Potrebbero piacerti anche
- Pediatric Supracondylar Fractures of The Distal Humerus: Provided by Springer - Publisher ConnectorDocumento7 paginePediatric Supracondylar Fractures of The Distal Humerus: Provided by Springer - Publisher ConnectorBison_sonNessuna valutazione finora
- Lesiones Deportivas de CodoDocumento11 pagineLesiones Deportivas de CodomalacatonchiNessuna valutazione finora
- Myers - Hamstring InjuriesDocumento11 pagineMyers - Hamstring InjuriesBéla TóthNessuna valutazione finora
- Muscular Calf Injuries in RunnersDocumento5 pagineMuscular Calf Injuries in RunnersDaniel Damacena FisioterapiaNessuna valutazione finora
- Swimmer 'S Shoulder: Painful Shoulder in The Competitive SwimmerDocumento10 pagineSwimmer 'S Shoulder: Painful Shoulder in The Competitive SwimmerGerardo EsäuNessuna valutazione finora
- 4 Imaging Review of Groin Pain in Elite Athletes An Anatomic Approach To Imaging Findings 3214658300Documento11 pagine4 Imaging Review of Groin Pain in Elite Athletes An Anatomic Approach To Imaging Findings 3214658300César ArveláezNessuna valutazione finora
- Stress Reaction and Fractures - StatPearls - NCBI BookshelfDocumento6 pagineStress Reaction and Fractures - StatPearls - NCBI BookshelfAlejandro OrduzNessuna valutazione finora
- Acute Elbow Dislocations: Mechanisms, Classification, Associated InjuriesDocumento7 pagineAcute Elbow Dislocations: Mechanisms, Classification, Associated Injuriesharpreet singhNessuna valutazione finora
- Acromioclavicular Joint Injuries: Diagnosis, Classification and Ligamentoplasty ProceduresDocumento8 pagineAcromioclavicular Joint Injuries: Diagnosis, Classification and Ligamentoplasty ProceduresMiguel Angel Lamas RamirezNessuna valutazione finora
- Traumatic Hip Dislocation: A ReviewDocumento6 pagineTraumatic Hip Dislocation: A ReviewAna HurtadoNessuna valutazione finora
- Nirula Mayberry 2010 Article Commentary Rib Fracture Fixation Controversies and Technical ChallengesDocumento10 pagineNirula Mayberry 2010 Article Commentary Rib Fracture Fixation Controversies and Technical ChallengesToàn NguyễnNessuna valutazione finora
- Pediatric Stress Fractures: A Pictorial Essay: 138 The Iowa Orthopedic JournalDocumento9 paginePediatric Stress Fractures: A Pictorial Essay: 138 The Iowa Orthopedic JournalAlejandro OrduzNessuna valutazione finora
- Shoulder ConditionsDocumento8 pagineShoulder ConditionsCarlos GonzalesNessuna valutazione finora
- Airway Management in Cervical Spine Injury 2017Documento7 pagineAirway Management in Cervical Spine Injury 2017SeveNNessuna valutazione finora
- Cools 2008 Screening The Athletes Shoulder ForDocumento9 pagineCools 2008 Screening The Athletes Shoulder ForLucyFloresNessuna valutazione finora
- Scapulothoracic Dissociation: Trauma UpdateDocumento5 pagineScapulothoracic Dissociation: Trauma UpdateFadlu ManafNessuna valutazione finora
- Aaos 2019Documento283 pagineAaos 2019alealer2708Nessuna valutazione finora
- Hip Dislocation: Current Treatment Regimens: Paul Tornetta III, MD, and Hamid R. Mostafavi, MDDocumento10 pagineHip Dislocation: Current Treatment Regimens: Paul Tornetta III, MD, and Hamid R. Mostafavi, MDJaime Anaya Sierra100% (1)
- BR J Sports Med 2005 Petersen 319 23Documento6 pagineBR J Sports Med 2005 Petersen 319 23harryNessuna valutazione finora
- Axillary Nerve Palsy and Deltoid Muscle AtonyDocumento12 pagineAxillary Nerve Palsy and Deltoid Muscle AtonyLaura CandussiNessuna valutazione finora
- TendinopatíaDocumento13 pagineTendinopatíaANGELICA BARRAZA ALVARADONessuna valutazione finora
- Pectoralis Major RuptureDocumento5 paginePectoralis Major RupturezakNessuna valutazione finora
- Neuropatia PerifericaDocumento11 pagineNeuropatia PerifericaJose Alejandro Bedoya SanchezNessuna valutazione finora
- Common Pediatric Elbow Fractures: Erin S. Hart Allison Turner Maurice Albright Brian E. GrottkauDocumento7 pagineCommon Pediatric Elbow Fractures: Erin S. Hart Allison Turner Maurice Albright Brian E. GrottkauFino SopianNessuna valutazione finora
- (ACC) Repetitive Microtrauma in Glenohumeral Joint During Sports Activities On AthleteDocumento10 pagine(ACC) Repetitive Microtrauma in Glenohumeral Joint During Sports Activities On AthleteputriNessuna valutazione finora
- Literature Review A. Close Fracture Regio Clavicula Medical Concept 1. DefinitionDocumento3 pagineLiterature Review A. Close Fracture Regio Clavicula Medical Concept 1. DefinitionNidia Achirul tamaraNessuna valutazione finora
- Epidemiology of Injuries and Prevention Strategies in Competitive SwimmersDocumento6 pagineEpidemiology of Injuries and Prevention Strategies in Competitive SwimmersJhonnyNogueraNessuna valutazione finora
- The Acumoxa Treatment of Shoulder Impingement SyndromeDocumento8 pagineThe Acumoxa Treatment of Shoulder Impingement SyndromeAngela PagliusoNessuna valutazione finora
- Axillary-Nerve-PalsyDocumento11 pagineAxillary-Nerve-Palsyksaurabh027Nessuna valutazione finora
- Diare AnakDocumento6 pagineDiare AnakVictoria HusadaniNessuna valutazione finora
- Regeneration of Injured Skeletal Muscle After The Injury: Review ArticleDocumento9 pagineRegeneration of Injured Skeletal Muscle After The Injury: Review ArticleSahira Rivera DroguettNessuna valutazione finora
- Applied biomechanics of swimming and injury prevention in competitive swimmersDocumento19 pagineApplied biomechanics of swimming and injury prevention in competitive swimmersBart Merkelbach100% (1)
- STM MCQDocumento4 pagineSTM MCQapi-233655790Nessuna valutazione finora
- The Management of Flail Chest: Brian L. Pettiford, MD, James D. Luketich, MD, Rodney J. Landreneau, MDDocumento9 pagineThe Management of Flail Chest: Brian L. Pettiford, MD, James D. Luketich, MD, Rodney J. Landreneau, MDVan Irish VentilacionNessuna valutazione finora
- Impingement Syndromes of The Ankle and Hindfoot: ProtocolsDocumento11 pagineImpingement Syndromes of The Ankle and Hindfoot: Protocolsmarioma07Nessuna valutazione finora
- ORIG Garrett1996 Muscle Strain InjuriesDocumento8 pagineORIG Garrett1996 Muscle Strain InjuriesAlejandra Botero EscobarNessuna valutazione finora
- Pre-Hospital Spinal Immobilisation - An Initial Consensus StatementDocumento4 paginePre-Hospital Spinal Immobilisation - An Initial Consensus StatementJade OttoniNessuna valutazione finora
- Guideline Reino Unido - Pre-Hospital Spinal Immobilisation, An Initial Consensus StatementDocumento4 pagineGuideline Reino Unido - Pre-Hospital Spinal Immobilisation, An Initial Consensus StatementTriz BeaNessuna valutazione finora
- FractureDocumento16 pagineFractureGenevieve LawrenceNessuna valutazione finora
- Ankle Sprains: Evaluation, Rehabilitation, and Prevention: Raining Revention AND EhabilitationDocumento7 pagineAnkle Sprains: Evaluation, Rehabilitation, and Prevention: Raining Revention AND EhabilitationtanyasisNessuna valutazione finora
- All ExhibitsDocumento16 pagineAll ExhibitsJuwel KobirNessuna valutazione finora
- Femoral Neck FractureDocumento19 pagineFemoral Neck FractureTabita P SNessuna valutazione finora
- Disorders of The Sternoclavicular Joint: SoulderDocumento14 pagineDisorders of The Sternoclavicular Joint: SoulderFillipe AgraNessuna valutazione finora
- Lower Limb InjuriesDocumento47 pagineLower Limb InjuriesDaisyyhyNessuna valutazione finora
- Harper 1982Documento4 pagineHarper 1982Sri MahadhanaNessuna valutazione finora
- Understanding Intertrochanteric Fractures of the FemurDocumento12 pagineUnderstanding Intertrochanteric Fractures of the FemurEinz Nur Amalyah IdrusNessuna valutazione finora
- Sports and Performing Arts Medicine. 3.Documento8 pagineSports and Performing Arts Medicine. 3.Atlas FizyoterapiNessuna valutazione finora
- Pathology Mechanism: Jefferson Fracture Is The Eponymous Name Given To A Burst Fracture ofDocumento25 paginePathology Mechanism: Jefferson Fracture Is The Eponymous Name Given To A Burst Fracture ofAtikah FairuzNessuna valutazione finora
- Current Perspectives On Elbow Dislocation and InstabilityDocumento15 pagineCurrent Perspectives On Elbow Dislocation and InstabilityAnonymous L9D1I7DZNessuna valutazione finora
- Brachial Distal Biceps Injuries: The Physician and SportsmedicineDocumento6 pagineBrachial Distal Biceps Injuries: The Physician and SportsmedicinedanielquingaalexNessuna valutazione finora
- Trauma C1 C2Documento8 pagineTrauma C1 C2Karen OrtizNessuna valutazione finora
- 76040138-Referat-Fraktur-Pelvis EditDocumento34 pagine76040138-Referat-Fraktur-Pelvis Editsri wulanNessuna valutazione finora
- Adult Traumatic Brachial Plexus InjuriesDocumento15 pagineAdult Traumatic Brachial Plexus Injuriesapi-241264935Nessuna valutazione finora
- Cervical Spine InjuriesDocumento11 pagineCervical Spine InjuriesPrakarsa Adi Daya NusantaraNessuna valutazione finora
- Distal Triceps RupturesDocumento5 pagineDistal Triceps RupturesEllan Giulianno FerreiraNessuna valutazione finora
- Savetamal 2008Documento10 pagineSavetamal 2008Eriekafebriayana RNessuna valutazione finora
- In Practice 2012 Moores 22 6Documento6 pagineIn Practice 2012 Moores 22 6ransinghNessuna valutazione finora
- Electrophysiology of SleepDocumento1 paginaElectrophysiology of Sleeplita34Nessuna valutazione finora
- Ballen Ocular Chemical Injury PDFDocumento1 paginaBallen Ocular Chemical Injury PDFlita34Nessuna valutazione finora
- First Month Chinese 2020Documento1 paginaFirst Month Chinese 2020lita34Nessuna valutazione finora
- Kaplan Sadock Gangguan TdiurDocumento3 pagineKaplan Sadock Gangguan Tdiurlita34Nessuna valutazione finora
- Tabel 3 Chemical Ocular Injury and Their Management (Paul Singh Et Al)Documento1 paginaTabel 3 Chemical Ocular Injury and Their Management (Paul Singh Et Al)lita34Nessuna valutazione finora
- Blood Clotting FactorsDocumento1 paginaBlood Clotting Factorslita34Nessuna valutazione finora
- Delays in PneumoniaDocumento11 pagineDelays in Pneumonialita34Nessuna valutazione finora
- Brain Stem Reticular FormationDocumento6 pagineBrain Stem Reticular Formationlita34Nessuna valutazione finora
- Scanned by CamscannerDocumento9 pagineScanned by Camscannerlita34Nessuna valutazione finora
- The CochleaDocumento1 paginaThe Cochlealita34Nessuna valutazione finora
- Confident Cooking Broiling GuidelinesDocumento1 paginaConfident Cooking Broiling Guidelineslita34Nessuna valutazione finora
- Etiology of Infectious Encephalitis 3Documento1 paginaEtiology of Infectious Encephalitis 3lita34Nessuna valutazione finora
- Blood Clotting 1Documento1 paginaBlood Clotting 1lita34Nessuna valutazione finora
- Criteria Ocular Chemical Injury PDFDocumento1 paginaCriteria Ocular Chemical Injury PDFlita34Nessuna valutazione finora
- Recommendation UtiDocumento1 paginaRecommendation Utilita34Nessuna valutazione finora
- Therapy CystitisDocumento1 paginaTherapy Cystitislita34Nessuna valutazione finora
- Kurva TB BB 2-20 TahunDocumento1 paginaKurva TB BB 2-20 Tahundibo_malmsteenNessuna valutazione finora
- UTI TreatmentDocumento1 paginaUTI Treatmentlita34Nessuna valutazione finora
- Percentile BB - U Dan TB - U PDFDocumento1 paginaPercentile BB - U Dan TB - U PDFQonita NahdiyahNessuna valutazione finora
- Etiology of Infectious Encephalitis 1Documento1 paginaEtiology of Infectious Encephalitis 1lita34Nessuna valutazione finora
- Etiology of Infectious Encephalitis 2Documento1 paginaEtiology of Infectious Encephalitis 2lita34Nessuna valutazione finora
- Dka 1Documento1 paginaDka 1lita34Nessuna valutazione finora
- Hepatoma StagingDocumento1 paginaHepatoma Staginglita34Nessuna valutazione finora
- Muscular System OverviewDocumento10 pagineMuscular System OverviewKevin Yul Ancheta100% (1)
- Muscles of The FootDocumento14 pagineMuscles of The FootZaid AbdulqadirNessuna valutazione finora
- Anatomy of the Forearm and HandDocumento12 pagineAnatomy of the Forearm and HandRegina GambayanNessuna valutazione finora
- Anatomi Kinesiologi Pergelangan Kaki Dan KakiDocumento38 pagineAnatomi Kinesiologi Pergelangan Kaki Dan KakiGhea Putri HendrianiNessuna valutazione finora
- Sample FlipchartDocumento2 pagineSample FlipchartJoão RodriguesNessuna valutazione finora
- Mastering Muscles & Movement of the Axial SkeletonDocumento1 paginaMastering Muscles & Movement of the Axial Skeletonjmccoy26Nessuna valutazione finora
- The Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingDocumento13 pagineThe Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingMikeunoeNessuna valutazione finora
- Kinesio TapingDocumento62 pagineKinesio TapingDiah Rahmat100% (1)
- Ankle Joint: Types, Capsule, Kigaments, Synovial Mmebrane - Blood Suply, Nerve Supply, Movements and Important RelationsDocumento16 pagineAnkle Joint: Types, Capsule, Kigaments, Synovial Mmebrane - Blood Suply, Nerve Supply, Movements and Important RelationsaminaNessuna valutazione finora
- Anatomy Decoded - Q & A 1 To 7 Upper Limb - WhatsApp Premium Group PDFDocumento43 pagineAnatomy Decoded - Q & A 1 To 7 Upper Limb - WhatsApp Premium Group PDFNijam Udeen100% (1)
- Rabbit MusculatureDocumento95 pagineRabbit MusculatureMikee Abraham100% (1)
- Hip Joint Anatomy - Overview, Gross AnatomyDocumento14 pagineHip Joint Anatomy - Overview, Gross AnatomyZuraedha ZamilNessuna valutazione finora
- Multiple ligament knee injuries acute managementDocumento7 pagineMultiple ligament knee injuries acute managementekyNessuna valutazione finora
- Pelvic Floor Muscle ExerciseDocumento11 paginePelvic Floor Muscle ExercisedinnaNessuna valutazione finora
- The Muscular SystemDocumento6 pagineThe Muscular SystemJessah Dela PeñaNessuna valutazione finora
- Muscular System ExplainedDocumento36 pagineMuscular System ExplainedAjay Pal NattNessuna valutazione finora
- Muscle Manual From Active IQDocumento81 pagineMuscle Manual From Active IQRicardoMontenegroMartinezNessuna valutazione finora
- 70 150 1 SM PDFDocumento9 pagine70 150 1 SM PDFUsbahNessuna valutazione finora
- The Sliding Filament TheoryDocumento2 pagineThe Sliding Filament TheoryZaivie VillanobosNessuna valutazione finora
- PS 01 - Lower Limb Muscles Table From Gray'sDocumento4 paginePS 01 - Lower Limb Muscles Table From Gray'szivp610% (1)
- MuschiDocumento49 pagineMuschiBarbyy01Nessuna valutazione finora
- Knee BiomechanicsDocumento20 pagineKnee Biomechanicscrisanto valdezNessuna valutazione finora
- Chapter 06Documento7 pagineChapter 06Teehee Jones100% (5)
- Bab 12 - Muscular SystemDocumento73 pagineBab 12 - Muscular SystemDaeng FarahnazNessuna valutazione finora
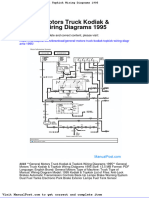
- General Motors Truck Kodiak Topkick Wiring Diagrams 1995Documento23 pagineGeneral Motors Truck Kodiak Topkick Wiring Diagrams 1995emilycollins260586owp99% (134)
- Muscular System ReviewerDocumento10 pagineMuscular System ReviewerGaille DacilloNessuna valutazione finora
- Adhesive Capsulitis Full PDFDocumento45 pagineAdhesive Capsulitis Full PDFjoanna gurtizaNessuna valutazione finora
- Abbas A. A. Shawka 2 Year Medical StudentDocumento15 pagineAbbas A. A. Shawka 2 Year Medical StudentPlutokidNessuna valutazione finora
- Muscular SystemDocumento15 pagineMuscular SystemReina Grace PanganibanNessuna valutazione finora
- Musculoskeletal Sports Ultrasound.1Documento2 pagineMusculoskeletal Sports Ultrasound.1Mateus AssisNessuna valutazione finora
- The Yogi Code: Seven Universal Laws of Infinite SuccessDa EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessValutazione: 4.5 su 5 stelle4.5/5 (104)
- Slow Burn: Burn Fat Faster By Exercising SlowerDa EverandSlow Burn: Burn Fat Faster By Exercising SlowerValutazione: 4.5 su 5 stelle4.5/5 (6)
- Chakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Da EverandChakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Valutazione: 4 su 5 stelle4/5 (2)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingDa EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingValutazione: 4.5 su 5 stelle4.5/5 (66)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!Da EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Valutazione: 4.5 su 5 stelle4.5/5 (22)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsDa EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsValutazione: 5 su 5 stelle5/5 (95)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindDa EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindValutazione: 4.5 su 5 stelle4.5/5 (1)
- Relentless: From Good to Great to UnstoppableDa EverandRelentless: From Good to Great to UnstoppableValutazione: 5 su 5 stelle5/5 (779)
- Meat Is for Pussies: A How-To Guide for Dudes Who Want to Get Fit, Kick Ass, and Take NamesDa EverandMeat Is for Pussies: A How-To Guide for Dudes Who Want to Get Fit, Kick Ass, and Take NamesValutazione: 3.5 su 5 stelle3.5/5 (8)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerDa EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerValutazione: 4 su 5 stelle4/5 (5)
- How Bad Do You Want It?: Mastering the Pshchology of Mind over MuscleDa EverandHow Bad Do You Want It?: Mastering the Pshchology of Mind over MuscleValutazione: 4.5 su 5 stelle4.5/5 (127)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesDa EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNessuna valutazione finora
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeDa EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeValutazione: 4.5 su 5 stelle4.5/5 (110)
- If You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsDa EverandIf You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsValutazione: 4.5 su 5 stelle4.5/5 (7)
- Hero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedDa EverandHero Maker: 12 Weeks to Superhero Fit: A Hollywood Trainer's REAL Guide to Getting the Body You've Always WantedValutazione: 4 su 5 stelle4/5 (1)
- Wheels of Life: A User's Guide to the Chakra SystemDa EverandWheels of Life: A User's Guide to the Chakra SystemValutazione: 4.5 su 5 stelle4.5/5 (33)
- Calisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesDa EverandCalisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesValutazione: 3 su 5 stelle3/5 (5)
- The Strength and Conditioning Bible: How to Train Like an AthleteDa EverandThe Strength and Conditioning Bible: How to Train Like an AthleteNessuna valutazione finora
- Calisthenics: 12 Effective Exercises to Build Calisthenics Body in 14 DaysDa EverandCalisthenics: 12 Effective Exercises to Build Calisthenics Body in 14 DaysValutazione: 3 su 5 stelle3/5 (5)
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingDa EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingValutazione: 4.5 su 5 stelle4.5/5 (18)
- Applied Polyvagal Theory in Yoga: Therapeutic Practices for Emotional HealthDa EverandApplied Polyvagal Theory in Yoga: Therapeutic Practices for Emotional HealthNessuna valutazione finora
- The Calisthenics Codex: Fifty Exercises for Functional FitnessDa EverandThe Calisthenics Codex: Fifty Exercises for Functional FitnessValutazione: 4 su 5 stelle4/5 (9)
- ROAR: How to Match Your Food and Fitness to Your Unique Female Physiology for Optimum Performance, Great Health, and a Strong, Lean Body for LifeDa EverandROAR: How to Match Your Food and Fitness to Your Unique Female Physiology for Optimum Performance, Great Health, and a Strong, Lean Body for LifeValutazione: 4.5 su 5 stelle4.5/5 (44)
- Light on Yoga: The Definitive Guide to Yoga PracticeDa EverandLight on Yoga: The Definitive Guide to Yoga PracticeValutazione: 5 su 5 stelle5/5 (1)
- 7 Weeks to 50 Pull-Ups: Strengthen and Sculpt Your Arms, Shoulders, Back, and Abs by Training to Do 50 Consecutive Pull-UpsDa Everand7 Weeks to 50 Pull-Ups: Strengthen and Sculpt Your Arms, Shoulders, Back, and Abs by Training to Do 50 Consecutive Pull-UpsValutazione: 3.5 su 5 stelle3.5/5 (2)