Potrebbero piacerti anche
- TWU Anesthesia Cheat SheetDocumento2 pagineTWU Anesthesia Cheat Sheetinvading_jam7582100% (5)
- 2019 Practice of Anesthesia For Infants and ChildrenDocumento2 pagine2019 Practice of Anesthesia For Infants and ChildrenJavier GlezqNessuna valutazione finora
- Metabolic Stress Case StudyDocumento10 pagineMetabolic Stress Case StudydakotaNessuna valutazione finora
- The Behavioral Objectives For The Teaching Plan DiabetesDocumento2 pagineThe Behavioral Objectives For The Teaching Plan DiabetesKaren Leigh Magsino100% (3)
- Dka CalculatorDocumento1 paginaDka CalculatordelfiaNessuna valutazione finora
- DKACalculatorDocumento1 paginaDKACalculatorRitch BassNessuna valutazione finora
- Principles of Management of DKADocumento4 paginePrinciples of Management of DKAHassen Kavi IsseNessuna valutazione finora
- Map DkaDocumento1 paginaMap DkaSH PrageethNessuna valutazione finora
- Guideline For The Management of Adults Patients With DKA or HHSDocumento3 pagineGuideline For The Management of Adults Patients With DKA or HHSJonard GiloNessuna valutazione finora
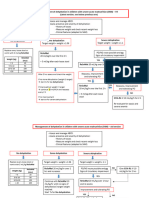
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedDocumento2 paginePediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaNessuna valutazione finora
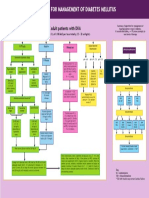
- DM Diabetic Ketoacidosis DKA Management Algorithm Adult Patients 2019Documento1 paginaDM Diabetic Ketoacidosis DKA Management Algorithm Adult Patients 2019Hendra AfrilaNessuna valutazione finora
- DKA AlgorismDocumento2 pagineDKA AlgorismYohannes hailuNessuna valutazione finora
- G CarbamazepineDocumento18 pagineG CarbamazepineCLARISSA GRACE GERALDINONessuna valutazione finora
- Quick Reference Guide Corrections 2021Documento6 pagineQuick Reference Guide Corrections 2021Prashin RocharamNessuna valutazione finora
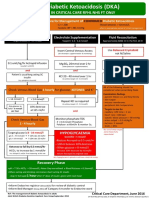
- Adult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyDocumento1 paginaAdult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyJung Bahadur SinghNessuna valutazione finora
- Kuwait PICU Taskforce DKA V1 5 June 2022Documento2 pagineKuwait PICU Taskforce DKA V1 5 June 2022Emad MashaalNessuna valutazione finora
- Electrolyte Replacement Infusions Pediatrics 0713Documento2 pagineElectrolyte Replacement Infusions Pediatrics 0713Hakobito Dela RosaNessuna valutazione finora
- DKA/HHS Pathway Phase 1 (Adult)Documento6 pagineDKA/HHS Pathway Phase 1 (Adult)marshaNessuna valutazione finora
- Dka CalculatorDocumento1 paginaDka CalculatorTalib AdilNessuna valutazione finora
- Adult: Diabetic Emergencies: Care Protocol and ChartDocumento4 pagineAdult: Diabetic Emergencies: Care Protocol and ChartvladhdNessuna valutazione finora
- DKA GuidelineDocumento1 paginaDKA GuidelineIvonneRemigioNessuna valutazione finora
- Decontamination Information: BathingDocumento2 pagineDecontamination Information: BathingNaNessuna valutazione finora
- Notes in Neonates محمد ابراهيم مستشفى قوص قنا.WhiteKnightLoveDocumento77 pagineNotes in Neonates محمد ابراهيم مستشفى قوص قنا.WhiteKnightLoveMaRwa IbrahimNessuna valutazione finora
- Item 6f - Acute Management of Hyperosmolar Hyperglycaemic StateDocumento1 paginaItem 6f - Acute Management of Hyperosmolar Hyperglycaemic StateStef AnNessuna valutazione finora
- Treatment of Acute Hypokalaemia in AdultsDocumento4 pagineTreatment of Acute Hypokalaemia in AdultsEmaNessuna valutazione finora
- ER Clinical NotesDocumento23 pagineER Clinical NotesmngaNessuna valutazione finora
- EPALS DKA Flowchart Jan 23 V4Documento1 paginaEPALS DKA Flowchart Jan 23 V4Miguel BaiaNessuna valutazione finora
- Routine Anesthesia Set UpDocumento4 pagineRoutine Anesthesia Set UpSteve Johnstone100% (2)
- Fluid and Electrolytes ManagementDocumento21 pagineFluid and Electrolytes ManagementRasYa DINessuna valutazione finora
- SAM Dehydration Algorithm - 29042021Documento2 pagineSAM Dehydration Algorithm - 29042021samarmojeebNessuna valutazione finora
- Digoxin Phenytoin Cyclosporin e Tacrolimu S Sirolimus Lithium CBZ VA PhenobarbDocumento5 pagineDigoxin Phenytoin Cyclosporin e Tacrolimu S Sirolimus Lithium CBZ VA PhenobarbDana MradNessuna valutazione finora
- حسابات الجرعة basharDocumento7 pagineحسابات الجرعة basharابو الخطابNessuna valutazione finora
- Dehydration - PedsCase - v9Documento1 paginaDehydration - PedsCase - v9Chinenye ModestaNessuna valutazione finora
- TPNDocumento4 pagineTPNQwerqwe QweqweNessuna valutazione finora
- COVID MX BsmmuDocumento2 pagineCOVID MX BsmmuNuhiat NahreenNessuna valutazione finora
- Female TPN FormulaDocumento2 pagineFemale TPN FormulaAnna's JourneyNessuna valutazione finora
- Fluid Therapy in Paediatrics - RevisedDocumento5 pagineFluid Therapy in Paediatrics - RevisedJehangir AllamNessuna valutazione finora
- Intravenous Infusion Orders For Common Medications in The ED and ICU - Bunbury HospitalDocumento39 pagineIntravenous Infusion Orders For Common Medications in The ED and ICU - Bunbury Hospital9wb646hq7mNessuna valutazione finora
- DKA Protocol TGDocumento11 pagineDKA Protocol TGabelNessuna valutazione finora
- ÷ Weight (KG) Dilute 1 ML (500mcg) of PGE1 With NS/ D5% To Yield The Total Volume From #1Documento14 pagine÷ Weight (KG) Dilute 1 ML (500mcg) of PGE1 With NS/ D5% To Yield The Total Volume From #1Nesreen G MohammedNessuna valutazione finora
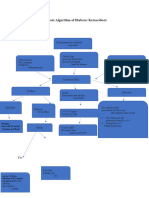
- Dka AlgorithmDocumento1 paginaDka AlgorithmAbhinav AggarwalNessuna valutazione finora
- Disaster Lecture MidtermsDocumento8 pagineDisaster Lecture MidtermsMae Arra Lecobu-anNessuna valutazione finora
- IV Fluid ChartDocumento2 pagineIV Fluid Chartbenny christantoNessuna valutazione finora
- DKA Protocol With Calculation SheetDocumento7 pagineDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNessuna valutazione finora
- Generic Name:: ElectrolytesDocumento9 pagineGeneric Name:: ElectrolytesEleazar Desillarico GonzalesNessuna valutazione finora
- CalciumchannelalgorithmDocumento1 paginaCalciumchannelalgorithmLind YLNessuna valutazione finora
- Pcol Lab MidtermsDocumento13 paginePcol Lab Midtermsellyzamarie08Nessuna valutazione finora
- Seizure and Anticonvulsant Medications GridDocumento1 paginaSeizure and Anticonvulsant Medications Gridpiyush RautNessuna valutazione finora
- Methanol Poisoning at A Glance PDFDocumento2 pagineMethanol Poisoning at A Glance PDFAmeer MattaNessuna valutazione finora
- Diabetes Mellitus in Pediatric: Dr. Wasnaa Hadi AbdullahDocumento30 pagineDiabetes Mellitus in Pediatric: Dr. Wasnaa Hadi AbdullahLily AddamsNessuna valutazione finora
- Guidelines and Protocols Of: Diabetes EmergenciesDocumento36 pagineGuidelines and Protocols Of: Diabetes Emergenciesyassen hassanNessuna valutazione finora
- AppendicitisDocumento2 pagineAppendicitisYosuaNessuna valutazione finora
- Decreased Consciousness ConsciousDocumento3 pagineDecreased Consciousness ConsciousEdRobertArnadNessuna valutazione finora
- شرح بسيط - 100252Documento2 pagineشرح بسيط - 100252magedsaif88Nessuna valutazione finora
- Drugs Reconst. Dilution Stability After Reconst. Dose Adjustment Infusion Rate NotesDocumento13 pagineDrugs Reconst. Dilution Stability After Reconst. Dose Adjustment Infusion Rate NotesRania ElwatidyNessuna valutazione finora
- Dka 1Documento34 pagineDka 1Anne Lorraine BringasNessuna valutazione finora
- 4 12 ToxicologyDocumento8 pagine4 12 ToxicologyLionelWrightNessuna valutazione finora
- Nomogram For Adjusting Unfractionated Heparin in Adults Using Anti-Factor Xa Activity or The aPTTDocumento2 pagineNomogram For Adjusting Unfractionated Heparin in Adults Using Anti-Factor Xa Activity or The aPTTLulwaNessuna valutazione finora
- Notes ImDocumento5 pagineNotes Imsharmee sarmientaNessuna valutazione finora
- Condition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockDocumento4 pagineCondition Formula IV Fluid Acute Gastroenteritis A. Severe Acute Malnutrition (SAM) Source: WHO?? 1. in ShockJohnPaulOliverosNessuna valutazione finora
- S2 2015 351938 BibliographyDocumento11 pagineS2 2015 351938 BibliographyPutriSakinahNessuna valutazione finora
- Intermittent Fasting Facts and Myths: Metabolic Benefits of Intermittent FastingDocumento4 pagineIntermittent Fasting Facts and Myths: Metabolic Benefits of Intermittent FastingIJAR JOURNALNessuna valutazione finora
- A Case of Possible Hypersensitivity Reactions To Human InsulinDocumento6 pagineA Case of Possible Hypersensitivity Reactions To Human Insulingandik danu pramigaNessuna valutazione finora
- Full Download Ebook PDF Lehnes Pharmacotherapeutics For Advanced Practice Providers PDFDocumento41 pagineFull Download Ebook PDF Lehnes Pharmacotherapeutics For Advanced Practice Providers PDFeleanor.jones934100% (31)
- International Journal of Trend in Scientific Research and Development (IJTSRD)Documento7 pagineInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNessuna valutazione finora
- Tobacco Consumption and The Effects 2 (Autosaved) .EditedDocumento10 pagineTobacco Consumption and The Effects 2 (Autosaved) .EditedMarvin CJNessuna valutazione finora
- DiabeteK - PPT Assignment For BioentrepreneurDocumento8 pagineDiabeteK - PPT Assignment For BioentrepreneurAbhishek AdhikariNessuna valutazione finora
- Diabetes Mellitus Concept MapDocumento2 pagineDiabetes Mellitus Concept MapIzhra Margate100% (5)
- 6.diabetes Education in ChilDocumento9 pagine6.diabetes Education in ChilWahyu Dwi NugrohoNessuna valutazione finora
- A Risk Prediction Model For Heart Failure Hospitalization JuroanlDocumento20 pagineA Risk Prediction Model For Heart Failure Hospitalization JuroanljamesboendNessuna valutazione finora
- Medical ManagementDocumento3 pagineMedical ManagementMark Jefferson LunaNessuna valutazione finora
- The Rediscovery of Water Only FastingDocumento6 pagineThe Rediscovery of Water Only FastingVince SardinaNessuna valutazione finora
- Neuro WorkbookDocumento4 pagineNeuro Workbookclairealcober1Nessuna valutazione finora
- Cues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationDocumento3 pagineCues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationLouwella RamosNessuna valutazione finora
- Health Protection and Improvement.Documento22 pagineHealth Protection and Improvement.Abhipriyo BanerjeeNessuna valutazione finora
- Blood GlucoseDocumento3 pagineBlood GlucoseChamCham AquinoNessuna valutazione finora
- Research Proposal: Mara College Kuala NerangDocumento10 pagineResearch Proposal: Mara College Kuala NerangAnwar Asyhraff0% (1)
- Hypoglycemic Effect of Avocado Seed Extract (Persean: Americana Mill) From Analysis of Oral Glucose ToleranceDocumento8 pagineHypoglycemic Effect of Avocado Seed Extract (Persean: Americana Mill) From Analysis of Oral Glucose ToleranceRecky PatalaNessuna valutazione finora
- Assignment 3Documento32 pagineAssignment 3kiran shaheen100% (1)
- The Weight Loss ManualDocumento56 pagineThe Weight Loss ManualSomashekarNessuna valutazione finora
- CPG Management of Type 2 Diabetes Mellitus (4th Edition)Documento84 pagineCPG Management of Type 2 Diabetes Mellitus (4th Edition)apalaginih100% (3)
- Vocabulary 2 KeperawatanDocumento9 pagineVocabulary 2 KeperawatanSoull MechaniccNessuna valutazione finora
- Method SujokDocumento4 pagineMethod Sujokbhupatin100% (6)
- Synthesis and Characterization of Solanum Nigrum MDocumento9 pagineSynthesis and Characterization of Solanum Nigrum MvenaNessuna valutazione finora
- Control System For Insulin PumpDocumento5 pagineControl System For Insulin PumpAdeyemiNessuna valutazione finora
- After Meal Control GscheinerDocumento40 pagineAfter Meal Control GscheinerLlana Pauline JacintoNessuna valutazione finora
- How To Write A 8-10 Page Research PaperDocumento8 pagineHow To Write A 8-10 Page Research Paperjpkoptplg100% (1)
- Pathophysiology Dyslipidemia PDFDocumento9 paginePathophysiology Dyslipidemia PDFtiffa07110% (1)
- SAF General Medicine 17-03-2020Documento43 pagineSAF General Medicine 17-03-2020manoj yadavNessuna valutazione finora