Potrebbero piacerti anche
- Management of Hypertension in CKDDocumento40 pagineManagement of Hypertension in CKDPratik TripathiNessuna valutazione finora
- Guidline Hipertensi Dengan DiabetesDocumento5 pagineGuidline Hipertensi Dengan DiabetesTri HandayaniNessuna valutazione finora
- Hosp Ops II Week 2 Questions 1Documento3 pagineHosp Ops II Week 2 Questions 1api-650133203Nessuna valutazione finora
- Adime PT 2Documento8 pagineAdime PT 2api-357368000Nessuna valutazione finora
- Slide Speaker Candesartan For Hypertension in CKD PatientsDocumento43 pagineSlide Speaker Candesartan For Hypertension in CKD Patientsesdras pramuditaNessuna valutazione finora
- HPN in CKDDocumento27 pagineHPN in CKDLeigh Picardal Caragos-MerinNessuna valutazione finora
- Rawabi Saleh Bakrman Fatima Mohammed Dawood Supervision: Dr. Hassan BayashootDocumento21 pagineRawabi Saleh Bakrman Fatima Mohammed Dawood Supervision: Dr. Hassan BayashootRawabi SalehNessuna valutazione finora
- Chapter 3 Management of Progression and Compl 2013 Kidney International SupDocumento18 pagineChapter 3 Management of Progression and Compl 2013 Kidney International SupwardaninurindahNessuna valutazione finora
- Cumbria and Lancs KCN Algorithm PDFDocumento18 pagineCumbria and Lancs KCN Algorithm PDFratih83Nessuna valutazione finora
- Chronic Kidney DiseaseDocumento3 pagineChronic Kidney Diseaseapi-668470097Nessuna valutazione finora
- Drug Induced Kel 5Documento32 pagineDrug Induced Kel 5Nusaibah RomadhoniNessuna valutazione finora
- Epo DrugstudyDocumento3 pagineEpo DrugstudyKhatlen BagaresNessuna valutazione finora
- Atorvastatin Drugs StudyDocumento3 pagineAtorvastatin Drugs StudyRodolfo CampoNessuna valutazione finora
- Woodell2018 (Jurnal Asli)Documento13 pagineWoodell2018 (Jurnal Asli)Fatah Jati PNessuna valutazione finora
- Penunjang Pemeriksaan KlinisDocumento88 paginePenunjang Pemeriksaan Klinisgrady_christian_9720Nessuna valutazione finora
- KDIGO 2022 Diabetes Guideline Quick Reference GuideDocumento2 pagineKDIGO 2022 Diabetes Guideline Quick Reference GuideChristian Risco QuezadaNessuna valutazione finora
- CHRONIC KIDNEY DISEASE Pelatihan Perawat HD 2021Documento33 pagineCHRONIC KIDNEY DISEASE Pelatihan Perawat HD 2021Yudha WirawanNessuna valutazione finora
- CKD CmeDocumento45 pagineCKD Cmeizatul farhanahNessuna valutazione finora
- Upper Gi BleedDocumento5 pagineUpper Gi Bleedanita13Nessuna valutazione finora
- AMLODIPINEDocumento3 pagineAMLODIPINESL Hanna NebridaNessuna valutazione finora
- 2019 Article EssentialPointsFromEvidence-baDocumento15 pagine2019 Article EssentialPointsFromEvidence-baNur RahmahNessuna valutazione finora
- Diabetic Kidney Disease (DKD)Documento39 pagineDiabetic Kidney Disease (DKD)monpyitharNessuna valutazione finora
- Effect of Low-Dose Perindopril/Indapamide On Albuminuria in DiabetesDocumento9 pagineEffect of Low-Dose Perindopril/Indapamide On Albuminuria in Diabetesguugle gogleNessuna valutazione finora
- CKD Kdigo 2012Documento27 pagineCKD Kdigo 2012giggs_libraNessuna valutazione finora
- Important Complications of Chronic Kidney Disease PDFDocumento4 pagineImportant Complications of Chronic Kidney Disease PDFDrBishnu Prasad MahalaNessuna valutazione finora
- KEM Protocols - Hypertensive Emergency (Dr. Pritha)Documento3 pagineKEM Protocols - Hypertensive Emergency (Dr. Pritha)Sonu AntonyNessuna valutazione finora
- Chronic Kidney Disease Malaysian CPG 2011Documento22 pagineChronic Kidney Disease Malaysian CPG 2011aideeh31100% (1)
- Diagnose CKD:: ACE inhibitor/ARB UseDocumento2 pagineDiagnose CKD:: ACE inhibitor/ARB UseAman AmanNessuna valutazione finora
- Enfrentamiento Práctico en Asctis de Reciente Comienzo Asociada A Cirrosis.Documento15 pagineEnfrentamiento Práctico en Asctis de Reciente Comienzo Asociada A Cirrosis.Maria Jose Gothe GandolfiNessuna valutazione finora
- Treating Hypertension in Patients With Medical CondtionsDocumento6 pagineTreating Hypertension in Patients With Medical CondtionsSebastian ApeleoNessuna valutazione finora
- DefisniDocumento41 pagineDefisniAzizah MNessuna valutazione finora
- PerindoprilDocumento5 paginePerindoprilEsther Afrianti SagalaNessuna valutazione finora
- Atrial Fibrillation TDDocumento6 pagineAtrial Fibrillation TDapi-594366475Nessuna valutazione finora
- CaptoprilDocumento3 pagineCaptoprilNovi YulianaNessuna valutazione finora
- Type 2 Diabetes Chronic Kidney Disease: Use of Dipeptidyl Peptidase-4 Inhibitors in Patients WithDocumento8 pagineType 2 Diabetes Chronic Kidney Disease: Use of Dipeptidyl Peptidase-4 Inhibitors in Patients WithRahmanu ReztaputraNessuna valutazione finora
- Section 2artfibDocumento2 pagineSection 2artfibIain Tarrant-MurphyNessuna valutazione finora
- HF 2 - PDFDocumento5 pagineHF 2 - PDFAndrea Díaz ValenciaNessuna valutazione finora
- Chronic Kidney Disease: For The Primary Care PhysicianDocumento54 pagineChronic Kidney Disease: For The Primary Care PhysicianFlavia PolodeanuNessuna valutazione finora
- In Primary Care: Chronic Kidney Disease (CKD)Documento4 pagineIn Primary Care: Chronic Kidney Disease (CKD)NotForAbuseNessuna valutazione finora
- 312-Rle-Drug StudyDocumento4 pagine312-Rle-Drug StudyRogelyn PatriarcaNessuna valutazione finora
- Atorvastatin Calcium Drug Study WWW RNpedia ComDocumento3 pagineAtorvastatin Calcium Drug Study WWW RNpedia ComEloisa BretañaNessuna valutazione finora
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocumento2 pagineName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesKarl Lourenz DeysolongNessuna valutazione finora
- AspirinDocumento2 pagineAspirinKarl Lourenz DeysolongNessuna valutazione finora
- CarvedilolDocumento2 pagineCarvedilolKarl Lourenz DeysolongNessuna valutazione finora
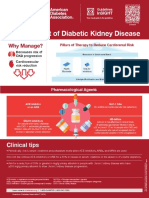
- Management of Diabetic Kidney Disease Updated 0Documento1 paginaManagement of Diabetic Kidney Disease Updated 0Jia-PeiWuNessuna valutazione finora
- Clinical Paperwork 20 2Documento3 pagineClinical Paperwork 20 2api-603548679Nessuna valutazione finora
- Aki and CKD Therapy 2021Documento46 pagineAki and CKD Therapy 2021Alfathri YunediNessuna valutazione finora
- 2017 AHA Hypertension Guideline SummaryDocumento16 pagine2017 AHA Hypertension Guideline Summaryyassin mostafaNessuna valutazione finora
- Compendio HighDocumento189 pagineCompendio HighCristi RojasNessuna valutazione finora
- Adime 2 UchcDocumento9 pagineAdime 2 Uchcapi-307029735Nessuna valutazione finora
- Chronic Kidney Disease: Know The Risks of Medications and Imaging StudiesDocumento2 pagineChronic Kidney Disease: Know The Risks of Medications and Imaging StudiesrchristevenNessuna valutazione finora
- Hipertensi KebidananDocumento77 pagineHipertensi KebidananNINING ALKOMAHNessuna valutazione finora
- Ebm - Role of Acei - Arb in Reducing Proteinuria - Progression of DM NephropathyDocumento25 pagineEbm - Role of Acei - Arb in Reducing Proteinuria - Progression of DM NephropathyHannah HalimNessuna valutazione finora
- Pharmaceutical Care in Renal DiseaseDocumento15 paginePharmaceutical Care in Renal DiseaseEfraim MangalukNessuna valutazione finora
- Albumin:Creatinine Ratio (Urine) - ACR: Description Indication Why Measure ACR?Documento2 pagineAlbumin:Creatinine Ratio (Urine) - ACR: Description Indication Why Measure ACR?Ebtisam alfakhriNessuna valutazione finora
- BENEDICT: Primary Prevention of Microalbuminuria in Hypertensive Type 2 DiabetesDocumento4 pagineBENEDICT: Primary Prevention of Microalbuminuria in Hypertensive Type 2 DiabetesWami FadelNessuna valutazione finora
- Hypertension For StudentsDocumento64 pagineHypertension For StudentsNajib Al FatinNessuna valutazione finora
- BenazeprilDocumento2 pagineBenazeprilFeliciaDorghamNessuna valutazione finora
- Hypertension Guidelines PDFDocumento10 pagineHypertension Guidelines PDFARAVINDANessuna valutazione finora
- Anemia in Chronic Kidney DiseaseDocumento38 pagineAnemia in Chronic Kidney DiseaseHemodialisa LindimaraNessuna valutazione finora
- Management of Renal Stones: Theme From January 2013 ExamDocumento123 pagineManagement of Renal Stones: Theme From January 2013 ExamBela VitoriaNessuna valutazione finora
- Cell Division LabDocumento5 pagineCell Division Labjenna727Nessuna valutazione finora
- Lung CancerDocumento17 pagineLung CancerLana AdilaNessuna valutazione finora
- The TYWLS Times - October 2018 EditionDocumento4 pagineThe TYWLS Times - October 2018 EditionThe TYWLS TimesNessuna valutazione finora
- sc1994 00 Dfu SLVDocumento211 paginesc1994 00 Dfu SLVMarta ValašekNessuna valutazione finora
- 3M Material Safety Data Sheet Electrical Moisture Sealant Pads (Ems Ii)Documento7 pagine3M Material Safety Data Sheet Electrical Moisture Sealant Pads (Ems Ii)danielliram993Nessuna valutazione finora
- Haematology Practice MCQsDocumento3 pagineHaematology Practice MCQsmonday125100% (1)
- Stages of Human DevelopmentDocumento20 pagineStages of Human DevelopmentTinisStrongNessuna valutazione finora
- Health Assessment Handout MayannDocumento9 pagineHealth Assessment Handout MayannDENNIS N. MUÑOZNessuna valutazione finora
- Finished Research PaperDocumento12 pagineFinished Research Paperapi-242056195Nessuna valutazione finora
- 237 Goljan Rapid Review Images FlashcardsDocumento34 pagine237 Goljan Rapid Review Images FlashcardsAhsan Tanvir100% (1)
- Chaper 3: Probability and Probability Models: (Introductory Biostatistics - Chap T. Le)Documento7 pagineChaper 3: Probability and Probability Models: (Introductory Biostatistics - Chap T. Le)Hà Anh Minh LêNessuna valutazione finora
- Trevor Nong Final ProjectDocumento7 pagineTrevor Nong Final Projectapi-375199340Nessuna valutazione finora
- Hifema: Dr. Bobi Ahmad Sahid, S.KepDocumento21 pagineHifema: Dr. Bobi Ahmad Sahid, S.Kepdr.Bobi Ahmad Sahid, S.KepNessuna valutazione finora
- Atod Practice QuizDocumento1 paginaAtod Practice Quizapi-263456844100% (1)
- DIARRHEADocumento2 pagineDIARRHEAJoni P TNessuna valutazione finora
- Guide: DR Srinath Rao Presenter:Dr SR Soumya (Materia Medica MD Part-1) 15/12/14Documento50 pagineGuide: DR Srinath Rao Presenter:Dr SR Soumya (Materia Medica MD Part-1) 15/12/14Krishna Veni100% (2)
- Bio Care Sanitary PadDocumento8 pagineBio Care Sanitary PadWie Pin Siddhi100% (1)
- Project NewDocumento33 pagineProject Newceeyem83% (12)
- Postsurgical Anatomy: Lung Transplantation Lobectomy and PneumonectomyDocumento36 paginePostsurgical Anatomy: Lung Transplantation Lobectomy and PneumonectomyYui Phitchaya MonsintornNessuna valutazione finora
- 2nd Announcement 18th ASNO Bali 2023Documento21 pagine2nd Announcement 18th ASNO Bali 2023Dayu Triana RahmawatiNessuna valutazione finora
- UrethritisDocumento11 pagineUrethritismarej143Nessuna valutazione finora
- Special TopicsDocumento8 pagineSpecial Topicskatherine ruizNessuna valutazione finora
- Gastrointestinal BleedingDocumento31 pagineGastrointestinal BleedingDenice IsidroNessuna valutazione finora
- Quizlet (4) MMMMMMDocumento30 pagineQuizlet (4) MMMMMMnaimNessuna valutazione finora
- IndependentDocumento20 pagineIndependentindy-bcNessuna valutazione finora
- PMDC Community Medicine Mcqs PDFDocumento280 paginePMDC Community Medicine Mcqs PDFJay KNessuna valutazione finora
- ThrombophiliasDocumento9 pagineThrombophiliasSeraj Abed ElmoatiNessuna valutazione finora
- Ficat and Arlet Staging of Avascular Necrosis of Femoral HeadDocumento6 pagineFicat and Arlet Staging of Avascular Necrosis of Femoral HeadFernando Sugiarto0% (1)