Potrebbero piacerti anche
- Ginni Rani NewDocumento41 pagineGinni Rani NewEkta RajputNessuna valutazione finora
- Gestational DMDocumento32 pagineGestational DMKatNessuna valutazione finora
- GESTASIONAL DIABETES MELLITUS SimposiumDocumento18 pagineGESTASIONAL DIABETES MELLITUS SimposiumHabiby Habibaty QolbiNessuna valutazione finora
- Gestational DiabetesDocumento12 pagineGestational DiabetessilentluciditysfNessuna valutazione finora
- Seminar 5 - DM in PregnancyDocumento19 pagineSeminar 5 - DM in PregnancyHakimah K. SuhaimiNessuna valutazione finora
- 11.pregnancy & Diabetes MellitusDocumento23 pagine11.pregnancy & Diabetes Mellituskume senbetaNessuna valutazione finora
- Diabetes in PregnancyDocumento38 pagineDiabetes in Pregnancybdzq3i12Nessuna valutazione finora
- Gestational Diabetes: Update in Diagnosis and ManagementDocumento61 pagineGestational Diabetes: Update in Diagnosis and ManagementTriani Ismelia FirdayantiNessuna valutazione finora
- Presentation On: Kgmu College of NursingDocumento42 paginePresentation On: Kgmu College of NursingSweety YadavNessuna valutazione finora
- Diabetes Mellitus: Medical Complications in PregnancyDocumento19 pagineDiabetes Mellitus: Medical Complications in PregnancySenopati KhanjieNessuna valutazione finora
- Gestational Diabetes Mellitus (GDM)Documento24 pagineGestational Diabetes Mellitus (GDM)asyrafali93Nessuna valutazione finora
- Gestational Diabetes MellitusDocumento21 pagineGestational Diabetes MellitusGlen Jacobs SumadihardjaNessuna valutazione finora
- Management of Gestational Diabetes and Type-2 Diabetes in PR PDFDocumento75 pagineManagement of Gestational Diabetes and Type-2 Diabetes in PR PDFYohannis AsefaNessuna valutazione finora
- Gestational Diabetes Mellitus: Capt Narendra Sarlam MH GwaliorDocumento41 pagineGestational Diabetes Mellitus: Capt Narendra Sarlam MH Gwalioryash shrivastavaNessuna valutazione finora
- Gestational DiabetesDocumento51 pagineGestational Diabeteskhadzx100% (2)
- Gestational Diabetes MellitusDocumento14 pagineGestational Diabetes MellitusCzarina PorciunculaNessuna valutazione finora
- Materi Diabetes Mellitus - WAHYUDocumento29 pagineMateri Diabetes Mellitus - WAHYUAli Sibra MulluziNessuna valutazione finora
- DR Farah Deeba Nasrullah Asst Prof Dept of Obgyn Unit Ii Chk/DuhsDocumento14 pagineDR Farah Deeba Nasrullah Asst Prof Dept of Obgyn Unit Ii Chk/DuhsUloko ChristopherNessuna valutazione finora
- Diabetes in Pregnancy: An Overview of Gestational DiabetesDocumento16 pagineDiabetes in Pregnancy: An Overview of Gestational DiabetesAlo MarianoNessuna valutazione finora
- DM PresentationDocumento74 pagineDM PresentationtivaNessuna valutazione finora
- Diabetes in Pregnancy: DR Omar Abu-AzzamDocumento36 pagineDiabetes in Pregnancy: DR Omar Abu-AzzamRoba Mohmed AlamroNessuna valutazione finora
- DiabetesDocumento38 pagineDiabetesHema MaliniNessuna valutazione finora
- Gestational DiabetesDocumento52 pagineGestational Diabetestammycristobalmd100% (8)
- Diabetes Mellitus & Pregnancy: G.M PunarbawaDocumento27 pagineDiabetes Mellitus & Pregnancy: G.M PunarbawaMartina RizkiNessuna valutazione finora
- Gestational Diabetes MellitusDocumento22 pagineGestational Diabetes MellitusNadia AgagonNessuna valutazione finora
- Updated For Diabetes Mellitus: Krairat Komdee, MD. Department of Internal Medicine Phayao HospitalDocumento47 pagineUpdated For Diabetes Mellitus: Krairat Komdee, MD. Department of Internal Medicine Phayao HospitalKrairat KomdeeNessuna valutazione finora
- Nutrition in DMDocumento33 pagineNutrition in DMkero R.habibNessuna valutazione finora
- Diabetes MellitusDocumento38 pagineDiabetes MellitustantsaNessuna valutazione finora
- Management Of: Diabetes in PregnancyDocumento8 pagineManagement Of: Diabetes in PregnancyNazmun NaharNessuna valutazione finora
- Gestational DiabetiesDocumento50 pagineGestational DiabetiesAkshat Goel100% (1)
- Diabetes MellitusDocumento40 pagineDiabetes MellitusDetria Rahma GastiNessuna valutazione finora
- DIPSI GuidelinesDocumento7 pagineDIPSI GuidelinesvinaypharmNessuna valutazione finora
- Gestational Diabetes MellitusDocumento43 pagineGestational Diabetes MellitusDeepa Saravan100% (1)
- Diabetes in Pregnancy: Early Diagnosis and Comphrehensive ManagementDocumento32 pagineDiabetes in Pregnancy: Early Diagnosis and Comphrehensive ManagementayuNessuna valutazione finora
- Guideline PERKENI 2015Documento34 pagineGuideline PERKENI 2015Iin Citra Liana HasibuanNessuna valutazione finora
- Gestational Diabetes Mellitus (GDM) .TriceDocumento47 pagineGestational Diabetes Mellitus (GDM) .TricejerrydanfordfxNessuna valutazione finora
- Diabetes Mellitus & Pregnancy by D.a.mehtaDocumento31 pagineDiabetes Mellitus & Pregnancy by D.a.mehtadr.d.a.mehta11Nessuna valutazione finora
- PCC HandbookDocumento193 paginePCC HandbookMusa LandeNessuna valutazione finora
- Recent Advances in Management of Gestational Diabetes and Pre-EclampsiaDocumento36 pagineRecent Advances in Management of Gestational Diabetes and Pre-EclampsiaSyed Zahed AliNessuna valutazione finora
- Diabetes in PregnancyDocumento62 pagineDiabetes in Pregnancykapil khanalNessuna valutazione finora
- Nutricare in Diabetes With Special ConditionsDocumento40 pagineNutricare in Diabetes With Special ConditionsNudrat KhanNessuna valutazione finora
- Prediabetes 1Documento21 paginePrediabetes 1Nirmaa100% (2)
- Management of Diabetes in PregnancyDocumento37 pagineManagement of Diabetes in PregnancySusanaNessuna valutazione finora
- Guyana Diabetes Guidelines 26-Jun-23 FinalDocumento20 pagineGuyana Diabetes Guidelines 26-Jun-23 FinalnathanielNessuna valutazione finora
- Gestational Diabetes MellitusDocumento42 pagineGestational Diabetes MellitusMohammed AbdNessuna valutazione finora
- 15 - Diabetes in PregnancyDocumento28 pagine15 - Diabetes in PregnancyMohammad Izwan ShahNessuna valutazione finora
- Diabetes and PregnancyDocumento63 pagineDiabetes and PregnancyAyesha KhatunNessuna valutazione finora
- Diabetes Mellitus in PregnancyDocumento55 pagineDiabetes Mellitus in Pregnancyapi-3856051100% (2)
- Diabetes Mellitus Management of Gestational Diabetes - 280720Documento12 pagineDiabetes Mellitus Management of Gestational Diabetes - 280720AddisNessuna valutazione finora
- Management of Diabetes in PregnancyDocumento37 pagineManagement of Diabetes in PregnancyveronicaNessuna valutazione finora
- Gestational Diabetes Mellitus (GDM)Documento11 pagineGestational Diabetes Mellitus (GDM)Sadia YousafNessuna valutazione finora
- Diabetes PregnancyDocumento65 pagineDiabetes PregnancyJohn Christopher LucesNessuna valutazione finora
- Gestational Diabetes 1Documento12 pagineGestational Diabetes 1Kyla Isobel DalonosNessuna valutazione finora
- Gestational Diabetes Update 2Documento42 pagineGestational Diabetes Update 2Aeni AiniNessuna valutazione finora
- 21.diabetes Mellitus in PregnancyDocumento47 pagine21.diabetes Mellitus in Pregnancydeneke100% (1)
- GDM (Gestational Diabetes Mellitus) PresentationDocumento32 pagineGDM (Gestational Diabetes Mellitus) PresentationMovies 4 YouNessuna valutazione finora
- Ketogenic Diet "Yes & No" Guide For BeginnersDa EverandKetogenic Diet "Yes & No" Guide For BeginnersValutazione: 3 su 5 stelle3/5 (1)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDa EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesValutazione: 4 su 5 stelle4/5 (2)
- Bacaan Setelah Shalat Fardhu PDFDocumento4 pagineBacaan Setelah Shalat Fardhu PDFMuhammad mukramNessuna valutazione finora
- Early Detection of Psychosomatic - UNTAD - 2012Documento12 pagineEarly Detection of Psychosomatic - UNTAD - 2012Muhammad mukramNessuna valutazione finora
- Coping Mechanism in Psychosomatic - UNTAD - 2012Documento12 pagineCoping Mechanism in Psychosomatic - UNTAD - 2012Muhammad mukramNessuna valutazione finora
- Miliaria Pustulosa (Infetrop)Documento11 pagineMiliaria Pustulosa (Infetrop)Muhammad mukramNessuna valutazione finora
- Kuliah Sinkop UntadDocumento35 pagineKuliah Sinkop UntadMuhammad mukramNessuna valutazione finora
- Chickenpox (Varicella) : What Is Chickenpox? What Are The Symptoms of Chickenpox?Documento3 pagineChickenpox (Varicella) : What Is Chickenpox? What Are The Symptoms of Chickenpox?Muhammad mukramNessuna valutazione finora
- Varicella Zoster (Chickenpox) : Frequently Asked QuestionsDocumento2 pagineVaricella Zoster (Chickenpox) : Frequently Asked QuestionsMuhammad mukramNessuna valutazione finora
- Somatic Complaints in Depression Psikosomatik Untad 2012Documento19 pagineSomatic Complaints in Depression Psikosomatik Untad 2012Muhammad mukramNessuna valutazione finora
- Drugs For Special Population: Dr. Jarir at Thobari, MSC, PHD, FispeDocumento56 pagineDrugs For Special Population: Dr. Jarir at Thobari, MSC, PHD, FispeMuhammad mukramNessuna valutazione finora
- No No RM Nama JK UmurDocumento45 pagineNo No RM Nama JK UmurMuhammad mukramNessuna valutazione finora
- Management of Mental Disorder in AdolescentDocumento20 pagineManagement of Mental Disorder in AdolescentMuhammad mukramNessuna valutazione finora
- Diagram KimiaDocumento6 pagineDiagram KimiaMuhammad mukramNessuna valutazione finora
- Anxiety and Surgery UNTAD 2012Documento35 pagineAnxiety and Surgery UNTAD 2012Muhammad mukramNessuna valutazione finora
- Dermatitis: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDocumento30 pagineDermatitis: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityMuhammad mukramNessuna valutazione finora
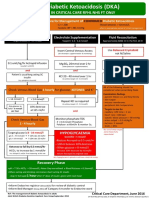
- Adult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyDocumento1 paginaAdult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyJung Bahadur SinghNessuna valutazione finora
- Randolph Cornelio M. Capon, BSN, RNDocumento42 pagineRandolph Cornelio M. Capon, BSN, RNhassen zabalaNessuna valutazione finora
- Diabetic EmergencyDocumento28 pagineDiabetic Emergencychandrima pattadarNessuna valutazione finora
- Case Study About Type II Diabetes MellitusDocumento84 pagineCase Study About Type II Diabetes MellitusMark Anthony S. Castillo89% (35)
- Notes ImDocumento5 pagineNotes Imsharmee sarmientaNessuna valutazione finora
- DiabetesDocumento12 pagineDiabetessshiffanaNessuna valutazione finora
- Jurnal Kad Dan HonkDocumento9 pagineJurnal Kad Dan Honksimpati91Nessuna valutazione finora
- Diabetes 2023Documento15 pagineDiabetes 2023Hira ijazNessuna valutazione finora
- EBEEDM Sample Questions FINAL 2018Documento66 pagineEBEEDM Sample Questions FINAL 2018Pamela Musabelliu100% (2)
- Dissecting The Interaction Between COVID-19 and Diabetes MellitusDocumento11 pagineDissecting The Interaction Between COVID-19 and Diabetes MellitusmehakNessuna valutazione finora
- SNB (SN) Question 2015 July 29Documento4 pagineSNB (SN) Question 2015 July 29phyo shan100% (2)
- WT OetDocumento13 pagineWT OetRomana PereiraNessuna valutazione finora
- Acid-Base Disorders in The Critically Ill PatientDocumento11 pagineAcid-Base Disorders in The Critically Ill PatientAniAliciaOrtizCastleNessuna valutazione finora
- Diabetes Complications Case StudyDocumento5 pagineDiabetes Complications Case StudyShiloh RiverNessuna valutazione finora
- Diabetes Mellitus: DefinitionDocumento95 pagineDiabetes Mellitus: DefinitionMalik Rizwan ElahiNessuna valutazione finora
- Diabetic Ketoacidosis in PregnancyDocumento12 pagineDiabetic Ketoacidosis in PregnancyMuhammad BilalNessuna valutazione finora
- The Doom and Bloom Making InsulinDocumento19 pagineThe Doom and Bloom Making InsulinkukhriNessuna valutazione finora
- EndocrinoDocumento15 pagineEndocrinoMichelle ElizaldeNessuna valutazione finora
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDocumento1 paginaJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandNessuna valutazione finora
- Fluids and Electrolytes - ExamDocumento6 pagineFluids and Electrolytes - ExamLouie Bello60% (5)
- Pharmacolgical Mangment of Diabetic Ketoacidosis: by Suliman OsmanDocumento27 paginePharmacolgical Mangment of Diabetic Ketoacidosis: by Suliman OsmanAymen OmerNessuna valutazione finora
- Monitorizarea Cardiaca Recunoasterea RitmurilorDocumento378 pagineMonitorizarea Cardiaca Recunoasterea Ritmurilorsun seal100% (1)
- Gastroparesis in Type 1 Diabetes Final Working PaperDocumento12 pagineGastroparesis in Type 1 Diabetes Final Working Paperapi-384481487Nessuna valutazione finora
- Diabetic Ketoacidosis: Mechanisms DiagnosisDocumento1 paginaDiabetic Ketoacidosis: Mechanisms Diagnosisricardo arreguiNessuna valutazione finora
- Acute Complications of Diabetes MellitusDocumento1 paginaAcute Complications of Diabetes MellitusGerardLum100% (1)
- Chapter 38: Care of Patients With Diabetes and Hypoglycemia: Multiple ChoiceDocumento13 pagineChapter 38: Care of Patients With Diabetes and Hypoglycemia: Multiple ChoiceNurse UtopiaNessuna valutazione finora
- Management of Diabetic KetoacidosisDocumento4 pagineManagement of Diabetic Ketoacidosiscarla jazmin cortes rodriguezNessuna valutazione finora
- DKA, HHS, HYPOGLYCEMIA MKDocumento42 pagineDKA, HHS, HYPOGLYCEMIA MKSol Gat ChupataNessuna valutazione finora
- Nursing Care of Client With Endocrine DisorderDocumento93 pagineNursing Care of Client With Endocrine DisorderApril_Anne_Vel_343Nessuna valutazione finora
- DocxDocumento20 pagineDocxHarrington_773951393100% (1)