Potrebbero piacerti anche
- Mind Wars ArtDocumento3 pagineMind Wars ArtBeth Book ReviewNessuna valutazione finora
- Alcohol and Violence: The Nature of the Relationship and the Promise of PreventionDa EverandAlcohol and Violence: The Nature of the Relationship and the Promise of PreventionNessuna valutazione finora
- Aspects of the Dialogical Self: Extended proceedings of a symposium on the Second International Conference on the Dialogical Self (Ghent, Oct. 2002), including psycholonguistical, conversational, and educational contributionsDa EverandAspects of the Dialogical Self: Extended proceedings of a symposium on the Second International Conference on the Dialogical Self (Ghent, Oct. 2002), including psycholonguistical, conversational, and educational contributionsMarie C BertauNessuna valutazione finora
- Incident Reports of Harassment, Vandalism, Hacking, & Thefts From 1987 To March 22, 2010Documento476 pagineIncident Reports of Harassment, Vandalism, Hacking, & Thefts From 1987 To March 22, 2010Stan J. CaterboneNessuna valutazione finora
- Task Force On Sexual Assault and Interpersonal Violence Final Report 2014-15Documento16 pagineTask Force On Sexual Assault and Interpersonal Violence Final Report 2014-15Fourth EstateNessuna valutazione finora
- Autism and Sexual Issues: A Survival Guide For People With Asperger's SyndromeDocumento2 pagineAutism and Sexual Issues: A Survival Guide For People With Asperger's SyndromeJohannaCraneDeNarvaezNessuna valutazione finora
- 7 - Sexual Self 1Documento17 pagine7 - Sexual Self 1marbie aliyahNessuna valutazione finora
- Why Provocative Clothing Shouldn't Effect Sexual HarrasmentDocumento2 pagineWhy Provocative Clothing Shouldn't Effect Sexual HarrasmentShanNessuna valutazione finora
- Information Pack Revised 14 Oct 2014Documento47 pagineInformation Pack Revised 14 Oct 2014api-246003035Nessuna valutazione finora
- Stalk Essay 2Documento8 pagineStalk Essay 2api-284104099Nessuna valutazione finora
- Running Head: Adaptive Traits Associated With PsychopathyDocumento44 pagineRunning Head: Adaptive Traits Associated With PsychopathyMira MNessuna valutazione finora
- The Roots of ViolenceDocumento28 pagineThe Roots of ViolenceEstrella CastilloNessuna valutazione finora
- Cyber StalkingDocumento21 pagineCyber StalkingParas BothraNessuna valutazione finora
- Independent Parliamentary Inquiry Into Stalking Law ReformDocumento42 pagineIndependent Parliamentary Inquiry Into Stalking Law ReformBren RyanNessuna valutazione finora
- Depersonalization in Response To Life-Threatening DangerDocumento10 pagineDepersonalization in Response To Life-Threatening DangeryochaiatariaNessuna valutazione finora
- Super Heros 123Documento4 pagineSuper Heros 123api-285136925Nessuna valutazione finora
- Strahlenfolter Stalking - TI - Thomas Rosenstengel - Satanismus Und Ritueller Missbrauch - ThomasrosenstengelDocumento39 pagineStrahlenfolter Stalking - TI - Thomas Rosenstengel - Satanismus Und Ritueller Missbrauch - ThomasrosenstengelWirklichkeit-kommtNessuna valutazione finora
- Youth Crime and JusticeDocumento16 pagineYouth Crime and JusticeAhtisham MirNessuna valutazione finora
- DR Heidi Stevenson Welker Dissertation ApprovedDocumento153 pagineDR Heidi Stevenson Welker Dissertation ApprovedvcautinNessuna valutazione finora
- Clearly Invisible ExcerptDocumento7 pagineClearly Invisible Excerptdrdawkins09Nessuna valutazione finora
- Strahlenfolter - Targeted Individuals of Organized Stalking and Electronic Harassments - 2012 ARCHIV - Hrvcanada-blogspot-DeDocumento28 pagineStrahlenfolter - Targeted Individuals of Organized Stalking and Electronic Harassments - 2012 ARCHIV - Hrvcanada-blogspot-DeTimo_KaehlkeNessuna valutazione finora
- Is Psychology A Science?Documento4 pagineIs Psychology A Science?Travis LiladharNessuna valutazione finora
- 3 2 08 Abuse Rampant in Juvenile Centers Across U SDocumento2 pagine3 2 08 Abuse Rampant in Juvenile Centers Across U SmocojaildocsNessuna valutazione finora
- WWW Thestalkingofsarahdegeyter Com 2020-11-16 Sarah Degeyter Attorney InteractioDocumento7 pagineWWW Thestalkingofsarahdegeyter Com 2020-11-16 Sarah Degeyter Attorney InteractioKeith LankfordNessuna valutazione finora
- Politicians Prostitutes Priests UpdateDocumento11 paginePoliticians Prostitutes Priests UpdateChristopher Alan HigniteNessuna valutazione finora
- Rebalancing The ScalesDocumento76 pagineRebalancing The ScalesdavidNessuna valutazione finora
- Boys and Men Healing Documentary/the Healing Years Documentary ReviewsDocumento2 pagineBoys and Men Healing Documentary/the Healing Years Documentary ReviewsbigvoicepicturesNessuna valutazione finora
- Strahlenfolter - TI - Rachael Orban - Organized Stalking - Am 09.08.2008 YoutubeDocumento37 pagineStrahlenfolter - TI - Rachael Orban - Organized Stalking - Am 09.08.2008 YoutubeTimo_KaehlkeNessuna valutazione finora
- Strahlenfolter - TI - How To Detect Electronic Harassment Easy - Targeted Individuals - YoutubeDocumento44 pagineStrahlenfolter - TI - How To Detect Electronic Harassment Easy - Targeted Individuals - YoutubeTimo_KaehlkeNessuna valutazione finora
- Voice RecognitionDocumento3 pagineVoice RecognitionSimon Benjamin100% (1)
- The Sex Offender and History of AbuseDocumento12 pagineThe Sex Offender and History of AbuseAaron Jenny Norgren100% (1)
- AkwashDocumento5 pagineAkwashdejanpecicNessuna valutazione finora
- Child Sexual Abuse What Does The Research Tell Us A Literature ReviewDocumento185 pagineChild Sexual Abuse What Does The Research Tell Us A Literature ReviewVanessa Kaye UrbanoNessuna valutazione finora
- How HipHop and Rap Affects YouthsDocumento4 pagineHow HipHop and Rap Affects YouthsSayyid Muhammad Aqeed AabidiNessuna valutazione finora
- Exploring The Lived Experience of Problematic Users of Internet Pornography (AOD)Documento29 pagineExploring The Lived Experience of Problematic Users of Internet Pornography (AOD)Francesca Palazzolo100% (1)
- Disability Benefits and Application File July 7, 2015 No Compression by HackersDocumento66 pagineDisability Benefits and Application File July 7, 2015 No Compression by HackersStan J. CaterboneNessuna valutazione finora
- Community Notification: John Howard Society of Alberta 1997Documento12 pagineCommunity Notification: John Howard Society of Alberta 1997HRCNessuna valutazione finora
- Team Name: Amir Syazwan B. IbrahimDocumento9 pagineTeam Name: Amir Syazwan B. IbrahimAnas SafwanNessuna valutazione finora
- Strahlenfolter Stalking - TI - Human Experimentation - Psychotronics Warfare - Part 4 - Synthetic Telepathy & Gang Stalking - GeeldonDocumento16 pagineStrahlenfolter Stalking - TI - Human Experimentation - Psychotronics Warfare - Part 4 - Synthetic Telepathy & Gang Stalking - GeeldonHermann-SchwanneckeNessuna valutazione finora
- Former Gang Stalking Private Security Spills On Program Silent HolocaustDocumento58 pagineFormer Gang Stalking Private Security Spills On Program Silent HolocaustlacyNessuna valutazione finora
- Victor Cline's Study PDFDocumento22 pagineVictor Cline's Study PDFsolay12Nessuna valutazione finora
- The Implications of Social MEDIA and TechnologyDocumento10 pagineThe Implications of Social MEDIA and Technologyhayee khanNessuna valutazione finora
- Victim Mentality PDFDocumento96 pagineVictim Mentality PDFfantasticuser1Nessuna valutazione finora
- Evaluation Mental Workload of Cognitive Tasks in Virtual Reality Using EOG Eye Tracker and EEG SignalsDocumento16 pagineEvaluation Mental Workload of Cognitive Tasks in Virtual Reality Using EOG Eye Tracker and EEG SignalsJ Andrés SalasNessuna valutazione finora
- 1998 - Coercion and Punishment in Long-Term Perspectives - McCordDocumento405 pagine1998 - Coercion and Punishment in Long-Term Perspectives - McCordnermal93Nessuna valutazione finora
- Torture Must Be CriminalisedDocumento1 paginaTorture Must Be CriminalisedWitsJusticeProjectNessuna valutazione finora
- Cyber Stalking Is A Cyber Crime or NotDocumento10 pagineCyber Stalking Is A Cyber Crime or NotdotrinufyaNessuna valutazione finora
- Press Release Surveillance AbuseDocumento4 paginePress Release Surveillance AbuseKeith LankfordNessuna valutazione finora
- Maruna and Mann 2006Documento23 pagineMaruna and Mann 2006stephanieNessuna valutazione finora
- Allen, Et Al. (2020) - Psychological Interventions For Sexual FantasiesDocumento8 pagineAllen, Et Al. (2020) - Psychological Interventions For Sexual FantasiesNancy MartinezNessuna valutazione finora
- Testimony - Peter A. ValbergDocumento41 pagineTestimony - Peter A. ValbergwgbhnewsNessuna valutazione finora
- Epidemiological SurveillanceDocumento22 pagineEpidemiological SurveillanceSyafiq HusniNessuna valutazione finora
- The NEATS: A Child & Family AssessmentDocumento46 pagineThe NEATS: A Child & Family AssessmentJane GilgunNessuna valutazione finora
- Peller V Shenker PC Stalking TSDocumento183 paginePeller V Shenker PC Stalking TSkarenNessuna valutazione finora
- PSYC350 Final NotesDocumento38 paginePSYC350 Final NotesAli KalyarNessuna valutazione finora
- April 2016 BUMC Proceedings - Blue Zones - Pag 220Documento148 pagineApril 2016 BUMC Proceedings - Blue Zones - Pag 220chown2k9Nessuna valutazione finora
- Trump's War On The U.S. Intelligence Community - The New RepublicDocumento10 pagineTrump's War On The U.S. Intelligence Community - The New RepublicjoseramirezeNessuna valutazione finora
- Gang Stalking - The Link Between Community Mobbing and Mass ShootingsDocumento6 pagineGang Stalking - The Link Between Community Mobbing and Mass ShootingsKarl-Hans-RohnNessuna valutazione finora
- Cognitive Behavioral Interventions For Sexually Abused Children Exhibiting PTSD SymptomatologyDocumento15 pagineCognitive Behavioral Interventions For Sexually Abused Children Exhibiting PTSD SymptomatologyalmaNessuna valutazione finora
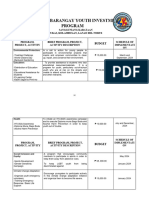
- Annual Barangay Youth Investment ProgramDocumento4 pagineAnnual Barangay Youth Investment ProgramBarangay MukasNessuna valutazione finora
- SAARC and Pakistan, Challenges, ProspectDocumento10 pagineSAARC and Pakistan, Challenges, ProspectRiaz kingNessuna valutazione finora
- Encyclopedia of Human Geography PDFDocumento2 pagineEncyclopedia of Human Geography PDFRosi Seventina100% (1)
- Remedies For Marriage PDFDocumento6 pagineRemedies For Marriage PDFAshutosh Rawat100% (1)
- Retrato Alvin YapanDocumento8 pagineRetrato Alvin YapanAngel Jan AgpalzaNessuna valutazione finora
- Plyler V Doe 1982Documento7 paginePlyler V Doe 1982api-412275167Nessuna valutazione finora
- Skill Developmet For Indian Textile Industry: S.K.SoniDocumento66 pagineSkill Developmet For Indian Textile Industry: S.K.Sonisandipsoni221811Nessuna valutazione finora
- Neste Annual Report 2019Documento213 pagineNeste Annual Report 2019Xianchi ZhangNessuna valutazione finora
- Profile - Sudip SahaDocumento2 pagineProfile - Sudip Sahasudipsinthee1Nessuna valutazione finora
- Type Certificate Data Sheet: No. EASA.R.100Documento9 pagineType Certificate Data Sheet: No. EASA.R.100SauliusNessuna valutazione finora
- South Valley: Transfer CertificateDocumento2 pagineSouth Valley: Transfer CertificateNitin PatidarNessuna valutazione finora
- Power Quality Improvement in Distribution Networks Containing DistributedDocumento6 paginePower Quality Improvement in Distribution Networks Containing DistributedsmruthiNessuna valutazione finora
- OneSumX IFRS9 ECL Impairments Produc SheetDocumento2 pagineOneSumX IFRS9 ECL Impairments Produc SheetRaju KaliperumalNessuna valutazione finora
- 235 at 2022Documento36 pagine235 at 2022Miguel FaganelloNessuna valutazione finora
- Gazette Issued Detailing Functions Under Namal's New MinistryDocumento5 pagineGazette Issued Detailing Functions Under Namal's New MinistryDarshana Sanjeewa0% (2)
- Layout Strategies: Iscussion UestionsDocumento18 pagineLayout Strategies: Iscussion Uestionshectorfa1Nessuna valutazione finora
- EGYPTIAN LITERA-WPS OfficeDocumento14 pagineEGYPTIAN LITERA-WPS OfficeLemoj CombiNessuna valutazione finora
- Letter of Appeal Pacheck Kay Tita ConnieDocumento2 pagineLetter of Appeal Pacheck Kay Tita ConnieNikko Avila IgdalinoNessuna valutazione finora
- 4 - ISO - 19650 - Guidance - Part - A - The - Information - Management - Function - and - Resources - Edition 3Documento16 pagine4 - ISO - 19650 - Guidance - Part - A - The - Information - Management - Function - and - Resources - Edition 3Rahul Tidke - ExcelizeNessuna valutazione finora
- Ky Yeu Hoi ThaoHVTC Quyen 1Documento1.348 pagineKy Yeu Hoi ThaoHVTC Quyen 1mmmanhtran2012Nessuna valutazione finora
- Meb Ydt 16Documento21 pagineMeb Ydt 16Guney BeyNessuna valutazione finora
- Ltma Lu DissertationDocumento5 pagineLtma Lu DissertationPayToWriteMyPaperUK100% (1)
- CentipedeDocumento2 pagineCentipedeMaeNessuna valutazione finora
- SMART Goal Worksheet (Action Plan)Documento2 pagineSMART Goal Worksheet (Action Plan)Tiaan de Jager100% (1)
- Bible Who Am I AdvancedDocumento3 pagineBible Who Am I AdvancedLeticia FerreiraNessuna valutazione finora
- Elvis CV Dec 2017Documento3 pagineElvis CV Dec 2017api-385945907Nessuna valutazione finora
- Business Forecasting: by ITH PhannyDocumento2 pagineBusiness Forecasting: by ITH PhannysmsNessuna valutazione finora
- Nittscher vs. NittscherDocumento4 pagineNittscher vs. NittscherKeej DalonosNessuna valutazione finora
- D0683SP Ans5Documento20 pagineD0683SP Ans5Tanmay SanchetiNessuna valutazione finora