Potrebbero piacerti anche
- Lab Qa QC Manual PDFDocumento152 pagineLab Qa QC Manual PDFmiguelsanchezjuNessuna valutazione finora
- Standard Operating Procedure: TitleDocumento9 pagineStandard Operating Procedure: TitleayodejidetaNessuna valutazione finora
- GPM Guideline Inspect EngDocumento96 pagineGPM Guideline Inspect EngDilawar BakhtNessuna valutazione finora
- Quality Manual. Quality Manual. Institute For Standardization and Control of Pharmaceuticals. SOP No. QM-01 - 02Documento34 pagineQuality Manual. Quality Manual. Institute For Standardization and Control of Pharmaceuticals. SOP No. QM-01 - 02Kenneth JapsonNessuna valutazione finora
- Sops IndexDocumento3 pagineSops IndexIbrahim IssaNessuna valutazione finora
- Salom Pharmacy LTD: Quality Control Laboratory SPL-SOP-QC-DISS-001 Operation of Dissolution Rate ApparatusDocumento2 pagineSalom Pharmacy LTD: Quality Control Laboratory SPL-SOP-QC-DISS-001 Operation of Dissolution Rate ApparatusPaolo Peps100% (1)
- SOP For Handling of Spillage of Solid - Liquid Media Containing Growth - Pharmaceutical GuidelinesDocumento1 paginaSOP For Handling of Spillage of Solid - Liquid Media Containing Growth - Pharmaceutical GuidelinesJose Ramon Dalo BautistaNessuna valutazione finora
- Iso 9187 1 1991Documento9 pagineIso 9187 1 1991Muhammad ImranNessuna valutazione finora
- Corrective And Preventative Action A Complete Guide - 2020 EditionDa EverandCorrective And Preventative Action A Complete Guide - 2020 EditionNessuna valutazione finora
- ORA-LAB.4.13 Record and Data Management (v02)Documento11 pagineORA-LAB.4.13 Record and Data Management (v02)Vedang BhagwatNessuna valutazione finora
- A Review On Good Distribution PracticesDocumento6 pagineA Review On Good Distribution Practicesbharath saiNessuna valutazione finora
- Quality Management System AuditDocumento14 pagineQuality Management System AuditSpectro SinghNessuna valutazione finora
- Pharmaceutical Country Profile PeruDocumento147 paginePharmaceutical Country Profile PeruNethcy JapNessuna valutazione finora
- RiskISO 17025Documento8 pagineRiskISO 17025paeg6512Nessuna valutazione finora
- Ensure Quality with GMP ComplianceDocumento78 pagineEnsure Quality with GMP ComplianceAhmad Yusrizal FaizinNessuna valutazione finora
- Quality Management Systems A Complete Guide - 2021 EditionDa EverandQuality Management Systems A Complete Guide - 2021 EditionNessuna valutazione finora
- Process Validation - DR Asmaa El-Kersh, M.SCDocumento44 pagineProcess Validation - DR Asmaa El-Kersh, M.SCTahan SibueaNessuna valutazione finora
- New Screening Tests For Fomema Medical Examination and Updated Procedures For Appeal ProcessDocumento11 pagineNew Screening Tests For Fomema Medical Examination and Updated Procedures For Appeal ProcesssyazawaniNessuna valutazione finora
- Laboratory Housekeeping: 1.0 PurposeDocumento3 pagineLaboratory Housekeeping: 1.0 PurposeAbu MuazNessuna valutazione finora
- OOSDocumento14 pagineOOSqfbfabyholaNessuna valutazione finora
- Aac 05 - Laboratory Services Are Provided As Per The Scope of The Hospital'S Services and Laboratory Safety Requirements - 1.0 PurposeDocumento6 pagineAac 05 - Laboratory Services Are Provided As Per The Scope of The Hospital'S Services and Laboratory Safety Requirements - 1.0 PurposeBhavna ThakurNessuna valutazione finora
- A2LA Expalnations For ISO 17025 RequirementsDocumento27 pagineA2LA Expalnations For ISO 17025 RequirementsgiamilliaNessuna valutazione finora
- CR007 SOP Reconciliation of SAEsDocumento5 pagineCR007 SOP Reconciliation of SAEsclinfoxNessuna valutazione finora
- FDA guide to corrective and preventive actions (CAPADocumento9 pagineFDA guide to corrective and preventive actions (CAPADiego Armando Juárez AguilarNessuna valutazione finora
- 4013 Stability TestingDocumento5 pagine4013 Stability TestingtghonsNessuna valutazione finora
- Product Formulation DevelopmentDocumento3 pagineProduct Formulation DevelopmentAnonymous mBOujo5Nessuna valutazione finora
- Microbiology-Lab Practical SOP - 10Documento2 pagineMicrobiology-Lab Practical SOP - 10Biswanath Bhunia100% (1)
- Winthrox QC checklistDocumento5 pagineWinthrox QC checklistanoushia alviNessuna valutazione finora
- Alconox Detergent Cleaning ValidationDocumento12 pagineAlconox Detergent Cleaning ValidationstanlesNessuna valutazione finora
- Meclizine HCLDocumento10 pagineMeclizine HCLChEng_Nessuna valutazione finora
- Microbiological Best Lab Practices & Environmental MonitoringDocumento26 pagineMicrobiological Best Lab Practices & Environmental MonitoringNurul Hardiyanthi SadikinNessuna valutazione finora
- Weather Folds Pharmaceutical Standard Operating Procedures Good Laboratory PracticesDocumento5 pagineWeather Folds Pharmaceutical Standard Operating Procedures Good Laboratory PracticesWeatherfolds PharmaNessuna valutazione finora
- 16.0 Re-Validation / RequalificationDocumento3 pagine16.0 Re-Validation / RequalificationBhavik YadavNessuna valutazione finora
- Standard Operating Procedure For Product Mock RecallsDocumento3 pagineStandard Operating Procedure For Product Mock RecallsSolomonNessuna valutazione finora
- Medical Device Quality Systems Manual: A Small Entity Compliance GuideDocumento468 pagineMedical Device Quality Systems Manual: A Small Entity Compliance GuideScott BeachNessuna valutazione finora
- Content: Standard Operating Procedure (SOP) Master SOP For Writing Quality Management DocumentsDocumento6 pagineContent: Standard Operating Procedure (SOP) Master SOP For Writing Quality Management DocumentsAmer RahmahNessuna valutazione finora
- Testing Procedure of Caps: Ferozsons Laboratories Limited Work InstructionsDocumento8 pagineTesting Procedure of Caps: Ferozsons Laboratories Limited Work InstructionsaKureishiNessuna valutazione finora
- The Procurement Qualification and Calibration of Lab InstrumentsDocumento7 pagineThe Procurement Qualification and Calibration of Lab InstrumentsMowaten MasryNessuna valutazione finora
- Environmental Monitoring Incubation Conditions - JustificationDocumento4 pagineEnvironmental Monitoring Incubation Conditions - Justificationveerreddy_157808Nessuna valutazione finora
- Water Quality ManualDocumento9 pagineWater Quality ManualRavii Curtis100% (1)
- Development of CCSDocumento54 pagineDevelopment of CCSDiana Oldani100% (2)
- Creation of SOP - 10Documento10 pagineCreation of SOP - 10ibrahimgomaaNessuna valutazione finora
- LAB 130 Stability Management Procedure SampleDocumento3 pagineLAB 130 Stability Management Procedure SampleOdunlamiNessuna valutazione finora
- Acusera Brochure May14 085007Documento112 pagineAcusera Brochure May14 085007SeftiyantiNessuna valutazione finora
- Pyriproxyfen Papaya Draft ProtocolDocumento16 paginePyriproxyfen Papaya Draft ProtocolprecauteNessuna valutazione finora
- Environmental monitoring of clean rooms in vaccine manufacturing facilitiesDocumento37 pagineEnvironmental monitoring of clean rooms in vaccine manufacturing facilitiesKrischaireddy AnnapureddyNessuna valutazione finora
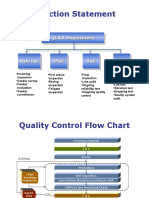
- Function Statement: QC&A DepartmentDocumento3 pagineFunction Statement: QC&A DepartmentMohamed100% (1)
- Winthrox Laboratories Pvt. LTD: Quality Assurance DepartmentDocumento2 pagineWinthrox Laboratories Pvt. LTD: Quality Assurance Departmentanoushia alviNessuna valutazione finora
- Quality Records: Neptune OrthopaedicsDocumento1 paginaQuality Records: Neptune Orthopaedicsdhir.ankurNessuna valutazione finora
- Type III DMF White Papr (1) .Rev 1 Final - Doc5!8!023Documento65 pagineType III DMF White Papr (1) .Rev 1 Final - Doc5!8!023bot38100% (2)
- Usp 601Documento33 pagineUsp 601Nur AcarNessuna valutazione finora
- Issuance of DocumentsDocumento2 pagineIssuance of DocumentsAshok KumarNessuna valutazione finora
- SOP for Handling Out of Trend Pharmaceutical ResultsDocumento3 pagineSOP for Handling Out of Trend Pharmaceutical ResultsMubarak PatelNessuna valutazione finora
- Action Plan For Quality System Improvement - 06 - 12Documento9 pagineAction Plan For Quality System Improvement - 06 - 12Parveen KumarNessuna valutazione finora
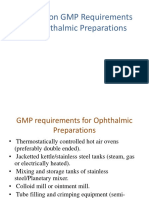
- GMP Requirements for Ophthalmic Preparations SeminarDocumento57 pagineGMP Requirements for Ophthalmic Preparations Seminarvkguptajss100% (1)
- GMP Trends-1Documento177 pagineGMP Trends-1skvemulaNessuna valutazione finora
- Issuing Date Doc No: Effective Date Department Next Review Date SectionDocumento5 pagineIssuing Date Doc No: Effective Date Department Next Review Date SectionAmer Abu RahmahNessuna valutazione finora
- Good Distribution Practices A Complete Guide - 2021 EditionDa EverandGood Distribution Practices A Complete Guide - 2021 EditionNessuna valutazione finora
- Process Approach A Complete Guide - 2019 EditionDa EverandProcess Approach A Complete Guide - 2019 EditionNessuna valutazione finora
- Good Distribution Practice A Complete Guide - 2020 EditionDa EverandGood Distribution Practice A Complete Guide - 2020 EditionNessuna valutazione finora
- Pharmacogenomic WorkshopDocumento1 paginaPharmacogenomic WorkshopRevathy GunaseelanNessuna valutazione finora
- Zoom Tutorial Update Mar 20 PDFDocumento14 pagineZoom Tutorial Update Mar 20 PDFRevathy GunaseelanNessuna valutazione finora
- Insulin (IN374S)Documento2 pagineInsulin (IN374S)Revathy GunaseelanNessuna valutazione finora
- C-Peptide ELISA Kit GuideDocumento2 pagineC-Peptide ELISA Kit GuideRevathy GunaseelanNessuna valutazione finora
- Nomination Form (Mnams) : (For Diplomate of National Board (DNB) Examination Passed Candidates)Documento4 pagineNomination Form (Mnams) : (For Diplomate of National Board (DNB) Examination Passed Candidates)Revathy GunaseelanNessuna valutazione finora
- MC ScriptDocumento3 pagineMC ScriptRevathy GunaseelanNessuna valutazione finora
- Cobas Liat User Manual SW 3 2Documento196 pagineCobas Liat User Manual SW 3 2Revathy Gunaseelan100% (1)
- Thrombocytopenia: An Update: K. J. Smock, S. L. PerkinsDocumento10 pagineThrombocytopenia: An Update: K. J. Smock, S. L. PerkinsRevathy GunaseelanNessuna valutazione finora
- NABL 160 - Guide Preparing A Quality Manual PDFDocumento61 pagineNABL 160 - Guide Preparing A Quality Manual PDFzilangamba_s453567% (3)
- MB0050 - Descriptive Practice QPDocumento3 pagineMB0050 - Descriptive Practice QPAbdul Lateef Khan100% (1)
- Camera CalibrationDocumento11 pagineCamera CalibrationFabien MairesseNessuna valutazione finora
- Keys to Maintaining Pressure Equipment IntegrityDocumento22 pagineKeys to Maintaining Pressure Equipment IntegrityNabil Al-KhirdajiNessuna valutazione finora
- Student Research Report on Walls Company ProductsDocumento3 pagineStudent Research Report on Walls Company ProductsTalha Khalid100% (1)
- Effectiveness of Product Packaging On Customer Patronage of Bournvita in Ekiti State PDFDocumento14 pagineEffectiveness of Product Packaging On Customer Patronage of Bournvita in Ekiti State PDFRahul ThampiNessuna valutazione finora
- Tourists' Spatial Behavior in Urban DestinationsDocumento14 pagineTourists' Spatial Behavior in Urban DestinationsMaria Cristina GiugăNessuna valutazione finora
- JournalDocumento81 pagineJournalDinataNusantaraChandraNessuna valutazione finora
- PWC Conflict Minerals Compliance ProcessDocumento8 paginePWC Conflict Minerals Compliance ProcessJustformedia JustformediaNessuna valutazione finora
- Sharma (2018) Developing and Validating An Instrument For Measuring Online Service Quality in The Tourism SectorDocumento34 pagineSharma (2018) Developing and Validating An Instrument For Measuring Online Service Quality in The Tourism SectorArunNessuna valutazione finora
- Sle Proposal FormDocumento3 pagineSle Proposal Formapi-445367900Nessuna valutazione finora
- Evaluating HRD ProgrammesDocumento46 pagineEvaluating HRD ProgrammesAchmad PriyaniNessuna valutazione finora
- Exploration of Placer Gold Deposits by Geomagnetic Surveys PDFDocumento9 pagineExploration of Placer Gold Deposits by Geomagnetic Surveys PDFAulia Kurnia HadyNessuna valutazione finora
- Research MethodDocumento7 pagineResearch MethodNasrumih NasirNessuna valutazione finora
- Chap006 MKTG StrategyDocumento18 pagineChap006 MKTG Strategybhar4tpNessuna valutazione finora
- Impact of Wages On Employee ProductivityDocumento2 pagineImpact of Wages On Employee ProductivityAlelei BungalanNessuna valutazione finora
- What Is The Delphi Method?Documento2 pagineWhat Is The Delphi Method?Dunia Miqdad100% (1)
- Journal of Environmental ManagementDocumento13 pagineJournal of Environmental ManagementAndreamNessuna valutazione finora
- 3 IDocumento11 pagine3 ICris Fredrich AndalizaNessuna valutazione finora
- QA QC WeldingDocumento11 pagineQA QC Weldinghareesh13h100% (1)
- Gadget Level Dependence of Children Age 3-6 Years Invillage Cranggang Dawe KudusDocumento8 pagineGadget Level Dependence of Children Age 3-6 Years Invillage Cranggang Dawe Kudusvera zulfiNessuna valutazione finora
- Evolution of Business Policy and StrategyDocumento33 pagineEvolution of Business Policy and StrategyKarlayaanNessuna valutazione finora
- EthnographyDocumento22 pagineEthnographyJoe Marflo FloresNessuna valutazione finora
- SOC Board StatementDocumento1 paginaSOC Board StatementEllma ShaffinaNessuna valutazione finora
- Discrete Choice Experiments Are Not Conjoint Analysis: Jordan J Louviere Terry N Flynn Richard T CarsonDocumento16 pagineDiscrete Choice Experiments Are Not Conjoint Analysis: Jordan J Louviere Terry N Flynn Richard T CarsonYaronBabaNessuna valutazione finora
- Development and Validation of Financial Literacy Test Among Filipino LearnersDocumento7 pagineDevelopment and Validation of Financial Literacy Test Among Filipino LearnersAsh AlbaniaNessuna valutazione finora
- Practical Research 2: (With Learning Activity Sheets) Quantitative Research For Senior High SchoolDocumento54 paginePractical Research 2: (With Learning Activity Sheets) Quantitative Research For Senior High SchoolRodelyn Ramos GonzalesNessuna valutazione finora
- Research Paper Scope and Limitations SampleDocumento7 pagineResearch Paper Scope and Limitations Sampleukldyebkf100% (1)
- Abdulrahman Dhabaan - (OB Final Project)Documento49 pagineAbdulrahman Dhabaan - (OB Final Project)Abdulrahman DhabaanNessuna valutazione finora
- Effectiveness of Performance Appraisal System in PRILDocumento67 pagineEffectiveness of Performance Appraisal System in PRILgeorgecool_2006100% (1)