Potrebbero piacerti anche
- Handbook for the Assessment of Driving CapacityDa EverandHandbook for the Assessment of Driving CapacityMaria T. SchultheisNessuna valutazione finora
- Validity of The Cognitive Behavioral Driver's Inventory in Predicting Driving OutcomeDocumento8 pagineValidity of The Cognitive Behavioral Driver's Inventory in Predicting Driving OutcomeAnonymous 3SZxXHNessuna valutazione finora
- SOKRATIS Driving Thessaloniki Alzheimer 2019 - 2Documento51 pagineSOKRATIS Driving Thessaloniki Alzheimer 2019 - 2Sokratis PapageorgiouNessuna valutazione finora
- Practice Parameter: Diagnostic Assessment of The Child With Cerebral Palsy (CP)Documento80 paginePractice Parameter: Diagnostic Assessment of The Child With Cerebral Palsy (CP)bobo boboNessuna valutazione finora
- Chairman's Report Final Exam 2016.2 General CommentsDocumento12 pagineChairman's Report Final Exam 2016.2 General CommentsJane KoNessuna valutazione finora
- General Comments: Chair's Report Final Exam 2019.1Documento19 pagineGeneral Comments: Chair's Report Final Exam 2019.1Jane KoNessuna valutazione finora
- Presented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDocumento22 paginePresented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDanielle Stella N'LucaNessuna valutazione finora
- Community Mobility: Driving As An OccupationDocumento59 pagineCommunity Mobility: Driving As An Occupationmona alkhudairNessuna valutazione finora
- May 2016 Exam ReportDocumento16 pagineMay 2016 Exam ReportJane KoNessuna valutazione finora
- Iverson - 10 - Dementia and Driving ConsensusDocumento11 pagineIverson - 10 - Dementia and Driving Consensusmadalena limaNessuna valutazione finora
- Cataract Surgical Coverage and Outcome in The Tibet Autonomous RegionDocumento5 pagineCataract Surgical Coverage and Outcome in The Tibet Autonomous RegionLina Shabrina QoribNessuna valutazione finora
- May 2018 Exam ReportDocumento16 pagineMay 2018 Exam ReportJane KoNessuna valutazione finora
- General Comments: Chair's Report Final Exam 2018.2Documento16 pagineGeneral Comments: Chair's Report Final Exam 2018.2Jane KoNessuna valutazione finora
- The Driving Dilemma: Theresa Braford MHS, OTR/LDocumento30 pagineThe Driving Dilemma: Theresa Braford MHS, OTR/LFandf HomesNessuna valutazione finora
- May 2015 Exam ReportDocumento19 pagineMay 2015 Exam ReportJane KoNessuna valutazione finora
- May 2014 Exam ReportDocumento20 pagineMay 2014 Exam ReportJane KoNessuna valutazione finora
- Summary, Conclusion and RecommendationDocumento9 pagineSummary, Conclusion and RecommendationCharles BognotNessuna valutazione finora
- Project Title: A Machine Learning Methodology For Diagnosing Chronic Kidney DiseaseDocumento11 pagineProject Title: A Machine Learning Methodology For Diagnosing Chronic Kidney Diseasefdfdfdfd100% (1)
- 5 Annual Meeting of The Washington Group On Disability StatisticsDocumento105 pagine5 Annual Meeting of The Washington Group On Disability StatisticsChia GarciaNessuna valutazione finora
- Orthotics Consensus Conference ReportDocumento354 pagineOrthotics Consensus Conference ReportAlec joshua RapadaNessuna valutazione finora
- Observational Study For Determining The Percentage of Vehicles Completely Stopping at An All-Way Stop-Sign IntersectionDocumento27 pagineObservational Study For Determining The Percentage of Vehicles Completely Stopping at An All-Way Stop-Sign IntersectionRaj Kishore100% (6)
- Natural History and Outcome of Optic Pathway Gliomas in ChildrenDocumento7 pagineNatural History and Outcome of Optic Pathway Gliomas in ChildrenCamilo Benavides BurbanoNessuna valutazione finora
- Dyslipidaemia GuidelinesDocumento28 pagineDyslipidaemia GuidelinesEllieNessuna valutazione finora
- ABO American Board of Orthodontics 2013-CALIBRATION-KIT PDFDocumento63 pagineABO American Board of Orthodontics 2013-CALIBRATION-KIT PDFEryson Thiago PradoNessuna valutazione finora
- ABO American Board of Orthodontics 2013-CALIBRATION-KITDocumento63 pagineABO American Board of Orthodontics 2013-CALIBRATION-KITEryson Thiago PradoNessuna valutazione finora
- RSNA 2014 BalfeDocumento39 pagineRSNA 2014 BalfeyfaynerNessuna valutazione finora
- Geriatric ScoreDocumento16 pagineGeriatric ScoreJemsner IrothNessuna valutazione finora
- Visual and Cognitive Predictors of Driving SafetyDocumento11 pagineVisual and Cognitive Predictors of Driving SafetyNelly LeónNessuna valutazione finora
- The Acceptance of Using Virtualreality in ADocumento2 pagineThe Acceptance of Using Virtualreality in AJENIFER KARINA PUTZ LORENZINessuna valutazione finora
- Kedokteran - Pengendara Sebagai Faktor Risiko Terjadinya Kecelakaan Lalu Lintas Sepeda Motor Tahun 2010Documento7 pagineKedokteran - Pengendara Sebagai Faktor Risiko Terjadinya Kecelakaan Lalu Lintas Sepeda Motor Tahun 2010Gaspar TuamesNessuna valutazione finora
- New Standards and Guidelines For Drivers With Obstructive Sleep Apnoea SyndromeDocumento49 pagineNew Standards and Guidelines For Drivers With Obstructive Sleep Apnoea Syndromea3llamNessuna valutazione finora
- Guidelines: Recommendations On Screening For Colorectal Cancer in Primary CareDocumento9 pagineGuidelines: Recommendations On Screening For Colorectal Cancer in Primary CarezhazhapatrisaNessuna valutazione finora
- Guidance Stepwise Final 04 10 2012Documento60 pagineGuidance Stepwise Final 04 10 2012daku dakunaNessuna valutazione finora
- PinetoDocumento2 paginePinetocarlo47Nessuna valutazione finora
- Colorectal Final EvidsummaryDocumento19 pagineColorectal Final Evidsummaryppdsipd2019Nessuna valutazione finora
- PIIS0741521416300027 DapusDocumento21 paginePIIS0741521416300027 DapusKevin AdrianNessuna valutazione finora
- A Clustering of Injury BehaviorsDocumento5 pagineA Clustering of Injury BehaviorsfivekujakartaNessuna valutazione finora
- Ayat and DuaaDocumento16 pagineAyat and Duaaايات حسن كريم عبد الله البديري البديريNessuna valutazione finora
- The 10 Min Geriatric AssessmentDocumento44 pagineThe 10 Min Geriatric AssessmentAndy F MonroeNessuna valutazione finora
- Strokeaha 108 532069Documento6 pagineStrokeaha 108 532069Alexandra PopNessuna valutazione finora
- Driving Simulation For Evaluation and Rehabilitation of Driving After StrokeDocumento9 pagineDriving Simulation For Evaluation and Rehabilitation of Driving After StrokeMar Ruiz CuadraNessuna valutazione finora
- Young Driver Safety Solutions To An AgeDocumento100 pagineYoung Driver Safety Solutions To An AgeSilvana BogićevićNessuna valutazione finora
- 5621 WardDocumento31 pagine5621 Ward_maghus_Nessuna valutazione finora
- Assessing Older DriversDocumento5 pagineAssessing Older DriversArt SmithNessuna valutazione finora
- Appleton Area Recreation Park Visitor SurveyDocumento20 pagineAppleton Area Recreation Park Visitor SurveyWest Central TribuneNessuna valutazione finora
- Bisha10 1007@BF00942931Documento5 pagineBisha10 1007@BF00942931mahvd2010Nessuna valutazione finora
- Evaluating The Quality, Utility and Reliability of Information in Uveitis Videos Shared On YoutubeDocumento12 pagineEvaluating The Quality, Utility and Reliability of Information in Uveitis Videos Shared On Youtubearifin85drNessuna valutazione finora
- Three-Year Follow-Up of A Randomized Trial Comparing Focal/Grid Photocoagulation and Intravitreal Triamcinolone For Diabetic Macular EdemaDocumento7 pagineThree-Year Follow-Up of A Randomized Trial Comparing Focal/Grid Photocoagulation and Intravitreal Triamcinolone For Diabetic Macular EdemaDikiArmaDuhaAlaydrusNessuna valutazione finora
- التقييم الدوري والترقية السنوية جراحة المسالكDocumento5 pagineالتقييم الدوري والترقية السنوية جراحة المسالكMohammed GorjiNessuna valutazione finora
- Comparison of Driving Difficulty Between Bilateral Cataract and Non-Cataract Elderly Drivers in Malaysia: A Preliminary StudyDocumento8 pagineComparison of Driving Difficulty Between Bilateral Cataract and Non-Cataract Elderly Drivers in Malaysia: A Preliminary StudyKris AdinataNessuna valutazione finora
- Acute Kidney Injury: Uth Renal Lecture Erica Bjornstad, MD, PHD, MPH February 2020Documento124 pagineAcute Kidney Injury: Uth Renal Lecture Erica Bjornstad, MD, PHD, MPH February 2020King MazingaNessuna valutazione finora
- Lau 2002Documento6 pagineLau 2002Nylla Shin Hyenna LieNessuna valutazione finora
- Program DirectorDocumento172 pagineProgram DirectorzigetgooNessuna valutazione finora
- Interpretation: L23 - FPSC Malviya Nagar1 A-88 Shivanand Marg, Malviyanagar JaipurDocumento4 pagineInterpretation: L23 - FPSC Malviya Nagar1 A-88 Shivanand Marg, Malviyanagar Jaipurmahima goyalNessuna valutazione finora
- Reject Analysis: A Low Tech Solution?Documento19 pagineReject Analysis: A Low Tech Solution?Irham Fathurrahman100% (1)
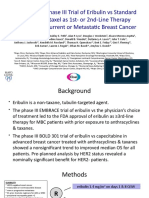
- Randomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast CancerDocumento14 pagineRandomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast Canceralberto cabelloNessuna valutazione finora
- State Urology Workforce Practice USDocumento97 pagineState Urology Workforce Practice USDominic FerraoNessuna valutazione finora
- Online Appendix D12 (Pleural Disease) - Pleural Malignancy Prognostic ScoresDocumento6 pagineOnline Appendix D12 (Pleural Disease) - Pleural Malignancy Prognostic Scores4wntsgj69pNessuna valutazione finora
- Eman Abdulla Al JahmiDocumento46 pagineEman Abdulla Al JahmiVivi Aisyah BndowosoNessuna valutazione finora
- Indice MotorDocumento4 pagineIndice Motormanu122114Nessuna valutazione finora
- TuberkulosisanakDocumento106 pagineTuberkulosisanakUdin NicotinicNessuna valutazione finora
- Comprehensive Geriatric Assessment Proforma Apr-15Documento11 pagineComprehensive Geriatric Assessment Proforma Apr-15Udin Nicotinic100% (2)
- Occupational DermatitisDocumento5 pagineOccupational DermatitisUdin NicotinicNessuna valutazione finora
- Allergic Rhinitis and RhinosinusitisDocumento54 pagineAllergic Rhinitis and RhinosinusitisUdin NicotinicNessuna valutazione finora
- Management of Acute Malnutrition PDFDocumento9 pagineManagement of Acute Malnutrition PDFUdin NicotinicNessuna valutazione finora
- Speech and Language DelayDocumento6 pagineSpeech and Language DelayLianda Destrin NurfadilahNessuna valutazione finora
- Nosocomial Bacteremia in Perspective: A Community - Wide StudyDocumento21 pagineNosocomial Bacteremia in Perspective: A Community - Wide StudyUdin NicotinicNessuna valutazione finora
- 1 CoverDocumento3 pagine1 CoverUnaBaNaNaNessuna valutazione finora
- Mioma WilliamsDocumento16 pagineMioma WilliamsUdin NicotinicNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaUdin NicotinicNessuna valutazione finora
- Trauma AbdomenDocumento13 pagineTrauma AbdomenUdin NicotinicNessuna valutazione finora
- EbookDocumento8 pagineEbookUdin NicotinicNessuna valutazione finora
- Diagnosis AnemiaDocumento28 pagineDiagnosis AnemiaUdin NicotinicNessuna valutazione finora
- Gerontological Nursing 2021Documento157 pagineGerontological Nursing 2021Andrew Isiah BonifacioNessuna valutazione finora
- Personal Development Quarter 1-Module 5: Powers of The MindDocumento33 paginePersonal Development Quarter 1-Module 5: Powers of The MindJenny E. Forcadilla100% (3)
- Varun Kumar, 2017 - Getting Started in PsychiatryDocumento148 pagineVarun Kumar, 2017 - Getting Started in PsychiatryBernard FZ100% (1)
- Mental Health in Older AdultsDocumento14 pagineMental Health in Older AdultsAlyssa NicoleNessuna valutazione finora
- 12 Best Brain Foods Memory Concentration AnDocumento10 pagine12 Best Brain Foods Memory Concentration AnRovin RamphalNessuna valutazione finora
- Downtime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimeDocumento5 pagineDowntime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimerupaliNessuna valutazione finora
- NeuroscienceDocumento92 pagineNeurosciencetimea_gheneaNessuna valutazione finora
- GERO FINAL Flashcards - Questions and Answers - QuizletDocumento19 pagineGERO FINAL Flashcards - Questions and Answers - QuizletNur SanaaniNessuna valutazione finora
- On Dementia and Other Cognitive DisordersDocumento14 pagineOn Dementia and Other Cognitive DisordersasclepiuspdfsNessuna valutazione finora
- Seth References To DimensionsDocumento8 pagineSeth References To DimensionsStephani BommaritoNessuna valutazione finora
- Vascular Dementia - Symptoms & TreatmentsDocumento9 pagineVascular Dementia - Symptoms & TreatmentsRatnaPrasadNalamNessuna valutazione finora
- Escala Internacional de Demencia HIVDocumento8 pagineEscala Internacional de Demencia HIVctobonaNessuna valutazione finora
- Interpersonal Communication in Older Adulthood - Interdisciplinary Theory and Research 1994, SAGEDocumento281 pagineInterpersonal Communication in Older Adulthood - Interdisciplinary Theory and Research 1994, SAGERubén JacobNessuna valutazione finora
- Dementia FinalDocumento80 pagineDementia FinalAbelNessuna valutazione finora
- Towards A Dementia Plan: A WHO GuideDocumento82 pagineTowards A Dementia Plan: A WHO GuideMark Gilbert MilallosNessuna valutazione finora
- About Frontotemporal DementiaDocumento2 pagineAbout Frontotemporal DementiaRuwanthi FonsekaNessuna valutazione finora
- Psychiatry Image BankDocumento117 paginePsychiatry Image BankSameeksha DasNessuna valutazione finora
- Psychological Assessment: (Insert and PDF Palihug Te Hehe)Documento6 paginePsychological Assessment: (Insert and PDF Palihug Te Hehe)Casas, Jo-an Pauline A.100% (1)
- Brain Health Breakthroughs-13 Memory FoodsDocumento30 pagineBrain Health Breakthroughs-13 Memory FoodsNiftyNessuna valutazione finora
- Case 2Documento155 pagineCase 2Jade HemmingsNessuna valutazione finora
- CHC43015-AC-Subject 5-AWB-F-v.2.1Documento47 pagineCHC43015-AC-Subject 5-AWB-F-v.2.1Virender Arya78% (9)
- Effectiveness of Physical Activity Interventions For Improving Depression, Anxiety and DistressDocumento10 pagineEffectiveness of Physical Activity Interventions For Improving Depression, Anxiety and DistressDouglas SantosNessuna valutazione finora
- Ideal Discharge Elderly PatientDocumento3 pagineIdeal Discharge Elderly PatientFelicia Risca RyandiniNessuna valutazione finora
- WP contentuploads202209BRAVE Ebook No Brainer PDFDocumento24 pagineWP contentuploads202209BRAVE Ebook No Brainer PDFDacianaNessuna valutazione finora
- Organic Mental DisordersDocumento6 pagineOrganic Mental Disorderspriya maneshNessuna valutazione finora
- SCE Geriatrics CompressedDocumento434 pagineSCE Geriatrics CompressedFaris FirasNessuna valutazione finora
- NCM 114 Topic 4 Comprehensive Geriatric AssessmentDocumento16 pagineNCM 114 Topic 4 Comprehensive Geriatric AssessmentCaitlynNessuna valutazione finora
- Stahl's Essential Psychopharmacology - 5th EditionDocumento640 pagineStahl's Essential Psychopharmacology - 5th EditionCátia Ramos85% (55)
- Reaction Paper (Webinar)Documento2 pagineReaction Paper (Webinar)Aime MvuyekureNessuna valutazione finora
- Sensory Stimulation in Dementia CareDocumento12 pagineSensory Stimulation in Dementia CareNikki SwiftNessuna valutazione finora