV PDFDocumento6 pagineExample Icu CV PDFKeeranmayeeishraNessuna valutazione finora
- 001 HIDE and SEEK Free Childrens BookDocumento27 pagine001 HIDE and SEEK Free Childrens BookDhanasekaran VadivalaganNessuna valutazione finora
- Doppler in ObstetricsDocumento162 pagineDoppler in ObstetricsbadbearpstNessuna valutazione finora
- How To Read Music Notes Qlcss Pp1 9 DunnDocumento9 pagineHow To Read Music Notes Qlcss Pp1 9 DunnMuhammad Sollehen MisnanNessuna valutazione finora
- Can Love Happentwice Ebook Full Version Download PDF Ravinder Singh2 PDFDocumento114 pagineCan Love Happentwice Ebook Full Version Download PDF Ravinder Singh2 PDFKeeranmayeeishraNessuna valutazione finora
- Pi Obstetric CholestasisDocumento5 paginePi Obstetric CholestasisSanaNessuna valutazione finora
- WHO Report On COVID-19 - April 24, 2020Documento12 pagineWHO Report On COVID-19 - April 24, 2020CityNewsTorontoNessuna valutazione finora
- Neet Patttern PointsDocumento9 pagineNeet Patttern PointskarthiktsvmcNessuna valutazione finora
- Diagnosis and Management of Cervical InsufficiencyDocumento8 pagineDiagnosis and Management of Cervical InsufficiencyKeeranmayeeishraNessuna valutazione finora
- 18-23 Weeks Scan PDFDocumento135 pagine18-23 Weeks Scan PDFAlvaro Dario Verdugo UnigarroNessuna valutazione finora
- Bhatla Et Al-2019-International Journal of Gynecology & ObstetricsDocumento7 pagineBhatla Et Al-2019-International Journal of Gynecology & ObstetricsJerico SantosNessuna valutazione finora
- Get Started With Dropbox PDFDocumento10 pagineGet Started With Dropbox PDFReka ErdantoNessuna valutazione finora
- 0714 Obg Manuck PDFDocumento9 pagine0714 Obg Manuck PDFKeeranmayeeishraNessuna valutazione finora
- PegDocumento21 paginePegandy wongNessuna valutazione finora
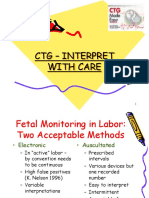
- CTG - Interpret With CareDocumento55 pagineCTG - Interpret With CareKeeranmayeeishraNessuna valutazione finora
- FT LSCS ArpithaDocumento2 pagineFT LSCS ArpithaKeeranmayeeishraNessuna valutazione finora
- A Night at The Museum: Roll Up ! Roll Up! Museums IncDocumento1 paginaA Night at The Museum: Roll Up ! Roll Up! Museums IncKeeranmayeeishraNessuna valutazione finora
- How To Become A Super Learner by Jim Kwik WorkbookDocumento11 pagineHow To Become A Super Learner by Jim Kwik WorkbookKeeranmayeeishraNessuna valutazione finora
- The Conscious Parent Transforming Ourselves Empowering Our ChildrenDocumento198 pagineThe Conscious Parent Transforming Ourselves Empowering Our ChildrenNatalija Gligoric100% (19)
- March 2017 RecallDocumento62 pagineMarch 2017 RecallSaeed HasanNessuna valutazione finora
- Mark Twain QuotesDocumento1 paginaMark Twain QuotesBen ChongNessuna valutazione finora
- Tog 12539Documento6 pagineTog 12539KeeranmayeeishraNessuna valutazione finora
- Handbook of Nonprescription Drugs - Ch44 Hair LossDocumento19 pagineHandbook of Nonprescription Drugs - Ch44 Hair LossKatyNessuna valutazione finora
- Role of Food and Exercise in Polycystic Ovarian SyndromeDocumento3 pagineRole of Food and Exercise in Polycystic Ovarian SyndromeInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Uerm Board Review - ObDocumento15 pagineUerm Board Review - ObCamilla FernandezNessuna valutazione finora
- Pcos GP Tool 2dec2013Documento6 paginePcos GP Tool 2dec2013Maram AbdullahNessuna valutazione finora
- Polycystic Ovary Syndrome: Dr. Gurpreet KaurDocumento57 paginePolycystic Ovary Syndrome: Dr. Gurpreet KaurPiyush Agarwal100% (1)
- Pcos ApprovedDocumento30 paginePcos ApprovedEsha BhatiaNessuna valutazione finora
- 2021 Clinical Practice Guidelines On The Diagnosis and Management of Polycystic OvaryDocumento11 pagine2021 Clinical Practice Guidelines On The Diagnosis and Management of Polycystic OvarySalma Yuri KhairunnisaNessuna valutazione finora
- Polycystic Ovarian SyndromeDocumento11 paginePolycystic Ovarian Syndromezianab aliNessuna valutazione finora
- Ovarian CystsDocumento28 pagineOvarian CystsMuhammad AbeeshNessuna valutazione finora
- OBSTETRICSMock BoardsDocumento17 pagineOBSTETRICSMock BoardsDominque RabastoNessuna valutazione finora
- PCOS Patient HandoutDocumento16 paginePCOS Patient HandoutAnonymous NI5oJfd2cNessuna valutazione finora
- Polycystic Ovary SyndromeDocumento17 paginePolycystic Ovary SyndromeramsaybajjuNessuna valutazione finora
- Divine Intervention Episode 22 Obgyn Shelf Review PDFDocumento167 pagineDivine Intervention Episode 22 Obgyn Shelf Review PDFSwisskelly1100% (1)
- Survey of Poly Cystic Ovarian Disease (PCOD) Among The Girl Students of Bishop Heber College, Trichirapalli, Tamil Nadu, IndiaDocumento9 pagineSurvey of Poly Cystic Ovarian Disease (PCOD) Among The Girl Students of Bishop Heber College, Trichirapalli, Tamil Nadu, IndiayooyoNessuna valutazione finora
- Pcos Infertility Ayurveda ApproachDocumento3 paginePcos Infertility Ayurveda ApproachAlna TechnicalNessuna valutazione finora
- Final-5 Ayurvedic - Treatment - of - Polycystic - Ovary - Syndrome - PCOS-2022-02-16-08-23Documento4 pagineFinal-5 Ayurvedic - Treatment - of - Polycystic - Ovary - Syndrome - PCOS-2022-02-16-08-23Deepak KumarNessuna valutazione finora
- Polycystic Ovary SyndromeDocumento13 paginePolycystic Ovary SyndromeNAYSHA YANET CHAVEZ RONDINELNessuna valutazione finora
- Assessment of Body Fat Composition Parameters in Women of Polycystic Ovary Syndrome (Pcos) : A Case - Control StudyDocumento7 pagineAssessment of Body Fat Composition Parameters in Women of Polycystic Ovary Syndrome (Pcos) : A Case - Control StudyIJAR JOURNALNessuna valutazione finora
- Child RoomDocumento21 pagineChild RoomAnoop RajNessuna valutazione finora
- Polycystic Ovarian Syndrome (PCOS)Documento119 paginePolycystic Ovarian Syndrome (PCOS)Jasani JayrajNessuna valutazione finora
- Metformin Use in Women With Polycystic Ovary Syndrome: Neil P. JohnsonDocumento6 pagineMetformin Use in Women With Polycystic Ovary Syndrome: Neil P. JohnsonanyNessuna valutazione finora
- 09-2013 UTpt EndoDocumento44 pagine09-2013 UTpt Endomina0% (1)
- Primary Amenorrhea Is Failure of Menses To Occur by One of The FollowingDocumento13 paginePrimary Amenorrhea Is Failure of Menses To Occur by One of The FollowingMuhammad Ilyas AhmadNessuna valutazione finora
- Jurnal 2Documento25 pagineJurnal 2Ade Yurga TonaraNessuna valutazione finora
- GynaecologyDocumento123 pagineGynaecologyKiranNessuna valutazione finora
- Sop Jcem 2013Documento28 pagineSop Jcem 2013Leonard MendonçaNessuna valutazione finora
- Polycystic Ovarian SyndromeDocumento2 paginePolycystic Ovarian SyndromeCarlo CruzNessuna valutazione finora
- Rajiv Gandhi University of Health SciencesDocumento14 pagineRajiv Gandhi University of Health SciencesJalajarani AridassNessuna valutazione finora
- AmenorrheaDocumento41 pagineAmenorrheaarfahregarNessuna valutazione finora