Potrebbero piacerti anche
- On Admission:: STROKE MANAGEMENT (Beaumont Hospital)Documento3 pagineOn Admission:: STROKE MANAGEMENT (Beaumont Hospital)Nadia SalwaniNessuna valutazione finora
- ACLS Drug TherapyDocumento8 pagineACLS Drug TherapySahrensNessuna valutazione finora
- Acute Renal FailureDocumento5 pagineAcute Renal FailureSalman KhanNessuna valutazione finora
- 2017 05 GC Pocket CardDocumento2 pagine2017 05 GC Pocket Cardapi-312241089Nessuna valutazione finora
- Acute Glomerulonephritis: Group 8 PresentationDocumento25 pagineAcute Glomerulonephritis: Group 8 PresentationcollinsmagNessuna valutazione finora
- Electrolyte DisordersDocumento10 pagineElectrolyte DisordersSlavicaNessuna valutazione finora
- ATSP (Asked To See Patient) BookletDocumento24 pagineATSP (Asked To See Patient) BookletCindy WongNessuna valutazione finora
- 2013 Sepsis GuidelinesDocumento58 pagine2013 Sepsis GuidelinesMuhd Azam100% (1)
- Secondary Arterial HypertensionDocumento32 pagineSecondary Arterial HypertensionAndi SusiloNessuna valutazione finora
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- M&M Hypovolemic ShockDocumento30 pagineM&M Hypovolemic ShockRyan FornollesNessuna valutazione finora
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- PATHOPHYSIOLOGY OF SHOCKDocumento56 paginePATHOPHYSIOLOGY OF SHOCKDr. Haricharan ANessuna valutazione finora
- Es I Algorithm PosterDocumento2 pagineEs I Algorithm Posterkusdiyah ningrumNessuna valutazione finora
- Alopecia: By. Mr. P. Dhilip KumarDocumento9 pagineAlopecia: By. Mr. P. Dhilip Kumarpreet kaur100% (1)
- CANINE-Spontaneous Pneumothorax in DogsDocumento7 pagineCANINE-Spontaneous Pneumothorax in Dogstaner_soysurenNessuna valutazione finora
- APPROACH TO MANAGING JOINT PAINDocumento44 pagineAPPROACH TO MANAGING JOINT PAINKavya Anoop100% (1)
- Opportunistic Infections in HIVDocumento50 pagineOpportunistic Infections in HIVamandaNessuna valutazione finora
- Neurological Manifestations of HIV/AIDSDocumento34 pagineNeurological Manifestations of HIV/AIDSashuNessuna valutazione finora
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocumento74 pagineBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- Acute CNS Infections Diagnosis GuideDocumento53 pagineAcute CNS Infections Diagnosis GuideEhab KhiryNessuna valutazione finora
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Fluid, Electrolyte and Acid-Base BalanceDocumento42 pagineFluid, Electrolyte and Acid-Base BalanceMiss Vina100% (1)
- Green Dialysis - Prof - SantoroDocumento25 pagineGreen Dialysis - Prof - SantorogreennephroNessuna valutazione finora
- Critical Patient Monitoring CriteriaDocumento3 pagineCritical Patient Monitoring CriteriaSundaresan MNessuna valutazione finora
- Essentials of Diagnosis and Treatment of Acute LeukemiaDocumento16 pagineEssentials of Diagnosis and Treatment of Acute Leukemianouval_iqbalNessuna valutazione finora
- Basics of AnesthesiaDocumento34 pagineBasics of Anesthesiadremad1974Nessuna valutazione finora
- Delirium in critically ill patients: Should we worryDocumento37 pagineDelirium in critically ill patients: Should we worrySanj.etcNessuna valutazione finora
- Hypovolemic ShockDocumento21 pagineHypovolemic ShockOlga GoryachevaNessuna valutazione finora
- Patient Examination GuideDocumento118 paginePatient Examination GuideJun JavierNessuna valutazione finora
- Emergency Department Staffing PlanDocumento5 pagineEmergency Department Staffing PlanshahidchaudharyNessuna valutazione finora
- DR Aida Lombok 3 Mei 2017 - HisfarsiDocumento39 pagineDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamNessuna valutazione finora
- Invasive Pulmonary Aspergi Llosis: Seminars in Respiratory and Critical Care MedicineDocumento24 pagineInvasive Pulmonary Aspergi Llosis: Seminars in Respiratory and Critical Care MedicineChengShiun ShiueNessuna valutazione finora
- Innovation EDDocumento32 pagineInnovation EDAETCM Emergency medicineNessuna valutazione finora
- Hypertensive Emergencies (ESC 2019)Documento10 pagineHypertensive Emergencies (ESC 2019)Glen LazarusNessuna valutazione finora
- Diabetes Case Study Fall 2016 1Documento7 pagineDiabetes Case Study Fall 2016 1api-284823421Nessuna valutazione finora
- Intensive Care Trauma SheetDocumento2 pagineIntensive Care Trauma SheetalexipsNessuna valutazione finora
- Up-Pgh Competency Program For New EmployeeDocumento49 pagineUp-Pgh Competency Program For New EmployeeMichael SilvaNessuna valutazione finora
- Rapid Response TeamDocumento4 pagineRapid Response TeamMichael SilvaNessuna valutazione finora
- NHS DIABETESUNDERGOING Surgery Adults Full PDFDocumento72 pagineNHS DIABETESUNDERGOING Surgery Adults Full PDFekyNessuna valutazione finora
- KegawatdaruratanDocumento164 pagineKegawatdaruratanmeida astriani gozaziNessuna valutazione finora
- Checklist of Nonverbal Pain IndicatorsDocumento41 pagineChecklist of Nonverbal Pain IndicatorsantipaticoNessuna valutazione finora
- Post-Cardiac Arrest Therapeutic Hypothermia Targeted Temperature Manangement (TTM) Quick SheetDocumento3 paginePost-Cardiac Arrest Therapeutic Hypothermia Targeted Temperature Manangement (TTM) Quick SheetkimberlyNessuna valutazione finora
- Blood Transfusion - Sep 08 1 (1) Edited) NightDocumento13 pagineBlood Transfusion - Sep 08 1 (1) Edited) Nightmyvi31788% (8)
- Glasgow Coma Scale assessment and physical exam checklistDocumento1 paginaGlasgow Coma Scale assessment and physical exam checklistbrownehsNessuna valutazione finora
- GI BLEED - Medicine - Internal MedicineDocumento11 pagineGI BLEED - Medicine - Internal Medicinezezma GamingNessuna valutazione finora
- Massive Transfusion ProtocolDocumento11 pagineMassive Transfusion ProtocolAlaa Abdelmoaty OmranNessuna valutazione finora
- Isbi Practice Guidelines For Burn Care Part 2 2018 PDFDocumento90 pagineIsbi Practice Guidelines For Burn Care Part 2 2018 PDFAstri SuyataNessuna valutazione finora
- Regional AnesthesiaDocumento54 pagineRegional AnesthesiaIdza Fariha AfriNessuna valutazione finora
- Hemophilia: Factor IX (Hemophilia B)Documento38 pagineHemophilia: Factor IX (Hemophilia B)Jhvhjgj JhhgtyNessuna valutazione finora
- Esophageal Varices Week 4 T2T3Documento37 pagineEsophageal Varices Week 4 T2T3liewhuilianNessuna valutazione finora
- Acid Base Disorders - Lecture 45Documento14 pagineAcid Base Disorders - Lecture 45yassin mostafaNessuna valutazione finora
- Integrated ChecklistDocumento2 pagineIntegrated ChecklistKena BenNessuna valutazione finora
- COPD Differential Diagnosis ModuleDocumento44 pagineCOPD Differential Diagnosis ModulenicusoorNessuna valutazione finora
- Dr. Surya Abadi KristyoadiDocumento42 pagineDr. Surya Abadi KristyoadiDr. Surya Abadi KristyoadiNessuna valutazione finora
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocumento4 pagineRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniNessuna valutazione finora
- Shock (For Surgery)Documento50 pagineShock (For Surgery)Emmanuel Rojith VazNessuna valutazione finora
- STEP HPEF Trial NEJm 2023Documento16 pagineSTEP HPEF Trial NEJm 2023felipeNessuna valutazione finora
- APICON 2019 Brochure PDFDocumento24 pagineAPICON 2019 Brochure PDFrasakatla jaswanthNessuna valutazione finora
- Guide to Evaluating Acute MonoarthritisDocumento28 pagineGuide to Evaluating Acute MonoarthritisShrouk EldakroryNessuna valutazione finora
- 14-Child With ArthritisDocumento44 pagine14-Child With Arthritisزياد سعيدNessuna valutazione finora
- Clinical Approach To Acute Arthritis: Yolanda Farhey, MD Assistant Professor Division of ImmunologyDocumento77 pagineClinical Approach To Acute Arthritis: Yolanda Farhey, MD Assistant Professor Division of ImmunologyAmine YounisNessuna valutazione finora
- Seronegative Spodyloarthropathy-1Documento29 pagineSeronegative Spodyloarthropathy-1azza271421Nessuna valutazione finora
- Acs PDFDocumento1 paginaAcs PDFPowool LalaNessuna valutazione finora
- Stu Lts HyperDocumento54 pagineStu Lts HyperPowool LalaNessuna valutazione finora
- Keynote Lecture. Importance of CME in Emergency Management (Dr. Dr. Eugenius Phyowai Ganap, SP - OG (K) ) PDFDocumento45 pagineKeynote Lecture. Importance of CME in Emergency Management (Dr. Dr. Eugenius Phyowai Ganap, SP - OG (K) ) PDFPowool LalaNessuna valutazione finora
- Dr. Suryono, SPJPDocumento26 pagineDr. Suryono, SPJPPowool LalaNessuna valutazione finora
- Guideline For The Diagnosis and Management of Hypertension in Adults - 2016Documento84 pagineGuideline For The Diagnosis and Management of Hypertension in Adults - 2016Are Pee Etc100% (1)
- HFHS CKD V6Documento76 pagineHFHS CKD V6medicalNessuna valutazione finora
- Silabus Materi Clinical Update 2019 PDFDocumento36 pagineSilabus Materi Clinical Update 2019 PDFPowool LalaNessuna valutazione finora
- Acca Toolkit 2018Documento212 pagineAcca Toolkit 2018daltonngangi100% (3)
- Spinal Injury & Spinal Cord InjuryDocumento66 pagineSpinal Injury & Spinal Cord InjuryPowool LalaNessuna valutazione finora
- Wound CareDocumento60 pagineWound CareNila WatiNessuna valutazione finora
- Pretest Dan Posttest PDFDocumento9 paginePretest Dan Posttest PDFPowool LalaNessuna valutazione finora
- Stereo TacticDocumento61 pagineStereo TacticPowool LalaNessuna valutazione finora
- 11.VIRAL Infection PADA KULITedited - PPT (Compatibility Mode)Documento8 pagine11.VIRAL Infection PADA KULITedited - PPT (Compatibility Mode)pheeplukzNessuna valutazione finora
- Post Herpetic NeuralgiaDocumento44 paginePost Herpetic NeuralgiaRia Puji PangestutiNessuna valutazione finora
- Bukue4edDocumento69 pagineBukue4edPowool LalaNessuna valutazione finora
- Bicol University College of Nursing Protozoans ComparisonDocumento3 pagineBicol University College of Nursing Protozoans ComparisonAbegail ListancoNessuna valutazione finora
- Encefalitis ViralDocumento5 pagineEncefalitis ViralRandy UlloaNessuna valutazione finora
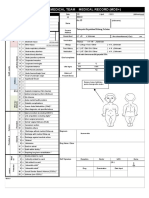
- Emergency Medical Team Medical Record (MDS+) : MDS - Check All That ApplyDocumento2 pagineEmergency Medical Team Medical Record (MDS+) : MDS - Check All That ApplySyafiraIdhatunNasyiahNessuna valutazione finora
- Covid-19 Pandemic and Its Impacts On Micro Small and Medium Enterprises of AssamDocumento8 pagineCovid-19 Pandemic and Its Impacts On Micro Small and Medium Enterprises of AssamIJAR JOURNALNessuna valutazione finora
- Paper 1: Concept of Health and DiseaseDocumento7 paginePaper 1: Concept of Health and DiseaseYash LohiyaNessuna valutazione finora
- Carolyn R. Zalameda-Castro, MDDocumento9 pagineCarolyn R. Zalameda-Castro, MDeza floresNessuna valutazione finora
- Diabetic Treatment Adherence at LASUTHDocumento63 pagineDiabetic Treatment Adherence at LASUTHijojo elizabethNessuna valutazione finora
- Managing Hypertension and Rheumatoid ArthritisDocumento2 pagineManaging Hypertension and Rheumatoid ArthritisKristinelou Marie ReynaNessuna valutazione finora
- Intestinal Flukes Liver Flukes Lung Flukes Blood Flukes: SinensisDocumento3 pagineIntestinal Flukes Liver Flukes Lung Flukes Blood Flukes: SinensisCHO-ON KIMNessuna valutazione finora
- Medical Parasitology A Self Instructional Text PDFDriveDocumento60 pagineMedical Parasitology A Self Instructional Text PDFDriveDenise Sta. AnaNessuna valutazione finora
- Postural Vital SignsDocumento3 paginePostural Vital Signsriffs_ahoyNessuna valutazione finora
- Framingham Data Famous Cohort Study of 5209 Subjects From Framingham MADocumento2 pagineFramingham Data Famous Cohort Study of 5209 Subjects From Framingham MAEdwin Johny Asnate SalazarNessuna valutazione finora
- Rundown AcaraDocumento3 pagineRundown Acaradedy nurmantoroNessuna valutazione finora
- Script EFN Hiv AidsDocumento3 pagineScript EFN Hiv AidsRina Mulyasari Mar Atussa'adahNessuna valutazione finora
- Vaccines in Zimbabwe InformationDocumento8 pagineVaccines in Zimbabwe InformationIsaac GumboNessuna valutazione finora
- Nail PsoriasisDocumento8 pagineNail PsoriasisNurdiana DwikarwatiNessuna valutazione finora
- Ethical Issues in Mandatory Smallpox VaccinationDocumento2 pagineEthical Issues in Mandatory Smallpox VaccinationFaizaNadeemNessuna valutazione finora
- ICRT Dubai Brochure - 0Documento12 pagineICRT Dubai Brochure - 0Godfrey MwansaNessuna valutazione finora
- Snake Bite First AidDocumento6 pagineSnake Bite First Aidmelchor bangaoilNessuna valutazione finora
- M1.U1. TutorialDocumento7 pagineM1.U1. TutorialRizki DiniNessuna valutazione finora
- 3rd Q LONG TEST IN HealthDocumento2 pagine3rd Q LONG TEST IN HealthDennmark IgutNessuna valutazione finora
- Amantillo ParkinsonsDocumento14 pagineAmantillo ParkinsonsATEHAN BORDSNessuna valutazione finora
- Pathogen Research AssignmentDocumento2 paginePathogen Research AssignmentDeven BaliNessuna valutazione finora
- Rheum at OlogyDocumento42 pagineRheum at Ologymy Lord JesusNessuna valutazione finora
- Low Back Pain in Car Drivers: A Review of Studies Published 1975 To 2005Documento15 pagineLow Back Pain in Car Drivers: A Review of Studies Published 1975 To 2005ViolintsarNessuna valutazione finora
- English Language Dialogue On HIVDocumento5 pagineEnglish Language Dialogue On HIVAFRI YUNIKANessuna valutazione finora
- Computer-Based English Proficiency Test AdvisoryDocumento7 pagineComputer-Based English Proficiency Test AdvisoryJoyce CarilloNessuna valutazione finora
- VaccinationCard 921591189Documento1 paginaVaccinationCard 921591189Haris PakyaraNessuna valutazione finora