Potrebbero piacerti anche
- Table 32-7Documento1 paginaTable 32-7Dragutin PetrićNessuna valutazione finora
- 2013 HIT Pocket Guide PDFDocumento4 pagine2013 HIT Pocket Guide PDFYoly SanchezNessuna valutazione finora
- Drug-Induced Conditions LectureDocumento48 pagineDrug-Induced Conditions Lectureapi-740273867Nessuna valutazione finora
- Heparin Induced Thrombocytopenia: By: Hadeel Abueid, Medical Student, Alquds University 3 March 2021Documento36 pagineHeparin Induced Thrombocytopenia: By: Hadeel Abueid, Medical Student, Alquds University 3 March 2021Hadeel Abu EidNessuna valutazione finora
- Heparin Induced ThrombocytopeniaDocumento17 pagineHeparin Induced ThrombocytopeniaTafsir arefin100% (1)
- Sec 9 HospitalDocumento36 pagineSec 9 HospitalAya Eid 7asanNessuna valutazione finora
- تقيم الجلطات الوريدية للكبارDocumento2 pagineتقيم الجلطات الوريدية للكبارAhmed Mohammed SalamaNessuna valutazione finora
- LovenoxDocumento1 paginaLovenoxKatie McPeek100% (2)
- 12av Acute Upper GI Bleeding EDDocumento2 pagine12av Acute Upper GI Bleeding EDA. RaufNessuna valutazione finora
- Practical Manual Scores Algorithms Haemostasis ThrombosisDocumento64 paginePractical Manual Scores Algorithms Haemostasis ThrombosisQuimico Inmunologia GeneticaNessuna valutazione finora
- ACLS ACS Algorithm NewDocumento3 pagineACLS ACS Algorithm Newsambo100% (1)
- PDF Nursing Care PlanDocumento16 paginePDF Nursing Care PlanMichael MabiniNessuna valutazione finora
- Lovenox (Enoxaparin)Documento1 paginaLovenox (Enoxaparin)E100% (1)
- Hypercoagulability and FibrinolyticDocumento42 pagineHypercoagulability and FibrinolyticdiansarlestaNessuna valutazione finora
- Enls V 3.0 Protocol Ais Final 0418Documento25 pagineEnls V 3.0 Protocol Ais Final 0418Caleb LinNessuna valutazione finora
- Suspected Stroke Algorithm: NINDS Time GoalsDocumento1 paginaSuspected Stroke Algorithm: NINDS Time Goalsjohndoe1995Nessuna valutazione finora
- Towards Developing A Scoring System For Febrile ThrombocytopeniaDocumento5 pagineTowards Developing A Scoring System For Febrile ThrombocytopeniaVimal NishadNessuna valutazione finora
- Acute Stroke Management by Carlos L Chua PDFDocumento61 pagineAcute Stroke Management by Carlos L Chua PDFHynne Jhea EchavezNessuna valutazione finora
- SASH IV Heparin GuidelineDocumento23 pagineSASH IV Heparin GuidelineMuhammad KhalilNessuna valutazione finora
- Deep Vein ThrombosisDocumento5 pagineDeep Vein Thrombosisampogison08Nessuna valutazione finora
- How To Approach A Patient With Bleeding?: ISTH Advanced Training Course, Portugal March 2014Documento100 pagineHow To Approach A Patient With Bleeding?: ISTH Advanced Training Course, Portugal March 2014ramanNessuna valutazione finora
- Bleeding DisordersDocumento62 pagineBleeding DisordersxtineNessuna valutazione finora
- Mahmood Care BlanDocumento5 pagineMahmood Care Blanmahmood asafraNessuna valutazione finora
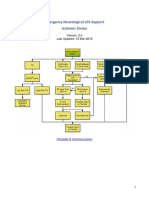
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Documento22 pagineEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNessuna valutazione finora
- Pharmacological Management of Acute Coronary Syndromes (ACS) and Acute Limb Ischemia (ALI)Documento44 paginePharmacological Management of Acute Coronary Syndromes (ACS) and Acute Limb Ischemia (ALI)hendratj90Nessuna valutazione finora
- ATTEST - Study - Supplementary DataDocumento8 pagineATTEST - Study - Supplementary Datasaurabh mahajanNessuna valutazione finora
- Venous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDDocumento23 pagineVenous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDعزالدين الطيارNessuna valutazione finora
- Heparin Induced Thrombocytopaeniaf PDFDocumento6 pagineHeparin Induced Thrombocytopaeniaf PDFOmyRojasNessuna valutazione finora
- Hypercoag States Algorithm 2014Documento10 pagineHypercoag States Algorithm 2014Sundar RamanathanNessuna valutazione finora
- Abdominal PDFDocumento1 paginaAbdominal PDFChakra BaktiNessuna valutazione finora
- Trombositopenia AfpDocumento5 pagineTrombositopenia AfpFadhila RamadhaniNessuna valutazione finora
- Revelation 1: 5,7Documento32 pagineRevelation 1: 5,7Christyl JoNessuna valutazione finora
- Lesson 8 THROMBOLYTICS FINALDocumento7 pagineLesson 8 THROMBOLYTICS FINALChristian PulmonesNessuna valutazione finora
- M33 - Stase IPD - Hassan Assagaf Guidance For The Treatment of Deep Vein Thrombosis and Pulmonary EmbolismDocumento16 pagineM33 - Stase IPD - Hassan Assagaf Guidance For The Treatment of Deep Vein Thrombosis and Pulmonary EmbolismHasan AssegafNessuna valutazione finora
- Laboratory Hemostatic DisordersDocumento41 pagineLaboratory Hemostatic DisordersYohanna SinuhajiNessuna valutazione finora
- Shahian2009 Halaman 12 DikonversiDocumento1 paginaShahian2009 Halaman 12 DikonversiKhairunisa SinulinggaNessuna valutazione finora
- Trombocitopenia PDFDocumento11 pagineTrombocitopenia PDFbrigde_xNessuna valutazione finora
- Primary Hemostasis Laboratory TestDocumento20 paginePrimary Hemostasis Laboratory Testtitania izaNessuna valutazione finora
- Arixtra Drug StudyDocumento2 pagineArixtra Drug StudyEdelweiss Marie Cayetano100% (1)
- NCM 219 Review Part 1 and 2Documento62 pagineNCM 219 Review Part 1 and 2jocieangelmendoza01Nessuna valutazione finora
- Lovenox (Enoxaparin) 80mgDocumento1 paginaLovenox (Enoxaparin) 80mgAdrianne BazoNessuna valutazione finora
- 5 Bleeding Disorders PPT EditedDocumento87 pagine5 Bleeding Disorders PPT EditedFrances Isabella OlasimanNessuna valutazione finora
- MBTroponinGuidelin PDFDocumento14 pagineMBTroponinGuidelin PDFBernadetta ViaNessuna valutazione finora
- Lovenox (Enoxaparin)Documento1 paginaLovenox (Enoxaparin)E100% (5)
- 109890management StrokeDocumento33 pagine109890management StrokeAndleeb GanaieNessuna valutazione finora
- NCM 109 SKILLS LAB DAY 1 Laboratory and Diagnostics22Documento55 pagineNCM 109 SKILLS LAB DAY 1 Laboratory and Diagnostics22Joseph DusichNessuna valutazione finora
- Drug Study - IBRANCEDocumento3 pagineDrug Study - IBRANCEKian HerreraNessuna valutazione finora
- Licensed Nurse CheckDocumento9 pagineLicensed Nurse CheckBianca MaeNessuna valutazione finora
- Hyperacute Stroke ManagementDocumento17 pagineHyperacute Stroke ManagementMahmoud Seif El NasrNessuna valutazione finora
- Antiplatelets Anticoagulant Drugs 1668083619Documento12 pagineAntiplatelets Anticoagulant Drugs 1668083619Nehal ElnagarNessuna valutazione finora
- HeparinDocumento2 pagineHeparinMagdayao Romamea100% (1)
- Questions For UNSW Mock Biomed VivaDocumento67 pagineQuestions For UNSW Mock Biomed VivaReuben TangNessuna valutazione finora
- Troponin PathwayDocumento1 paginaTroponin PathwayAllana AngelesNessuna valutazione finora
- Drug Study Heparin and FenylDocumento4 pagineDrug Study Heparin and FenylAnisa Jamito67% (3)
- Maternal Early Warning SistemDocumento2 pagineMaternal Early Warning SistemAnonymous PkOutzNessuna valutazione finora
- Anticoagulation TherapyDa EverandAnticoagulation TherapyJoe F. LauNessuna valutazione finora
- Acute Surgical Topics: An Infographic GuideDa EverandAcute Surgical Topics: An Infographic GuideNessuna valutazione finora
- Renin Angiotensin System and the HeartDa EverandRenin Angiotensin System and the HeartWalmor C. De MelloNessuna valutazione finora
- CHAPTER 2 (C) Innovation in EntrepreneurDocumento36 pagineCHAPTER 2 (C) Innovation in EntrepreneurHuiLingNessuna valutazione finora
- Solution Manual-Statistical Physics of Particles by Meheran KardarDocumento165 pagineSolution Manual-Statistical Physics of Particles by Meheran KardarDanielle Nguyen7% (14)
- Gita Ananda SDocumento10 pagineGita Ananda Srosaanggita76Nessuna valutazione finora
- FacebookDocumento2 pagineFacebookAbhijeet SingareNessuna valutazione finora
- Technology For Duck - Fish Integrated Farming System in GoaDocumento4 pagineTechnology For Duck - Fish Integrated Farming System in GoagavinilaaNessuna valutazione finora
- Pamphlet On Arrangement of Springs in Various Casnub Trolleys Fitted On Air Brake Wagon PDFDocumento9 paginePamphlet On Arrangement of Springs in Various Casnub Trolleys Fitted On Air Brake Wagon PDFNiKhil GuPtaNessuna valutazione finora
- Being Agile. Staying Resilient.: ANNUAL REPORT 2021-22Documento296 pagineBeing Agile. Staying Resilient.: ANNUAL REPORT 2021-22PrabhatNessuna valutazione finora
- GCGM PDFDocumento11 pagineGCGM PDFMiguel Angel Martin100% (1)
- Differentiating Language Difference and Language Disorder - Information For Teachers Working With English Language Learners in The Schools PDFDocumento23 pagineDifferentiating Language Difference and Language Disorder - Information For Teachers Working With English Language Learners in The Schools PDFIqra HassanNessuna valutazione finora
- Directorate of Technical Education, Maharashtra StateDocumento47 pagineDirectorate of Technical Education, Maharashtra StatePandurang GunjalNessuna valutazione finora
- Refrigerant Unit Lab ReportDocumento19 pagineRefrigerant Unit Lab Reportakmal100% (2)
- Lesson Plan Ordinal NumbersDocumento5 pagineLesson Plan Ordinal Numbersapi-329663096Nessuna valutazione finora
- 10 1 3 RMDDocumento5 pagine10 1 3 RMDRay GalfianNessuna valutazione finora
- Cover PageDocumento10 pagineCover PageAvijit GhoshNessuna valutazione finora
- Asian RegionalismDocumento15 pagineAsian RegionalismLiezel AalaNessuna valutazione finora
- Reforms of Parvez MusharifDocumento8 pagineReforms of Parvez MusharifTalha AslamNessuna valutazione finora
- How To Connect To iSCSI Targets On QNAP NAS Using MPIO On Windows 2008Documento30 pagineHow To Connect To iSCSI Targets On QNAP NAS Using MPIO On Windows 2008Jazz OberoiNessuna valutazione finora
- Veerasaiva Pantha in 12th Century MaharashtraDocumento2 pagineVeerasaiva Pantha in 12th Century MaharashtrarathkiraniNessuna valutazione finora
- ASC 2020-21 Questionnaire PDFDocumento11 pagineASC 2020-21 Questionnaire PDFShama PhotoNessuna valutazione finora
- FORM Module IpsDocumento10 pagineFORM Module IpsRizalNessuna valutazione finora
- Application Tracking System: Mentor - Yamini Ma'AmDocumento10 pagineApplication Tracking System: Mentor - Yamini Ma'AmBHuwanNessuna valutazione finora
- Beyond The Breech Trial. Maggie BanksDocumento4 pagineBeyond The Breech Trial. Maggie Bankspurpleanvil100% (2)
- Serie10 User Man ProgDocumento1.042 pagineSerie10 User Man Progfahmi derbel100% (1)
- Turning The Mind Into An AllyDocumento244 pagineTurning The Mind Into An AllyNic Sosa67% (3)
- 2009-04-CEN-TC121 N1574 Working Programme CEN TC 121Documento28 pagine2009-04-CEN-TC121 N1574 Working Programme CEN TC 121Manuel ValenteNessuna valutazione finora
- Motor BookDocumento252 pagineMotor BookKyaw KhNessuna valutazione finora
- SBU PlanningDocumento13 pagineSBU PlanningMohammad Raihanul HasanNessuna valutazione finora
- SWAMINATHAN Ajanta RhapsodyDocumento227 pagineSWAMINATHAN Ajanta RhapsodyRoberto E. García100% (1)
- Solutions For Tutorial Exercises Association Rule Mining.: Exercise 1. AprioriDocumento5 pagineSolutions For Tutorial Exercises Association Rule Mining.: Exercise 1. AprioriMarkib Singh AdawitahkNessuna valutazione finora
- Ddec VDocumento30 pagineDdec Vllama100% (1)