Potrebbero piacerti anche
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Head and Neck Cancer GuidelinesDocumento96 pagineHead and Neck Cancer GuidelinesTri KurniawanNessuna valutazione finora
- Dysphagia SurgicalDocumento75 pagineDysphagia Surgicalian ismail100% (1)
- What Does It Mean To Be Nil by Mouth?Documento2 pagineWhat Does It Mean To Be Nil by Mouth?Alexandra PlugarNessuna valutazione finora
- Esophageal Motility DisordersDocumento31 pagineEsophageal Motility DisordersAnonymous OlS0WZw100% (1)
- Esophageal CancerDocumento24 pagineEsophageal CancerSarah GatuzNessuna valutazione finora
- Dysphagia Presentation Auto Saved)Documento21 pagineDysphagia Presentation Auto Saved)Tiffani WallaceNessuna valutazione finora
- Dysphagia: DR Navin Shukla Associate Professor Department of E.N.T&H.N.SDocumento64 pagineDysphagia: DR Navin Shukla Associate Professor Department of E.N.T&H.N.SNavin ShuklaNessuna valutazione finora
- Preventing Aspiration Pneumonia by Addressing Three Key Risk Factors - Dysphagia, Poor Oral Hygiene, and Medication UseDocumento14 paginePreventing Aspiration Pneumonia by Addressing Three Key Risk Factors - Dysphagia, Poor Oral Hygiene, and Medication UseStacey WoodsNessuna valutazione finora
- TBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahDocumento84 pagineTBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahNadia RahimNessuna valutazione finora
- Intestinal ObstructionDocumento47 pagineIntestinal ObstructionAstrid Kurniawati AyuningtyasNessuna valutazione finora
- DysphagiaDocumento1 paginaDysphagiaShin EscaresesNessuna valutazione finora
- Laryngeal ObstructionDocumento2 pagineLaryngeal Obstructionajirah02Nessuna valutazione finora
- DYSPHAGIA Lecture NotesDocumento84 pagineDYSPHAGIA Lecture Notesmcmak357Nessuna valutazione finora
- Peri TonsilLar AbscessDocumento6 paginePeri TonsilLar Abscessrivan90Nessuna valutazione finora
- Upper Airway ObstructionDocumento31 pagineUpper Airway ObstructiontrimardiyanaisyanNessuna valutazione finora
- Lecture Contents: Definitions Composition of Hernia Managment of HerniaDocumento26 pagineLecture Contents: Definitions Composition of Hernia Managment of Herniaissam_1994Nessuna valutazione finora
- ICU One Pager Tracheostomy EmergenciesDocumento1 paginaICU One Pager Tracheostomy EmergenciesJonathan JohnsonNessuna valutazione finora
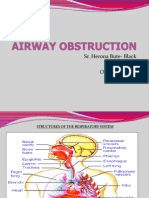
- Sr. Herona Bute- Black D.O.N.E October 7th 2011Documento35 pagineSr. Herona Bute- Black D.O.N.E October 7th 2011Jemicia AdamsNessuna valutazione finora
- OtosclerosisDocumento31 pagineOtosclerosisashry909100% (1)
- DysarthriaDocumento2 pagineDysarthriaBanjo VergaraNessuna valutazione finora
- Global AphasiaDocumento5 pagineGlobal AphasiaMuhammad Agus NurNessuna valutazione finora
- EncehaDocumento29 pagineEncehaToko RaMy Line100% (1)
- Crohns Disease Ebp Case Study PresentationDocumento23 pagineCrohns Disease Ebp Case Study Presentationapi-253093073Nessuna valutazione finora
- Chronic Rhinosinusitis With Nasal PolypsDocumento54 pagineChronic Rhinosinusitis With Nasal PolypsYosephine ninaNessuna valutazione finora
- Dysphagia Case StudyDocumento12 pagineDysphagia Case Studyapi-340845010Nessuna valutazione finora
- Benign Paroxysmal Positional Vertigo Pathophysiology, Causes, Canal Variants and Treatment PDFDocumento8 pagineBenign Paroxysmal Positional Vertigo Pathophysiology, Causes, Canal Variants and Treatment PDFegyzellahsNessuna valutazione finora
- Voice and Speech DisordersDocumento2 pagineVoice and Speech DisordersVishal Gaurav100% (1)
- Thyroglossal CystsDocumento4 pagineThyroglossal CystsCondurache Ilie-AndreiNessuna valutazione finora
- Dysphagia After Total LaryngectomyDocumento6 pagineDysphagia After Total LaryngectomyEduardo Lima de Melo Jr.Nessuna valutazione finora
- DSM-IV Schizophrenia Types and AssessmentDocumento32 pagineDSM-IV Schizophrenia Types and AssessmentJoyVee Pillagara-De LeonNessuna valutazione finora
- Presbycusis Causes and EffectsDocumento43 paginePresbycusis Causes and EffectsDesiana AyuNessuna valutazione finora
- Penetrating Abdominal TraumaDocumento67 paginePenetrating Abdominal TraumarizkaNessuna valutazione finora
- Diagnostic Assessment and Management of Dysphagia in Patients With Alzheimer's DiseaseDocumento9 pagineDiagnostic Assessment and Management of Dysphagia in Patients With Alzheimer's DiseaseLarissa MeloNessuna valutazione finora
- Inflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandInflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Chronic Otitis Media, Cholesteatoma, and Mastoiditis in AdultsDocumento14 pagineChronic Otitis Media, Cholesteatoma, and Mastoiditis in AdultschristineNessuna valutazione finora
- Notes, 1/e: Acute and Chronic Inflammation of LarynxDocumento23 pagineNotes, 1/e: Acute and Chronic Inflammation of LarynxvkNessuna valutazione finora
- OSA Diagnosis and TreatmentDocumento15 pagineOSA Diagnosis and TreatmentNaDrah YusOfNessuna valutazione finora
- 8 4 13notesDocumento437 pagine8 4 13notesJesse GriffithNessuna valutazione finora
- 7 Guidelines For The Care of Patients With Tracheostomy Tubes - Jan12 - 1 PDFDocumento100 pagine7 Guidelines For The Care of Patients With Tracheostomy Tubes - Jan12 - 1 PDFChing Tsz ShanNessuna valutazione finora
- Mood StabilizerDocumento2 pagineMood Stabilizernmyza89Nessuna valutazione finora
- RhinosinusitisDocumento45 pagineRhinosinusitisMuhammad Ade RahmanNessuna valutazione finora
- The Middle Ear TransformerDocumento13 pagineThe Middle Ear TransformerDiego RozulNessuna valutazione finora
- Peptic Ulcer DiseaseDocumento8 paginePeptic Ulcer Diseasepragna novaNessuna valutazione finora
- Esophageal Atresia and Tracheoesophageal FistulaDocumento21 pagineEsophageal Atresia and Tracheoesophageal FistulaIslam AmerNessuna valutazione finora
- DeliriumDocumento2 pagineDeliriumAngelique van Tonder100% (2)
- Psy MnemonicDocumento11 paginePsy MnemonicAmirul Hafiz100% (1)
- Effectiveness of Deep Pharyngeal Neuromuscular Stimulation Versus Thermal Gustatory Stimulation in Decreasing Length of Swallow Initiation and Improving Lingual Movements - Maria H WillisDocumento54 pagineEffectiveness of Deep Pharyngeal Neuromuscular Stimulation Versus Thermal Gustatory Stimulation in Decreasing Length of Swallow Initiation and Improving Lingual Movements - Maria H WillisconstantineeliaNessuna valutazione finora
- Pathophysiology of GERD and Its ComplicationDocumento25 paginePathophysiology of GERD and Its ComplicationalmiraNessuna valutazione finora
- Appendicitis: Causes, Symptoms, Diagnosis and TreatmentDocumento35 pagineAppendicitis: Causes, Symptoms, Diagnosis and TreatmentleighjagNessuna valutazione finora
- VFSS Swallowing Study for Dysphagia DiagnosisDocumento18 pagineVFSS Swallowing Study for Dysphagia Diagnosiskir4_yamat0Nessuna valutazione finora
- Dandy-Walker SyndromeDocumento12 pagineDandy-Walker SyndromeHarshita bansalNessuna valutazione finora
- Hiatal HerniaDocumento3 pagineHiatal HerniaJobelle AcenaNessuna valutazione finora
- Dysphagia: A Geriatric Giant?: Imedpub JournalsDocumento7 pagineDysphagia: A Geriatric Giant?: Imedpub JournalsErsya MuslihNessuna valutazione finora
- SB - Pediatrict Vocal NoduleDocumento7 pagineSB - Pediatrict Vocal NodulemediNessuna valutazione finora
- Meningitis-Malaria E PDFDocumento44 pagineMeningitis-Malaria E PDFSana ShafeeqNessuna valutazione finora
- Huntington's DiseaseDocumento15 pagineHuntington's DiseasePenny N R LestariNessuna valutazione finora
- Tumours of Larynx: A Clinicopathological StudyDa EverandTumours of Larynx: A Clinicopathological StudyNessuna valutazione finora
- Nasopharyngeal Carcinoma: From Etiology to Clinical PracticeDa EverandNasopharyngeal Carcinoma: From Etiology to Clinical PracticeAnne W.M. LeeNessuna valutazione finora
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- O&G History in Mandarin: Key Medical TermsDocumento1 paginaO&G History in Mandarin: Key Medical TermsHo Yong WaiNessuna valutazione finora
- Dengue CaseDocumento4 pagineDengue CaseHo Yong WaiNessuna valutazione finora
- Dengue CaseDocumento4 pagineDengue CaseHo Yong WaiNessuna valutazione finora
- Paediatrics at A GlanceDocumento2 paginePaediatrics at A GlanceHo Yong WaiNessuna valutazione finora
- Part 1Documento18 paginePart 1Ho Yong WaiNessuna valutazione finora
- Approach To The Patient With Dysphagia PDFDocumento7 pagineApproach To The Patient With Dysphagia PDFHo Yong Wai100% (1)
- Cerebellar SyndromeDocumento2 pagineCerebellar SyndromeHo Yong WaiNessuna valutazione finora
- Taking A Gynaecological HistoryDocumento21 pagineTaking A Gynaecological Historyasif_siddiqui_2100% (1)
- Dengue CaseDocumento4 pagineDengue CaseHo Yong WaiNessuna valutazione finora
- Department Coordinator BioDocumento1 paginaDepartment Coordinator BioHo Yong WaiNessuna valutazione finora
- Bipolar DisorderDocumento1 paginaBipolar DisorderHo Yong WaiNessuna valutazione finora
- HivDocumento1 paginaHivHo Yong WaiNessuna valutazione finora
- HomeworkDocumento12 pagineHomeworkHo Yong WaiNessuna valutazione finora
- CPG Management of Dengue Infection in Adults (Revised 2nd Edition)Documento68 pagineCPG Management of Dengue Infection in Adults (Revised 2nd Edition)umiraihana1Nessuna valutazione finora
- Ob-Gyn Clinical Cases (From Apgo Site)Documento221 pagineOb-Gyn Clinical Cases (From Apgo Site)jamieNessuna valutazione finora
- Lesson 5 ReviewDocumento4 pagineLesson 5 ReviewHo Yong WaiNessuna valutazione finora
- BVMDocumento3 pagineBVMHo Yong WaiNessuna valutazione finora
- Common ENT ComplaintsDocumento9 pagineCommon ENT ComplaintsHo Yong WaiNessuna valutazione finora
- Lesson 8 ReviewDocumento3 pagineLesson 8 ReviewHo Yong WaiNessuna valutazione finora
- Test Yourself AnaesthesiologyDocumento4 pagineTest Yourself AnaesthesiologyHo Yong WaiNessuna valutazione finora
- Anaesthesiology Student Reflects on Patient SafetyDocumento2 pagineAnaesthesiology Student Reflects on Patient SafetyHo Yong WaiNessuna valutazione finora
- Common Long Cases IM Sem 7Documento3 pagineCommon Long Cases IM Sem 7Ho Yong WaiNessuna valutazione finora
- Clinical Skills Guide for Medical ProceduresDocumento1 paginaClinical Skills Guide for Medical ProceduresHo Yong WaiNessuna valutazione finora
- Lesson 9 ReviewDocumento2 pagineLesson 9 ReviewHo Yong WaiNessuna valutazione finora
- Lesson 6 ReviewDocumento2 pagineLesson 6 ReviewHo Yong WaiNessuna valutazione finora
- TBL RheumatologyDocumento16 pagineTBL RheumatologyHo Yong WaiNessuna valutazione finora
- Lesson 3 ReviewDocumento4 pagineLesson 3 ReviewHo Yong WaiNessuna valutazione finora
- TBL PaedsDocumento10 pagineTBL PaedsHo Yong WaiNessuna valutazione finora
- Psy Case DiscussionDocumento16 paginePsy Case DiscussionHo Yong WaiNessuna valutazione finora
- Nursing Cardiovascular AssessmentDocumento2 pagineNursing Cardiovascular Assessmentgladz25100% (2)
- 3ixso2idq334tonwmfhk0rrcDocumento2 pagine3ixso2idq334tonwmfhk0rrcrishikeshraj2021Nessuna valutazione finora
- Hem OccultDocumento2 pagineHem OccultfidofidzNessuna valutazione finora
- 2020 AGEAGEING Deprescribing in Older People Approaching en of Life Development and Validation of STOPPFrail Version 2Documento7 pagine2020 AGEAGEING Deprescribing in Older People Approaching en of Life Development and Validation of STOPPFrail Version 2erika avelina rodriguez jaureguiNessuna valutazione finora
- P ArtographDocumento17 pagineP ArtographPrincess RoseNessuna valutazione finora
- AV CPG 2016 Ed 1.1Documento377 pagineAV CPG 2016 Ed 1.1Fatality FatalityNessuna valutazione finora
- 003 Clinical Appraisal-1Documento3 pagine003 Clinical Appraisal-1Erryl Justine AdvinculaNessuna valutazione finora
- The Health Effects of Stimulant DrinksDocumento9 pagineThe Health Effects of Stimulant DrinksGeovanny RochinaNessuna valutazione finora
- Autosomal Dominant DiseasesDocumento3 pagineAutosomal Dominant DiseasesAliHassanNessuna valutazione finora
- 2020 - Pemphigus Vulgaris and Bullous Pemphigoid Update On Diagnosis and TreatmentDocumento12 pagine2020 - Pemphigus Vulgaris and Bullous Pemphigoid Update On Diagnosis and TreatmentnancyerlenNessuna valutazione finora
- Textbook of Medical Parasitology Protozoology HelmDocumento2 pagineTextbook of Medical Parasitology Protozoology HelmAnge OuedraogoNessuna valutazione finora
- As Level Biology AQA Immune ResponseDocumento11 pagineAs Level Biology AQA Immune ResponseSahib Matharu100% (1)
- JURNAL NYERI GASTRITIS TERAPI MUSIK-dikonversiDocumento11 pagineJURNAL NYERI GASTRITIS TERAPI MUSIK-dikonversiemmazainNessuna valutazione finora
- Left-Sided Congestive Heart Failure Case PresentationDocumento64 pagineLeft-Sided Congestive Heart Failure Case PresentationNicole Villanueva, BSN - Level 3ANessuna valutazione finora
- Argumentative Essay FinalDocumento10 pagineArgumentative Essay Finalapi-550035247Nessuna valutazione finora
- EFM Teaching Didactic FINALDocumento81 pagineEFM Teaching Didactic FINALNadia RestyNessuna valutazione finora
- Defining Autism (Martha Herbert, M.D.)Documento52 pagineDefining Autism (Martha Herbert, M.D.)National Press FoundationNessuna valutazione finora
- AppareilComercial EITDocumento128 pagineAppareilComercial EITCarine OrnelasNessuna valutazione finora
- FWCQ22 COVID19 Healthcare Protocol V28 EnglishDocumento24 pagineFWCQ22 COVID19 Healthcare Protocol V28 EnglishKarthik KothandaramanNessuna valutazione finora
- CRP Latex TestDocumento9 pagineCRP Latex TestCitra DewiNessuna valutazione finora
- Oral Squamous Cell Carcinoma (OSCC)Documento37 pagineOral Squamous Cell Carcinoma (OSCC)Yusra Shaukat100% (1)
- Hirschsprung DiseaseDocumento96 pagineHirschsprung DiseaseHariette Delmo de Leon100% (1)
- Schizophrenia Coursework - Jack Kerouac PresentationDocumento16 pagineSchizophrenia Coursework - Jack Kerouac PresentationCMNessuna valutazione finora
- Appendix I: PROFORMADocumento6 pagineAppendix I: PROFORMAVishwas NayakNessuna valutazione finora
- Renting Homes and Visiting Doctors in EnglandDocumento5 pagineRenting Homes and Visiting Doctors in EnglandDheaaNessuna valutazione finora
- Acupuncture For Refractory Cases of Sudden Hearing LossDocumento7 pagineAcupuncture For Refractory Cases of Sudden Hearing LossBayu AgustinusNessuna valutazione finora
- Uterine AtonyDocumento1 paginaUterine AtonyYakumaNessuna valutazione finora
- Asthma Patient ProfileDocumento8 pagineAsthma Patient ProfileGlenn Asuncion PagaduanNessuna valutazione finora
- Radiology 101Documento2 pagineRadiology 101Nadhirah AnandaNessuna valutazione finora
- Treatment of Age-Related Macular Degeneration: Risk FactorsDocumento4 pagineTreatment of Age-Related Macular Degeneration: Risk FactorsisraelrtNessuna valutazione finora