Potrebbero piacerti anche
- Computation Sheet of Taxable Income & Income TaxDocumento2 pagineComputation Sheet of Taxable Income & Income TaxPandu DoradlaNessuna valutazione finora
- Purchase OrderDocumento2 paginePurchase Ordershakeel ahmedNessuna valutazione finora
- FW WP Appln FormDocumento22 pagineFW WP Appln Formsanjayak_3Nessuna valutazione finora
- Praveen KumarDocumento3 paginePraveen Kumarvidhi09Nessuna valutazione finora
- Nalco Tender - 1 PDFDocumento3 pagineNalco Tender - 1 PDFRajiv PoddarNessuna valutazione finora
- EPOnlineSvcAccessApplnForm CompileDocumento11 pagineEPOnlineSvcAccessApplnForm CompileRia ArguellesNessuna valutazione finora
- Leave Certificate: 08 May 2017 Tele/ Mob No Adjt-09596384093, MTO - 09596384093, SMDocumento1 paginaLeave Certificate: 08 May 2017 Tele/ Mob No Adjt-09596384093, MTO - 09596384093, SMramNessuna valutazione finora
- BLSPM3354H Partb 2021-22Documento3 pagineBLSPM3354H Partb 2021-22kumar reddyNessuna valutazione finora
- Purchase Order: Po No. DatedDocumento3 paginePurchase Order: Po No. DatedHolly SmithNessuna valutazione finora
- Read The Instructions Carefully:: WWW - Tnpsc.gov - inDocumento2 pagineRead The Instructions Carefully:: WWW - Tnpsc.gov - inJana VinayaNessuna valutazione finora
- Account Statement: Page 1 of 3Documento3 pagineAccount Statement: Page 1 of 3achyut kumarNessuna valutazione finora
- Reviewprint2 JSP PDFDocumento5 pagineReviewprint2 JSP PDFArnel GabiolaNessuna valutazione finora
- Booking Request ID: Visiting Purpose: Booking Confirmed On: SubjectDocumento2 pagineBooking Request ID: Visiting Purpose: Booking Confirmed On: SubjectManoj GoyalNessuna valutazione finora
- Booking Request ID: Visiting Purpose: Booking Confirmed On: SubjectDocumento1 paginaBooking Request ID: Visiting Purpose: Booking Confirmed On: SubjectPratik SharmaNessuna valutazione finora
- PO No. 91578 KohinoorDocumento2 paginePO No. 91578 KohinoorVipul RathodNessuna valutazione finora
- Delhi Hudco PDFDocumento1 paginaDelhi Hudco PDFrobbin singhNessuna valutazione finora
- Avishek LGTCS Trade LicenceDocumento1 paginaAvishek LGTCS Trade LicenceRidan DasNessuna valutazione finora
- Statement of Account: Date Transaction Type Amount NAV in INR (RS.) Price in INR (RS.) Number of Units Balance UnitDocumento1 paginaStatement of Account: Date Transaction Type Amount NAV in INR (RS.) Price in INR (RS.) Number of Units Balance Unitee206023Nessuna valutazione finora
- Holiday Home Booking 10 Oct 2016Documento2 pagineHoliday Home Booking 10 Oct 2016NityapriyaSrivastavaNessuna valutazione finora
- Udhyam RegistrationDocumento1 paginaUdhyam RegistrationDeepanshu Singh PanwarNessuna valutazione finora
- (A Government of India Enterprise) : Investment Details Details of Pending TY AdvancesDocumento1 pagina(A Government of India Enterprise) : Investment Details Details of Pending TY AdvancesindianroadromeoNessuna valutazione finora
- Account Statement: Folio Number: 1038047310Documento2 pagineAccount Statement: Folio Number: 1038047310Rajat RK KumarNessuna valutazione finora
- Tasleem MayDocumento2 pagineTasleem MayManthan ShahNessuna valutazione finora
- Udyam Up 27 0009505Documento1 paginaUdyam Up 27 0009505Rishi YadavNessuna valutazione finora
- Holiday HomesDocumento3 pagineHoliday HomesAnkit RajodiaNessuna valutazione finora
- Appointment SlipDocumento1 paginaAppointment SlipSwapnil RoyNessuna valutazione finora
- Government of India Directorate of Estates Regions Section, Nirman Bhawan, New Delhi-110108Documento1 paginaGovernment of India Directorate of Estates Regions Section, Nirman Bhawan, New Delhi-110108robbin singhNessuna valutazione finora
- Ldnov - Dec18551371124 2Documento1 paginaLdnov - Dec18551371124 2p_panchal82Nessuna valutazione finora
- Madhav Institute of Technology & Science, Gwalior: Examination Admit Card (Eac)Documento1 paginaMadhav Institute of Technology & Science, Gwalior: Examination Admit Card (Eac)Rohan MalakarNessuna valutazione finora
- Ruby General Hospital LTDDocumento1 paginaRuby General Hospital LTDSaurav PeriwalNessuna valutazione finora
- 1Documento4 pagine1Abhishek SinghviNessuna valutazione finora
- Tax Invoice: Original For RecipientDocumento6 pagineTax Invoice: Original For RecipientHarshal KolheNessuna valutazione finora
- 6500016884Documento7 pagine6500016884hfewkorbaNessuna valutazione finora
- Policy Schedule Cum Certificate of InsuranceDocumento2 paginePolicy Schedule Cum Certificate of Insurance058 PAUL MICHAEL SNessuna valutazione finora
- Holiday Home PDFDocumento1 paginaHoliday Home PDFMurthy NarasimhaNessuna valutazione finora
- Central Board of Secondary Education: Result: PassDocumento1 paginaCentral Board of Secondary Education: Result: PassYashNessuna valutazione finora
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Documento3 pagineForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Manav ChaudharyNessuna valutazione finora
- Acctstmt FDocumento3 pagineAcctstmt FAbhay SinghNessuna valutazione finora
- Salary Slip (00143059 December, 2015)Documento1 paginaSalary Slip (00143059 December, 2015)Aurang Zeb KhanNessuna valutazione finora
- HTTP Eawas - Nic.in Reports Rwservlet Server Rep Oramid Report Home1 Project Folder Holiday HH Booking Request1Documento1 paginaHTTP Eawas - Nic.in Reports Rwservlet Server Rep Oramid Report Home1 Project Folder Holiday HH Booking Request1Mohit DhakerNessuna valutazione finora
- Fee ReceiptDocumento1 paginaFee ReceiptShashankNessuna valutazione finora
- Ashutosh Resume 1Documento2 pagineAshutosh Resume 1Ashutosh samantarayNessuna valutazione finora
- Strategies ManagementDocumento2 pagineStrategies ManagementAkila Bosco100% (1)
- Admit Card Computer Based Online Test For Recruitment of Staff Nurse - 2445 VACANCIES ADVERTISED DATED - 18.10.2021Documento4 pagineAdmit Card Computer Based Online Test For Recruitment of Staff Nurse - 2445 VACANCIES ADVERTISED DATED - 18.10.2021saurav kumarNessuna valutazione finora
- NOC Letter - MuhammadDocumento1 paginaNOC Letter - MuhammadDoctor JrNessuna valutazione finora
- Milan Admission LetterDocumento1 paginaMilan Admission LetterPatel MilankumarNessuna valutazione finora
- Ack NSDL000043902Documento1 paginaAck NSDL000043902JohnsonNessuna valutazione finora
- Motor Insurance - Miscellaneous Carrying Comprehensive: Certificate of Insurance Cum Policy ScheduleDocumento3 pagineMotor Insurance - Miscellaneous Carrying Comprehensive: Certificate of Insurance Cum Policy ScheduleShiva DegaNessuna valutazione finora
- ConsolidatedMarksheet R210823018492Documento1 paginaConsolidatedMarksheet R210823018492Ritik VermaNessuna valutazione finora
- Sand Blasting Design ValidationDocumento1 paginaSand Blasting Design ValidationMvv SatyanarayanaNessuna valutazione finora
- InnovDocumento11 pagineInnovJawed AmanNessuna valutazione finora
- Communication Constable PDFDocumento1 paginaCommunication Constable PDFAjay Puri0% (1)
- Tele - Verification ReportDocumento2 pagineTele - Verification Reportvidhi09100% (1)
- Puc Certificate New 6383Documento1 paginaPuc Certificate New 6383dilip polutionNessuna valutazione finora
- Sidbi - Recruitment of Assistant Manager (Grade 'A' - General Stream) PDFDocumento2 pagineSidbi - Recruitment of Assistant Manager (Grade 'A' - General Stream) PDFManoj DasNessuna valutazione finora
- Medical Reimbursement Claim Form For Outdoor TreatmentDocumento1 paginaMedical Reimbursement Claim Form For Outdoor TreatmentHimanshu YadavNessuna valutazione finora
- ZHRF Claim OutdoorDocumento1 paginaZHRF Claim OutdoorACCOUNTS OFFICER PAY BSNL EG RAJAMAHENDRAVARAMNessuna valutazione finora
- Date:: Sl. Bill No. Date Amount Sl. Bill No. Date Amount Sl. Bill Date Amount No. No. No. NoDocumento1 paginaDate:: Sl. Bill No. Date Amount Sl. Bill No. Date Amount Sl. Bill Date Amount No. No. No. NoAKHIL C SUNNYNessuna valutazione finora
- Mediassist Claim FormDocumento5 pagineMediassist Claim FormsureshNessuna valutazione finora
- MiCare Claim FormDocumento2 pagineMiCare Claim FormPushan Punjabi100% (3)
- 4-Summary of Mediclaim Expenses - 1Documento4 pagine4-Summary of Mediclaim Expenses - 1DT worldNessuna valutazione finora
- Urine Therapy E BookDocumento2 pagineUrine Therapy E BookDT worldNessuna valutazione finora
- JD - Section Head Mechanical-2Documento3 pagineJD - Section Head Mechanical-2DT worldNessuna valutazione finora
- Urine TherapyDocumento43 pagineUrine TherapyBashu Poudel100% (3)
- Open NotificationDocumento214 pagineOpen NotificationDT worldNessuna valutazione finora
- International Business EnvironmentDocumento5 pagineInternational Business EnvironmentrahulNessuna valutazione finora
- Basics Stats Ti NspireDocumento7 pagineBasics Stats Ti NspirePanagiotis SotiropoulosNessuna valutazione finora
- Vacuum Dehydrator & Oil Purification System: A Filter Focus Technical Publication D1-14Documento1 paginaVacuum Dehydrator & Oil Purification System: A Filter Focus Technical Publication D1-14Drew LeibbrandtNessuna valutazione finora
- Tourism: The Business of Hospitality and TravelDocumento33 pagineTourism: The Business of Hospitality and TravelNajla Nabila AurelliaNessuna valutazione finora
- Germany's Three-Pillar Banking SystemDocumento7 pagineGermany's Three-Pillar Banking Systemmladen_nbNessuna valutazione finora
- Wiring DiagramsDocumento69 pagineWiring DiagramsMahdiNessuna valutazione finora
- CS506 Mid SubjectiveDocumento2 pagineCS506 Mid SubjectiveElma AlamNessuna valutazione finora
- Maths VIII FA4Documento3 pagineMaths VIII FA4BGTM 1988Nessuna valutazione finora
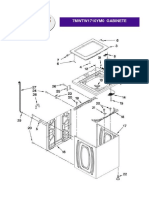
- 7MWTW1710YM0Documento8 pagine7MWTW1710YM0Izack-Dy JimZitNessuna valutazione finora
- Rajkumar Kitchen Model Oil Expeller - INRDocumento1 paginaRajkumar Kitchen Model Oil Expeller - INRNishant0% (1)
- A Study On Impact of Smartphone AddictioDocumento4 pagineA Study On Impact of Smartphone AddictiotansuoragotNessuna valutazione finora
- Guide To Networking Essentials Fifth Edition: Making Networks WorkDocumento33 pagineGuide To Networking Essentials Fifth Edition: Making Networks WorkKhamis SeifNessuna valutazione finora
- One Way Slab DesignDocumento10 pagineOne Way Slab DesignBijendra PradhanNessuna valutazione finora
- Problems of Spun Concrete Piles Constructed in Soft Soil in HCMC and Mekong Delta - VietnamDocumento6 pagineProblems of Spun Concrete Piles Constructed in Soft Soil in HCMC and Mekong Delta - VietnamThaoNessuna valutazione finora
- q2 Long Quiz 002 EntreDocumento8 pagineq2 Long Quiz 002 EntreMonn Justine Sabido0% (1)
- Section 1: 1. Ofosu, George Nelson 2. OBENG, Kevin Kofi 3.OBENG-OFORI, Afrifa KwameDocumento17 pagineSection 1: 1. Ofosu, George Nelson 2. OBENG, Kevin Kofi 3.OBENG-OFORI, Afrifa KwameTony JamesNessuna valutazione finora
- Mobile Fire Extinguishers. Characteristics, Performance and Test MethodsDocumento28 pagineMobile Fire Extinguishers. Characteristics, Performance and Test MethodsSawita LertsupochavanichNessuna valutazione finora
- CH 3 Revision Worksheet 2 Class 6 CSDocumento1 paginaCH 3 Revision Worksheet 2 Class 6 CSShreyank SinghNessuna valutazione finora
- Factors Affecting The Implementation of Green Procurement: Empirical Evidence From Indonesian Educational InstitutionDocumento12 pagineFactors Affecting The Implementation of Green Procurement: Empirical Evidence From Indonesian Educational InstitutionYeni Saro ManaluNessuna valutazione finora
- KL1508 KL1516: 8/16-Port Cat 5 High-Density Dual Rail LCD KVM SwitchDocumento5 pagineKL1508 KL1516: 8/16-Port Cat 5 High-Density Dual Rail LCD KVM SwitchnisarahmedgfecNessuna valutazione finora
- How To Make Affidavit at Pune Collector OfficeDocumento1 paginaHow To Make Affidavit at Pune Collector Officejayram1961Nessuna valutazione finora
- Setup LogDocumento221 pagineSetup LogCarlos MendezNessuna valutazione finora
- ASTM G165-99 (R2005) Standard Practice For Determining Rail-To-Earth ResistanceDocumento5 pagineASTM G165-99 (R2005) Standard Practice For Determining Rail-To-Earth Resistance曾乙申100% (1)
- Huzaima ResultDocumento2 pagineHuzaima ResultSaif Ali KhanNessuna valutazione finora
- TIP - IPBT M - E For MentorsDocumento3 pagineTIP - IPBT M - E For Mentorsallan galdianoNessuna valutazione finora
- DenmarkDocumento4 pagineDenmarkFalcon KingdomNessuna valutazione finora
- Instructions: This Affidavit Should Be Executed by The PersonDocumento1 paginaInstructions: This Affidavit Should Be Executed by The PersonspcbankingNessuna valutazione finora
- SWOT Analysis Microtel by WyndhamDocumento10 pagineSWOT Analysis Microtel by WyndhamAllyza Krizchelle Rosales BukidNessuna valutazione finora
- cv20672778 Prashanth - Sadak Operations-ManagerDocumento4 paginecv20672778 Prashanth - Sadak Operations-ManagerBhasker NiftyNessuna valutazione finora
- Computer Graphics Mini ProjectDocumento25 pagineComputer Graphics Mini ProjectGautam Singh78% (81)