Potrebbero piacerti anche
- Julie Reznicek, Paul W. Perdue, JR., Gonzalo Bearman - Musculoskeletal Infections - A Clinical Case Book-Springer (2020)Documento230 pagineJulie Reznicek, Paul W. Perdue, JR., Gonzalo Bearman - Musculoskeletal Infections - A Clinical Case Book-Springer (2020)Medicine Essentials SimplifiedNessuna valutazione finora
- Personal BoundariesDocumento4 paginePersonal Boundariesscribdreaderplus75% (4)
- Spirit Releasement Protocol ListDocumento4 pagineSpirit Releasement Protocol ListKristen Hammer100% (5)
- Nausea and Vomiting (Algorithm) PDFDocumento2 pagineNausea and Vomiting (Algorithm) PDFAnggie Anggriyana0% (1)
- Syllabus ElectrotherapyDocumento4 pagineSyllabus ElectrotherapySYED ALI HUSSAINNessuna valutazione finora
- The List - Eric Falstrault - Strength SenseiDocumento11 pagineThe List - Eric Falstrault - Strength SenseiJon shieldNessuna valutazione finora
- Nursing Notes Maternal and Child Nursing CareDocumento70 pagineNursing Notes Maternal and Child Nursing CareAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Screenshot 2022-11-06 at 5.51.25 PMDocumento1 paginaScreenshot 2022-11-06 at 5.51.25 PMHadiya KhaleelNessuna valutazione finora
- Peter Pan Syndrome Is A DeepDocumento3 paginePeter Pan Syndrome Is A DeeptucklertNessuna valutazione finora
- Poisoning and Drug OverdoseDocumento95 paginePoisoning and Drug OverdoseMohammed Younis Shaheen100% (2)
- Health EDUC Teaching Demo RubricsDocumento4 pagineHealth EDUC Teaching Demo RubricsAsniah Hadjiadatu Abdullah100% (1)
- Pnle ReviewerDocumento293 paginePnle ReviewerAsniah Hadjiadatu Abdullah94% (18)
- Virginia HendersonDocumento4 pagineVirginia HendersonJoyce TanNessuna valutazione finora
- Transmicion: FiloviridaeDocumento15 pagineTransmicion: FiloviridaeDaniela Ortiz100% (1)
- CPR and First Aid PowerpointDocumento21 pagineCPR and First Aid PowerpointZawawiIbnuRosyidNessuna valutazione finora
- EBOLA Virus DiseaseDocumento5 pagineEBOLA Virus DiseaseLeah Malate100% (1)
- Class 12 CBSE Investigatory Project On EbolaDocumento19 pagineClass 12 CBSE Investigatory Project On EbolaAdriana Dkhar Toi50% (8)
- White Lesion 7Documento114 pagineWhite Lesion 7Samina TarikNessuna valutazione finora
- Ebola Virus DiseaseDocumento3 pagineEbola Virus DiseasePoonam RanaNessuna valutazione finora
- Ebola Virus Disease: Key FactsDocumento2 pagineEbola Virus Disease: Key FactsNi-el 'ndra' SantosoNessuna valutazione finora
- Key FactsDocumento8 pagineKey FactsKhartika MarthaNessuna valutazione finora
- WHO - Ebola Virus DiseaseDocumento6 pagineWHO - Ebola Virus Diseasedhoo_babyNessuna valutazione finora
- Ebola Virus Disease: Key FactsDocumento5 pagineEbola Virus Disease: Key Facts黄銮添Nessuna valutazione finora
- Ebola Virus Disease: Key FactsDocumento3 pagineEbola Virus Disease: Key FactsAnthony Miguel RafananNessuna valutazione finora
- 1) Crimean-Congo Hemorrhagic Fever (CCHF) : DiagnosisDocumento55 pagine1) Crimean-Congo Hemorrhagic Fever (CCHF) : DiagnosisKaish DahiyaNessuna valutazione finora
- Understanding Ebola VirusDocumento2 pagineUnderstanding Ebola VirusChellaMarieNessuna valutazione finora
- Ebola Virus Disease: Key FactsDocumento5 pagineEbola Virus Disease: Key FactsMichaelKimDugeniaNessuna valutazione finora
- CDC Ebola Fact SheetDocumento13 pagineCDC Ebola Fact Sheetيوسف سيمنزNessuna valutazione finora
- Ebola Virus DiseaseDocumento17 pagineEbola Virus DiseaseViorelNessuna valutazione finora
- Ebola (Ebola Virus Disease) : TransmissionDocumento2 pagineEbola (Ebola Virus Disease) : TransmissionCaleb VoosNessuna valutazione finora
- Key FactsDocumento4 pagineKey FactsAnonymous JOOQkGbwoRNessuna valutazione finora
- Ebola RPRTDocumento19 pagineEbola RPRTDel FinNessuna valutazione finora
- Ebola - The Killer VirusDocumento3 pagineEbola - The Killer VirusLalit SinghNessuna valutazione finora
- Ebola Virus DiseaseDocumento2 pagineEbola Virus DiseaseBLETIVENessuna valutazione finora
- WHO - Ebola Virus Disease (Evd) Key FactsDocumento6 pagineWHO - Ebola Virus Disease (Evd) Key FactsBeatrice IoanaNessuna valutazione finora
- 19301920115-PT 818Documento8 pagine19301920115-PT 818Susmita GhoshNessuna valutazione finora
- EbolaDocumento20 pagineEbolaFabian PitkinNessuna valutazione finora
- Choo Choy Tian 00000027562 CH219 Practical ReportDocumento6 pagineChoo Choy Tian 00000027562 CH219 Practical ReportWei Hao ChanNessuna valutazione finora
- Ebola Epidemic: Unit 3Documento2 pagineEbola Epidemic: Unit 3Nia NormayunitaNessuna valutazione finora
- Ebola Virus DiseaseDocumento4 pagineEbola Virus Diseasev_vijayakanth7656Nessuna valutazione finora
- Ebola: What Clinicians Need To KnowDocumento3 pagineEbola: What Clinicians Need To KnowIman100% (1)
- Project Topic:: Human Biology Course Code: SectionDocumento9 pagineProject Topic:: Human Biology Course Code: SectionRadioactiveNessuna valutazione finora
- HS 2212-01 Infectious Diseases - AY2023-T2-Written Assignment Unit 5Documento6 pagineHS 2212-01 Infectious Diseases - AY2023-T2-Written Assignment Unit 5bnvjNessuna valutazione finora
- Biology Ebola Virus Project ReportDocumento19 pagineBiology Ebola Virus Project ReportChaitaneyMorNessuna valutazione finora
- About Ebola Hemorrhagic FeverDocumento5 pagineAbout Ebola Hemorrhagic FeverMiryam ChNessuna valutazione finora
- Ebola Health Education CHNDocumento23 pagineEbola Health Education CHNBrijesh YadavNessuna valutazione finora
- Bahasa Inggris 1Documento41 pagineBahasa Inggris 1RizqyAuliaNestaNessuna valutazione finora
- EBOLADocumento2 pagineEBOLAamirNessuna valutazione finora
- Bio Project Class 12Documento15 pagineBio Project Class 12joyitaNessuna valutazione finora
- Submitted To - Shalini Mam Submitted by - Yash Nagar Class - XII B Roll No.Documento10 pagineSubmitted To - Shalini Mam Submitted by - Yash Nagar Class - XII B Roll No.Yash Nagar100% (1)
- Hkaro - PeroDocumento5 pagineHkaro - PeroDANA S. SALIMNessuna valutazione finora
- EbolaDocumento4 pagineEbolaPratham RD JainNessuna valutazione finora
- EbolaDocumento4 pagineEbolaArathi KarshNessuna valutazione finora
- Ebola Virus Disease (WHO) : Key FactsDocumento5 pagineEbola Virus Disease (WHO) : Key FactsridhosetyawanNessuna valutazione finora
- Ebola Virnzddfus: Prepared by BLACK Professor: NB Year: 2019-2020 Subject: HDFHDFHDDocumento5 pagineEbola Virnzddfus: Prepared by BLACK Professor: NB Year: 2019-2020 Subject: HDFHDFHDDANA S. SALIMNessuna valutazione finora
- Ebola Virnzddfus: Prepared by BLACK Professor: NB Year: 2019-2020 Subject: HDFHDFHDDocumento5 pagineEbola Virnzddfus: Prepared by BLACK Professor: NB Year: 2019-2020 Subject: HDFHDFHDDANA S. SALIMNessuna valutazione finora
- Ebola Virnzddfus: Prepared by BLACK Professor: NB Year: 2019-2020 Subject: HDFHDFHDDocumento5 pagineEbola Virnzddfus: Prepared by BLACK Professor: NB Year: 2019-2020 Subject: HDFHDFHDDANA S. SALIMNessuna valutazione finora
- Ebola Virus 2Documento17 pagineEbola Virus 2Rashid madniNessuna valutazione finora
- An Overview of Ebola. An Emerging VirusDocumento7 pagineAn Overview of Ebola. An Emerging VirusBhaskar ReddyNessuna valutazione finora
- Ebola Virus: Prepared By: Gona Sirwan Salim Professor: M.Sonya Year: 2019-2020 Subject: Practical VirologyDocumento5 pagineEbola Virus: Prepared By: Gona Sirwan Salim Professor: M.Sonya Year: 2019-2020 Subject: Practical VirologyDANA S. SALIMNessuna valutazione finora
- North South UniversityDocumento3 pagineNorth South UniversityFoyez ChowdhuryNessuna valutazione finora
- North South University: Submitted ToDocumento13 pagineNorth South University: Submitted ToProbir Saha (192051023)Nessuna valutazione finora
- Term Paper Ebola VirusDocumento5 pagineTerm Paper Ebola Virusc5qj4swh100% (1)
- Ebola Virus Research Paper PDFDocumento4 pagineEbola Virus Research Paper PDFkcjzgcsifNessuna valutazione finora
- Ebola Virus DiseaseDocumento13 pagineEbola Virus DiseaseMade Sudarsana0% (1)
- Dissertation Virus EbolaDocumento8 pagineDissertation Virus EbolaCustomWritingPapersKnoxville100% (1)
- EBOLADocumento4 pagineEBOLAwawa3385Nessuna valutazione finora
- Ebola Virus Disease (EVD) : What Are The Symptoms?Documento2 pagineEbola Virus Disease (EVD) : What Are The Symptoms?Travel Health FremantleNessuna valutazione finora
- WHO - Ebola Haemorrhagic Fever.Documento3 pagineWHO - Ebola Haemorrhagic Fever.CSilva16Nessuna valutazione finora
- Ebola Virus Disease: Key FactsDocumento3 pagineEbola Virus Disease: Key FactsruguNessuna valutazione finora
- Ebola Virus DiseaseDocumento6 pagineEbola Virus DiseaseDyan LazoNessuna valutazione finora
- Ebola Virus DiseaseDocumento9 pagineEbola Virus DiseaseApoorva VermaNessuna valutazione finora
- Daniel Saladas ResumeDocumento2 pagineDaniel Saladas ResumeAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Application Forms (Fillable)Documento2 pagineApplication Forms (Fillable)Asniah Hadjiadatu AbdullahNessuna valutazione finora
- CV 2023010319584829Documento1 paginaCV 2023010319584829Asniah Hadjiadatu AbdullahNessuna valutazione finora
- Credential Verification Form Non-Clinical (Without Signature Page)Documento1 paginaCredential Verification Form Non-Clinical (Without Signature Page)Asniah Hadjiadatu AbdullahNessuna valutazione finora
- FNCP PoorsanitationmarwahDocumento3 pagineFNCP PoorsanitationmarwahAsniah Hadjiadatu AbdullahNessuna valutazione finora
- To Fill-Up Id-Atm FormDocumento7 pagineTo Fill-Up Id-Atm FormAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Poor Environmetal Sanitation As Health Threat CuesDocumento11 paginePoor Environmetal Sanitation As Health Threat CuesAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Family Case Study PresentationDocumento1 paginaFamily Case Study PresentationAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Poor Compliance With Treatment As Health Threat CuesDocumento11 paginePoor Compliance With Treatment As Health Threat CuesAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Health Teaching Plan FinaleDocumento4 pagineHealth Teaching Plan FinaleAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDocumento12 pagineAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Family Case Study On Pulmonary TuberculosisDocumento4 pagineFamily Case Study On Pulmonary TuberculosisAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Family Case StudyDocumento33 pagineFamily Case StudyAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Mock ResumeDocumento3 pagineMock ResumeAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Water RescueDocumento7 pagineWater RescueAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Or/Dr/Nicu/Pacu Requirements: Open Wound TypesDocumento6 pagineOr/Dr/Nicu/Pacu Requirements: Open Wound TypesAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Proposed Budget For The 17th Striping and Pinning Investiture CeremonyDocumento1 paginaProposed Budget For The 17th Striping and Pinning Investiture CeremonyAsniah Hadjiadatu AbdullahNessuna valutazione finora
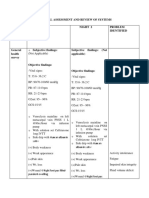
- Physical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedDocumento9 paginePhysical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Concept Map AtekharlssDocumento3 pagineConcept Map AtekharlssAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Assessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationDocumento11 pagineAssessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationAsniah Hadjiadatu Abdullah100% (1)
- Final Nursing CareplanDocumento7 pagineFinal Nursing CareplanAsniah Hadjiadatu AbdullahNessuna valutazione finora
- Psychiatric-Mental Health NursingDocumento6 paginePsychiatric-Mental Health NursingAsniah Hadjiadatu AbdullahNessuna valutazione finora
- The Good and Bad Effects of TV On ChildrenDocumento4 pagineThe Good and Bad Effects of TV On Childrenapi-206219067100% (1)
- Homeopathic Materia Medica by Farrington Causticum (Caust) : Lecture Lxxi Lecture LxxiiDocumento7 pagineHomeopathic Materia Medica by Farrington Causticum (Caust) : Lecture Lxxi Lecture LxxiimyoxusNessuna valutazione finora
- Internal Fixation ToolsDocumento22 pagineInternal Fixation ToolsChandan Kumar ChoubeyNessuna valutazione finora
- ILS 2014 Final Year Revision LectureDocumento54 pagineILS 2014 Final Year Revision LectureokaberntrNessuna valutazione finora
- Olympian Benchmark - 400mDocumento15 pagineOlympian Benchmark - 400merwandumontNessuna valutazione finora
- Fibromyalgia PDFDocumento5 pagineFibromyalgia PDFYalile TurkaNessuna valutazione finora
- How To Treat Varicose VeinsDocumento2 pagineHow To Treat Varicose VeinsTee VillanuevaNessuna valutazione finora
- Book Reviews: Trigger Points and Muscle Chains in OsteopathyDocumento4 pagineBook Reviews: Trigger Points and Muscle Chains in OsteopathyConstanza López MillerNessuna valutazione finora
- TrandolaprilDocumento28 pagineTrandolaprilYeyenJaejoongNessuna valutazione finora
- Fundamentals of Rheumatoid Arthritis and Various Homoeopathic Trials in Patients of Rheumatoid Arthritis: An UpdateDocumento6 pagineFundamentals of Rheumatoid Arthritis and Various Homoeopathic Trials in Patients of Rheumatoid Arthritis: An UpdateHomoeopathic PulseNessuna valutazione finora
- Infection Control in NurseryDocumento6 pagineInfection Control in NurserysobinjohnpklNessuna valutazione finora
- Chapter 4 A1 Poster Example 2Documento3 pagineChapter 4 A1 Poster Example 2Krisna PamungkasNessuna valutazione finora
- Abnormal Psychology Notes: Anxiety DisordersDocumento4 pagineAbnormal Psychology Notes: Anxiety DisordersAshley ChenenNessuna valutazione finora
- West Visayas State University Medical Center E. Lopez St. Jaro Iloilo CityDocumento7 pagineWest Visayas State University Medical Center E. Lopez St. Jaro Iloilo CityRegine Marie EspañaNessuna valutazione finora
- Dopamine D Liverpool PDFDocumento4 pagineDopamine D Liverpool PDFcacingpandora100% (1)
- 2212-02e TPB PAC Liquid 10Documento1 pagina2212-02e TPB PAC Liquid 10Saefuddin SaefuddinNessuna valutazione finora
- Aplastic AnemiaDocumento3 pagineAplastic AnemiaFrancis JuneNessuna valutazione finora
- NCP Micu Hascvd Cad - RioDocumento5 pagineNCP Micu Hascvd Cad - RioRio BonifacioNessuna valutazione finora
- Oral Preparations: Erdosteine ZertinDocumento4 pagineOral Preparations: Erdosteine ZertinmagreaNessuna valutazione finora