Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Mnemonic For Forearm Muscles and BoneDocumento2 pagineMnemonic For Forearm Muscles and BoneLaura Tapia89% (28)
- Child Birth and The Natural BirthDocumento10 pagineChild Birth and The Natural BirthMohan Perera100% (17)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- .. Uploads Lecture Implant Overdenture 200702Documento21 pagine.. Uploads Lecture Implant Overdenture 200702siddu76100% (1)
- Overview of The Philippine Health SystemDocumento10 pagineOverview of The Philippine Health SystemCaryl Ann RabanosNessuna valutazione finora
- Tisum 1Documento3 pagineTisum 1Joe JoeNessuna valutazione finora
- Contributo - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreasDocumento17 pagineContributo - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreasJoe JoeNessuna valutazione finora
- Video Conten - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreaDocumento1 paginaVideo Conten - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreaJoe JoeNessuna valutazione finora
- Tis Umum-1Documento2 pagineTis Umum-1Joe JoeNessuna valutazione finora
- ShoelaceDocumento5 pagineShoelaceJoe JoeNessuna valutazione finora
- Varicocele C To MyDocumento1 paginaVaricocele C To MyJoe JoeNessuna valutazione finora
- Trauma Scores and Scoring SystemsDocumento26 pagineTrauma Scores and Scoring SystemsNurhayati TimumunNessuna valutazione finora
- Colles' FractureDocumento4 pagineColles' FractureJoe JoeNessuna valutazione finora
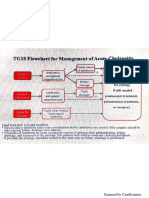
- Criterios de Tokio 2018Documento14 pagineCriterios de Tokio 2018Luis CoraspeNessuna valutazione finora
- Martin Abd Stab Wounds SyllabusDocumento9 pagineMartin Abd Stab Wounds SyllabusJoanne Ventura Advincula-IliligayNessuna valutazione finora
- Criterios de Tokio 2018Documento14 pagineCriterios de Tokio 2018Luis CoraspeNessuna valutazione finora
- Tokyo GuidelineDocumento7 pagineTokyo GuidelineJoe JoeNessuna valutazione finora
- Exercise & Diet: The Importance ofDocumento2 pagineExercise & Diet: The Importance ofEve Jay TaboclaonNessuna valutazione finora
- 7 Tips To Stay Mentally Healthy During CrisisDocumento2 pagine7 Tips To Stay Mentally Healthy During CrisisnoemiNessuna valutazione finora
- Jawaharlal Nehru Technological University Kakinada: T Ime T A B L EDocumento2 pagineJawaharlal Nehru Technological University Kakinada: T Ime T A B L Ezyx888Nessuna valutazione finora
- IDA Edelweiss Gallagher Final 25yrsDocumento5 pagineIDA Edelweiss Gallagher Final 25yrsShital KiranNessuna valutazione finora
- Anesthesiology Table of Contents 2018 PDFDocumento822 pagineAnesthesiology Table of Contents 2018 PDFRaul ForjanNessuna valutazione finora
- Guide Health Sector Categories in IrelandDocumento69 pagineGuide Health Sector Categories in IrelandprotoginaNessuna valutazione finora
- Office of The Mayor: Republic of The Philippines Province of La Union Municipality of Caba Tel. # (072) 607-03-12Documento3 pagineOffice of The Mayor: Republic of The Philippines Province of La Union Municipality of Caba Tel. # (072) 607-03-12Sunshine MaglayaNessuna valutazione finora
- Expanded Role of NursesDocumento32 pagineExpanded Role of NursesAnthony Riggs100% (2)
- "Glimpse of The Future" by Cyril Jonas PlanillaDocumento5 pagine"Glimpse of The Future" by Cyril Jonas PlanillaVin CustodioNessuna valutazione finora
- Munirah Et Al. 2022 - Crocus Sativus For Insomnia Systemic Review and Meta-AnalysisDocumento16 pagineMunirah Et Al. 2022 - Crocus Sativus For Insomnia Systemic Review and Meta-AnalysisLaura DecockNessuna valutazione finora
- Final IlmuladvDocumento6 pagineFinal IlmuladvFaisal Abbas BastamiNessuna valutazione finora
- Grade+8+-+P E +&+healthDocumento42 pagineGrade+8+-+P E +&+healthauxiee yvieNessuna valutazione finora
- Care, Cure, Core TheoryDocumento17 pagineCare, Cure, Core TheoryLouzcelle DAPATNessuna valutazione finora
- Mou of East West TpaDocumento13 pagineMou of East West Tpamalayanur rama chandraNessuna valutazione finora
- Herbal Medicine For Treatment and Prevention of Liver DiseasesDocumento6 pagineHerbal Medicine For Treatment and Prevention of Liver Diseaseskartini ciatawiNessuna valutazione finora
- Sanjivani Psychosocial Rehabilitation Centre, Nedumkunnam, Kottayam DT., KeralaDocumento3 pagineSanjivani Psychosocial Rehabilitation Centre, Nedumkunnam, Kottayam DT., KeralaJSM MKZYNessuna valutazione finora
- International Postnatal Growth Standards For Preterm InfantsDocumento3 pagineInternational Postnatal Growth Standards For Preterm InfantsNovalinda KasihNessuna valutazione finora
- Future of Clinical Engineering - J.tobey Clark - 2003Documento10 pagineFuture of Clinical Engineering - J.tobey Clark - 2003ManojNessuna valutazione finora
- Ama Report of The Council On Science and Public Health Obesity As A DiseaseDocumento14 pagineAma Report of The Council On Science and Public Health Obesity As A Diseaseapi-285790500Nessuna valutazione finora
- Critical Care of Pet BirdsDocumento12 pagineCritical Care of Pet BirdsLeslie CadavidNessuna valutazione finora
- Psychosocial Support For Parents of Extremely PretDocumento13 paginePsychosocial Support For Parents of Extremely PretDag AraNessuna valutazione finora
- The QUADAS Tool: Item Yes No UnclearDocumento1 paginaThe QUADAS Tool: Item Yes No UnclearAndrea PederziniNessuna valutazione finora
- Post Test On Food and Water Borne DiseasesDocumento4 paginePost Test On Food and Water Borne DiseasesMardie ArcesNessuna valutazione finora
- Epigastric Pulsation: Prevalence and Association With Co-Morbidities in Ksa, A Cross-Sectional Descriptive StudyDocumento6 pagineEpigastric Pulsation: Prevalence and Association With Co-Morbidities in Ksa, A Cross-Sectional Descriptive StudyIJAR JOURNALNessuna valutazione finora
- Ivy Miah Business Report Draft 1Documento8 pagineIvy Miah Business Report Draft 1api-580141445Nessuna valutazione finora
- I Great Medi Care Pds enDocumento6 pagineI Great Medi Care Pds enainafaqeeraNessuna valutazione finora
- Nutrition Recommendations in Pregnancy and LactationDocumento17 pagineNutrition Recommendations in Pregnancy and LactationDodi TambunNessuna valutazione finora