Potrebbero piacerti anche
- LM Precal Grade11 Sem 1Documento296 pagineLM Precal Grade11 Sem 1dnnlmrchngcnn91% (35)
- Indiana State Department of Health Certificate of DeathDocumento1 paginaIndiana State Department of Health Certificate of Deathkiny100% (1)
- McWilliams, Peter - You Can't Afford The Luxury of A Negative ThoughtDocumento42 pagineMcWilliams, Peter - You Can't Afford The Luxury of A Negative Thoughtniolus100% (3)
- Traumatic Brain Injury GuidelinesDocumento108 pagineTraumatic Brain Injury GuidelinesMu Z100% (1)
- Airedale N.H.S v. Bland 1993 (Basis of Auna) - DasvDocumento29 pagineAiredale N.H.S v. Bland 1993 (Basis of Auna) - DasvNiten ChopraNessuna valutazione finora
- Study Protocol (Trauma)Documento17 pagineStudy Protocol (Trauma)Ardy Antonio MDNessuna valutazione finora
- Legal and Ethical Aspects of Critical Care NursingDocumento66 pagineLegal and Ethical Aspects of Critical Care NursingJamille Abenir Lopez100% (2)
- The Art of Conversation Through Serious Illness-Lessons For Caregivers-Richard P. McquellonDocumento161 pagineThe Art of Conversation Through Serious Illness-Lessons For Caregivers-Richard P. McquellonTRAN NGOCNessuna valutazione finora
- Forensic Autopsy: DR Frank Kakuba GDocumento28 pagineForensic Autopsy: DR Frank Kakuba GMwanja MosesNessuna valutazione finora
- DeathDocumento42 pagineDeathEunice ChavezNessuna valutazione finora
- Ortho Final 2Documento18 pagineOrtho Final 2Nadine BenitoNessuna valutazione finora
- Four Chapter ThesisDocumento20 pagineFour Chapter ThesisEspi Marian100% (4)
- The Views of Orthodox Theology On Bioethical IssuesDocumento24 pagineThe Views of Orthodox Theology On Bioethical IssuessilviustoiangalatiNessuna valutazione finora
- Human Person Towards Impending Death: Introduction To The Philosophy of The Human PersonDocumento45 pagineHuman Person Towards Impending Death: Introduction To The Philosophy of The Human PersonRaniel John SampianoNessuna valutazione finora
- 2021 Lancet Community-Acquired PneumoniaDocumento14 pagine2021 Lancet Community-Acquired PneumoniaCarlos Del Valle JaureguiNessuna valutazione finora
- Legal Medicine and Medical JurisprudenceDocumento47 pagineLegal Medicine and Medical Jurisprudencet7uyuytuNessuna valutazione finora
- Advance Trauma Center-Quezon City PartDocumento10 pagineAdvance Trauma Center-Quezon City PartLeslie Dela TorreNessuna valutazione finora
- Research ToolDocumento15 pagineResearch Toolmayur.polNessuna valutazione finora
- JournalDocumento6 pagineJournalnaelarizqiNessuna valutazione finora
- CRITIQUE REVIEW (New)Documento6 pagineCRITIQUE REVIEW (New)Anita De GuzmanNessuna valutazione finora
- Schmidt2020 Article SynergisticEffectsOfForensicMeDocumento12 pagineSchmidt2020 Article SynergisticEffectsOfForensicMeLanny Dwi ChandraNessuna valutazione finora
- 1753-Article Text-39640-3-10-20220815Documento9 pagine1753-Article Text-39640-3-10-20220815Inah SaritaNessuna valutazione finora
- CRITIQUE REVIEW (New)Documento7 pagineCRITIQUE REVIEW (New)Anita De GuzmanNessuna valutazione finora
- Chapter 1Documento10 pagineChapter 1Leslie Dela TorreNessuna valutazione finora
- Predictors of Falls and Mortality Among Elderly Adults With Traumatic Brain Injury: A Nationwide, Population-Based StudyDocumento15 paginePredictors of Falls and Mortality Among Elderly Adults With Traumatic Brain Injury: A Nationwide, Population-Based Studywulan anugerah sariNessuna valutazione finora
- Bomb Blast Injuries: An Exploration of Patient Characteristics and Outcome Using Pakistan National Emergency Departments Surveillance (Pak-NEDS) DataDocumento5 pagineBomb Blast Injuries: An Exploration of Patient Characteristics and Outcome Using Pakistan National Emergency Departments Surveillance (Pak-NEDS) DataWildan DzakiyNessuna valutazione finora
- Prevalence and Correlates of Post-Traumatic Stress Disorder Among Survivors of Road Traffic Accidents in EthiopiaDocumento8 paginePrevalence and Correlates of Post-Traumatic Stress Disorder Among Survivors of Road Traffic Accidents in EthiopiaAsri PutriNessuna valutazione finora
- 424-Article Text-1618-1-10-20191115 PDFDocumento6 pagine424-Article Text-1618-1-10-20191115 PDFhaechan's fluffy bucket hatNessuna valutazione finora
- JCM 10 00797Documento11 pagineJCM 10 00797alazarNessuna valutazione finora
- Pressure UlcerDocumento5 paginePressure Ulcerifi medanNessuna valutazione finora
- Prehospital Guidelines For The Management of Traumatic Brain Injury - 3rd EditionDocumento32 paginePrehospital Guidelines For The Management of Traumatic Brain Injury - 3rd EditionPeyepeyeNessuna valutazione finora
- Duronjic Et Al. 2020 IMPACT OF LANGUAGE BARRIERS AND INTERPRETER REQUIREMENTDocumento2 pagineDuronjic Et Al. 2020 IMPACT OF LANGUAGE BARRIERS AND INTERPRETER REQUIREMENTLUIS ENRIQUE CALDERON GUERRERONessuna valutazione finora
- Global Action On Patient SafetyDocumento8 pagineGlobal Action On Patient SafetycynthiaNessuna valutazione finora
- Epidemiology of Traumatic Brain Injury in Eastern ChinaDocumento7 pagineEpidemiology of Traumatic Brain Injury in Eastern ChinaAdrianah OlyNessuna valutazione finora
- Multicentrico Trauma PediatricoDocumento7 pagineMulticentrico Trauma PediatricodamonenNessuna valutazione finora
- Survival Analysis and Mortality Predictors of Hospitalized Severe Burn Victims in A Malaysian Burns Intensive Care UnitDocumento8 pagineSurvival Analysis and Mortality Predictors of Hospitalized Severe Burn Victims in A Malaysian Burns Intensive Care UnitKenjiNessuna valutazione finora
- WFCCN Chapter 4 Safety-and-Quality-in-the-ICU 2nd EditionDocumento13 pagineWFCCN Chapter 4 Safety-and-Quality-in-the-ICU 2nd EditionJuan Carlos Mora TorresNessuna valutazione finora
- World Journal of Emergency Surgery: Preventable Trauma Deaths: From Panel Review To Population Based-StudiesDocumento7 pagineWorld Journal of Emergency Surgery: Preventable Trauma Deaths: From Panel Review To Population Based-StudiesRita RangelNessuna valutazione finora
- s12245 020 0266 3Documento5 pagines12245 020 0266 3chenth3r3Nessuna valutazione finora
- Jurnal Inter 1Documento10 pagineJurnal Inter 1Adhe YuniarNessuna valutazione finora
- Health Professionals of Emergency Service: Evaluation of Triage and Ethical Values in Disaster MedicineDocumento6 pagineHealth Professionals of Emergency Service: Evaluation of Triage and Ethical Values in Disaster MedicinetarsiahningsihNessuna valutazione finora
- Paguio Final TopicDocumento93 paginePaguio Final TopicGie UngonNessuna valutazione finora
- Non Thesis ProjectDocumento44 pagineNon Thesis Projectapi-285177380Nessuna valutazione finora
- Falls Prevention in Hospitals-The Need For A New Approach An Integrative ArticleDocumento4 pagineFalls Prevention in Hospitals-The Need For A New Approach An Integrative ArticleDwi NopriyantoNessuna valutazione finora
- 2019 Enf Transm SexualDocumento6 pagine2019 Enf Transm Sexualakihiki gonzalezNessuna valutazione finora
- Title Prevalence of Infections in Residential Care Homes (Rches) For The Elderly in Hong KongDocumento39 pagineTitle Prevalence of Infections in Residential Care Homes (Rches) For The Elderly in Hong KongHam FGNessuna valutazione finora
- Artikel 2Documento20 pagineArtikel 2rimafitrianiNessuna valutazione finora
- PSSJN - Volume 8 - Issue 3 - Pages 68-83Documento16 paginePSSJN - Volume 8 - Issue 3 - Pages 68-83Smith MpNessuna valutazione finora
- NILES-Volume 4-Issue 2 - Page 301-317Documento17 pagineNILES-Volume 4-Issue 2 - Page 301-317Maged SaadNessuna valutazione finora
- Profile of Nasopharyngeal Carcinoma in Dr. Cipto Mangunkusumo National Hospital, 2010Documento7 pagineProfile of Nasopharyngeal Carcinoma in Dr. Cipto Mangunkusumo National Hospital, 2010Aziddin Gani HarahapNessuna valutazione finora
- 2.abstract Book - BMMC 2011Documento199 pagine2.abstract Book - BMMC 2011Dragos CalinNessuna valutazione finora
- Multi-State Modelling of Heart Failure Care Path: A Population-Based Investigation From ItalyDocumento15 pagineMulti-State Modelling of Heart Failure Care Path: A Population-Based Investigation From ItalymarinatariganNessuna valutazione finora
- The Problem and Its Background 1.1Documento17 pagineThe Problem and Its Background 1.1At Sa Wakas AyNessuna valutazione finora
- HHS Public Access: Chest Trauma Outcomes: Public Versus Private Level I Trauma CentersDocumento19 pagineHHS Public Access: Chest Trauma Outcomes: Public Versus Private Level I Trauma CentersIthaNessuna valutazione finora
- Analysis of Mortality in PICU of A Tertiary Care Teaching Hospital, Telangana - An IntrospectionDocumento29 pagineAnalysis of Mortality in PICU of A Tertiary Care Teaching Hospital, Telangana - An IntrospectionRusmila UlfahNessuna valutazione finora
- Kaidt 2Documento17 pagineKaidt 2الرشيد النووورNessuna valutazione finora
- Elsherbiny 2017Documento8 pagineElsherbiny 2017Siti ChodijahNessuna valutazione finora
- A Survey of The Burden of Management of Chronic Suppurative Otitis Media in A Developing CountryDocumento15 pagineA Survey of The Burden of Management of Chronic Suppurative Otitis Media in A Developing CountryharryNessuna valutazione finora
- Oral Cancer: The First Symptoms and Reasons For Delaying Correct Diagnosis and Appropriate TreatmentDocumento9 pagineOral Cancer: The First Symptoms and Reasons For Delaying Correct Diagnosis and Appropriate TreatmentMarekNessuna valutazione finora
- 24 PrabaDocumento9 pagine24 PrabaAbdul GhofurNessuna valutazione finora
- (Kuali) 20568-39344-1-PBDocumento7 pagine(Kuali) 20568-39344-1-PBJoseph BennettNessuna valutazione finora
- 2022 Article 795Documento8 pagine2022 Article 795Juan David Hernández CifuentesNessuna valutazione finora
- Coba PrintttDocumento8 pagineCoba PrintttNunungNessuna valutazione finora
- Epidemiology and Outcomes of Burn Injuries at A Tertiary Burn Care Center in BangladeshDocumento7 pagineEpidemiology and Outcomes of Burn Injuries at A Tertiary Burn Care Center in BangladeshE.sundara BharathiNessuna valutazione finora
- Epidemiology and Changes in Mortality of Sepsis After The Implementation of Surviving Sepsis Campaign GuidelinesDocumento11 pagineEpidemiology and Changes in Mortality of Sepsis After The Implementation of Surviving Sepsis Campaign Guidelinesfaraz.mirza1Nessuna valutazione finora
- Global Prevelance of SCI 2014Documento23 pagineGlobal Prevelance of SCI 2014M.A. Ch.Nessuna valutazione finora
- Supportive Care Needs of Patients With Head and Neck Cancer Referred To Palliative MedicineDocumento8 pagineSupportive Care Needs of Patients With Head and Neck Cancer Referred To Palliative Medicinemadhumitha srinivasNessuna valutazione finora
- 2019 Golden Hour and The Management of Polytrauma. The Experience of Salento's Up-And-Coming Trauma Center PDFDocumento5 pagine2019 Golden Hour and The Management of Polytrauma. The Experience of Salento's Up-And-Coming Trauma Center PDFAndresPinedaMNessuna valutazione finora
- The Opioid Epidemic and the Therapeutic Community Model: An Essential GuideDa EverandThe Opioid Epidemic and the Therapeutic Community Model: An Essential GuideJonathan D. AveryNessuna valutazione finora
- Read Me - Fonts LinksDocumento1 paginaRead Me - Fonts LinkswegoupNessuna valutazione finora
- 123 Quartiles (Data)Documento2 pagine123 Quartiles (Data)wegoupNessuna valutazione finora
- Fix Format PPT Pra PkpaDocumento15 pagineFix Format PPT Pra PkpanuraninarunNessuna valutazione finora
- 123 Quartile MathsearchDocumento2 pagine123 Quartile MathsearchwegoupNessuna valutazione finora
- Spark Free PresentationDocumento10 pagineSpark Free PresentationwegoupNessuna valutazione finora
- Fix Format PPT Pra PkpaDocumento15 pagineFix Format PPT Pra PkpanuraninarunNessuna valutazione finora
- 1A Student Checklist Research Plan Instructions PDFDocumento2 pagine1A Student Checklist Research Plan Instructions PDFFrancisca CassandraNessuna valutazione finora
- Read Me - Fonts LinksDocumento1 paginaRead Me - Fonts LinkswegoupNessuna valutazione finora
- Spark Free PresentationDocumento10 pagineSpark Free PresentationwegoupNessuna valutazione finora
- 1A Student Checklist Research Plan Instructions PDFDocumento2 pagine1A Student Checklist Research Plan Instructions PDFFrancisca CassandraNessuna valutazione finora
- For CostumeDocumento1 paginaFor CostumewegoupNessuna valutazione finora
- XSTAT - United States - RevMedx, Inc - PDFDocumento2 pagineXSTAT - United States - RevMedx, Inc - PDFwegoupNessuna valutazione finora
- XSTAT - United States - RevMedx, Inc - PDFDocumento2 pagineXSTAT - United States - RevMedx, Inc - PDFwegoupNessuna valutazione finora
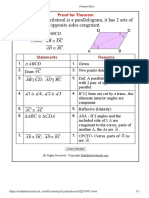
- Theorems Dealing With Parallelograms - MathBitsNotebook (Geo - CCSS Math)Documento2 pagineTheorems Dealing With Parallelograms - MathBitsNotebook (Geo - CCSS Math)wegoupNessuna valutazione finora
- Answer Box PDFDocumento1 paginaAnswer Box PDFwegoupNessuna valutazione finora
- Answer Box PDFDocumento1 paginaAnswer Box PDFwegoupNessuna valutazione finora
- 1111Documento1 pagina1111wegoupNessuna valutazione finora
- For UploadDocumento2 pagineFor UploadwegoupNessuna valutazione finora
- For CostumeDocumento4 pagineFor CostumewegoupNessuna valutazione finora
- For CostumeDocumento1 paginaFor CostumewegoupNessuna valutazione finora
- Vaccine Exemption Religious Side Supporting DocumentDocumento14 pagineVaccine Exemption Religious Side Supporting DocumentAshish100% (3)
- 3Documento82 pagine3Hadjiyusoph Azis0% (1)
- God's Generals Do Not Fear DeathDocumento6 pagineGod's Generals Do Not Fear DeathCLOVIS J. MBEUKANessuna valutazione finora
- The Anthropology of Death RevisitedDocumento20 pagineThe Anthropology of Death RevisitedNatalia MaggiNessuna valutazione finora
- Analysis of Allen Poe's Death Theme in His Short Stories: Lin XiaobinDocumento3 pagineAnalysis of Allen Poe's Death Theme in His Short Stories: Lin XiaobinkuhsdfNessuna valutazione finora
- How Shradh OriginateDocumento4 pagineHow Shradh Originaterealindiaproperty100% (1)
- Themedicolegaldeathinvestigatoranevolutionincr PDFDocumento15 pagineThemedicolegaldeathinvestigatoranevolutionincr PDFatjoerossNessuna valutazione finora
- Guia Prático de Audiovisual 3º Ed - English VersionDocumento47 pagineGuia Prático de Audiovisual 3º Ed - English VersionLuiz Fernando da SilvaNessuna valutazione finora
- Sas7 Death and MeaningDocumento4 pagineSas7 Death and MeaningRj ArenasNessuna valutazione finora
- 9b) Medical Complications of Drug TakingDocumento19 pagine9b) Medical Complications of Drug TakingDr. Zirwa AsimNessuna valutazione finora
- I R: Why Cows Die in US Dairy Herds: Nvited EviewDocumento10 pagineI R: Why Cows Die in US Dairy Herds: Nvited EviewArshad IslamNessuna valutazione finora
- ConX 1.0 Cell Support CompilationDocumento74 pagineConX 1.0 Cell Support CompilationalthegelNessuna valutazione finora
- Book - Ronda Chervin - Weeping With Jesus The Journey From Grief To HopeDocumento90 pagineBook - Ronda Chervin - Weeping With Jesus The Journey From Grief To HopeEma C.Nessuna valutazione finora
- Organ Donation: From Diagnosis To Transplant: ReviewDocumento10 pagineOrgan Donation: From Diagnosis To Transplant: ReviewFIA SlotNessuna valutazione finora
- Coping With Loss, Grieving and DeathDocumento17 pagineCoping With Loss, Grieving and DeathElija Leigh MauricioNessuna valutazione finora
- Travis Oakes Fatality Inquiry ReportDocumento10 pagineTravis Oakes Fatality Inquiry ReportcalcitydeskNessuna valutazione finora
- Peace TitleDocumento2 paginePeace TitleJanayitri MandalNessuna valutazione finora
- Radiobiology 5Documento31 pagineRadiobiology 5joaNessuna valutazione finora
- Philosophy Module Week 7 (Revised)Documento6 paginePhilosophy Module Week 7 (Revised)Mireia MinatozakiNessuna valutazione finora
- Taboo ThesisDocumento8 pagineTaboo ThesisClaudia Acosta100% (2)