Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Effect of Integrated Nutrient and Weed Management Practices On Weeds, Growth and Yieldand Economics of Transplanted RiceDocumento13 pagineEffect of Integrated Nutrient and Weed Management Practices On Weeds, Growth and Yieldand Economics of Transplanted RiceAparajay SurnamelessNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- An Obituary On Caste As A SystemDocumento5 pagineAn Obituary On Caste As A SystemAparajay SurnamelessNessuna valutazione finora
- Education at Santiniketan - 1902-1920Documento15 pagineEducation at Santiniketan - 1902-1920Aparajay SurnamelessNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hindu-Muslim Relations in The Works of TagoreDocumento19 pagineHindu-Muslim Relations in The Works of TagoreAparajay SurnamelessNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Baig - THE PARTITION OF BENGAL AND ITS AFTERMATHDocumento28 pagineBaig - THE PARTITION OF BENGAL AND ITS AFTERMATHAparajay SurnamelessNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Sumit Sarkar - THE SWADESHI MOVEMENT IN Bengal 1903-1908Documento457 pagineSumit Sarkar - THE SWADESHI MOVEMENT IN Bengal 1903-1908Aparajay SurnamelessNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Effect of Crop Establishment Methods and Organic - RiceDocumento5 pagineEffect of Crop Establishment Methods and Organic - RiceAparajay SurnamelessNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Effect of Crop Establishment Methods and Organic - RiceDocumento5 pagineEffect of Crop Establishment Methods and Organic - RiceAparajay SurnamelessNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- An Economic Analysis of Different Rice Varieties in Cauvery Delta Region of Tamil NaduDocumento6 pagineAn Economic Analysis of Different Rice Varieties in Cauvery Delta Region of Tamil NaduAparajay SurnamelessNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Effect of Integrated NPK Management On The Productivity of Rice-RiceDocumento4 pagineEffect of Integrated NPK Management On The Productivity of Rice-RiceAparajay SurnamelessNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Effect of Herbicides For Enhancing TheDocumento5 pagineEffect of Herbicides For Enhancing TheAparajay SurnamelessNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Right To The CityDocumento16 pagineRight To The CitySofía RuizNessuna valutazione finora
- A Case For Silicon Fertilization To Improve Crop YieldsDocumento14 pagineA Case For Silicon Fertilization To Improve Crop YieldsNanda Hendra PratamaNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Effect of Fly Ash and Silicate SolubilizingDocumento7 pagineEffect of Fly Ash and Silicate SolubilizingAparajay SurnamelessNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Rosa Luxemburg Finace Demand Capital SurplusDocumento25 pagineRosa Luxemburg Finace Demand Capital SurplusAparajay SurnamelessNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- SA LVI 21 SukhadeoThorat 22052021Documento7 pagineSA LVI 21 SukhadeoThorat 22052021Aparajay SurnamelessNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Diseases of Rice in Cauvery Delta Region of Tamil NaduDocumento12 pagineDiseases of Rice in Cauvery Delta Region of Tamil NaduAparajay SurnamelessNessuna valutazione finora
- 1.caste and Economic DiscriminationDocumento4 pagine1.caste and Economic DiscriminationAnurag PrabhakarNessuna valutazione finora
- Reservation and EfficiencyDocumento3 pagineReservation and EfficiencyAparajay SurnamelessNessuna valutazione finora
- (Vol LI No 8) Sukhadeo Thorat, Nitin Tagade, Ajaya K Naik-Prejudice Against Reservation Policies How and Why - Economic and Political Weekly (2016)Documento9 pagine(Vol LI No 8) Sukhadeo Thorat, Nitin Tagade, Ajaya K Naik-Prejudice Against Reservation Policies How and Why - Economic and Political Weekly (2016)Subhadeep SinhamahapatraNessuna valutazione finora
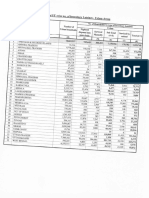
- Statewise No. of Insanitary LatrinesDocumento1 paginaStatewise No. of Insanitary LatrinesAparajay SurnamelessNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Nfhs 4 ReportDocumento666 pagineNfhs 4 ReportAparajay Surnameless100% (1)
- (The Legacy of Social Exclusion) PDFDocumento5 pagine(The Legacy of Social Exclusion) PDFAnuj GoyalNessuna valutazione finora
- Chomsky and WittgensteinDocumento3 pagineChomsky and WittgensteinAparajay SurnamelessNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hegel On Madness and TragedyDocumento30 pagineHegel On Madness and TragedyAparajay SurnamelessNessuna valutazione finora
- The Psychology of Jung in Hermann Hesse Work'sDocumento13 pagineThe Psychology of Jung in Hermann Hesse Work'sAlejandra Figueroa100% (1)
- Ethics and Genetically Modified FoodDocumento248 pagineEthics and Genetically Modified FoodAparajay SurnamelessNessuna valutazione finora
- Towards Feminist MarxismDocumento37 pagineTowards Feminist MarxismAparajay SurnamelessNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Einstein at Lincoln UniversityDocumento3 pagineEinstein at Lincoln UniversitySteven WilliamsNessuna valutazione finora
- UntitledDocumento18 pagineUntitledjake ruthNessuna valutazione finora
- 45-TQM in Indian Service Sector PDFDocumento16 pagine45-TQM in Indian Service Sector PDFsharan chakravarthyNessuna valutazione finora
- Welcome To The Falcons School For GirlsDocumento6 pagineWelcome To The Falcons School For GirlsSowmiyiaNessuna valutazione finora
- Introduction To Paid Search Advertising - TranscriptDocumento4 pagineIntroduction To Paid Search Advertising - TranscriptAnudeep KumarNessuna valutazione finora
- Gerson Lehrman GroupDocumento1 paginaGerson Lehrman GroupEla ElaNessuna valutazione finora
- Module 4 - Starting Your BusinessDocumento8 pagineModule 4 - Starting Your BusinessJHERICA SURELLNessuna valutazione finora
- Logistics Specialist NAVEDTRA 15004BDocumento970 pagineLogistics Specialist NAVEDTRA 15004Blil_ebb100% (5)
- Napoleon BonaparteDocumento1 paginaNapoleon Bonaparteyukihara_mutsukiNessuna valutazione finora
- Student Name: - : Question DetailsDocumento105 pagineStudent Name: - : Question Detailsyea okayNessuna valutazione finora
- Greek Gods & Goddesses (Gods & Goddesses of Mythology) PDFDocumento132 pagineGreek Gods & Goddesses (Gods & Goddesses of Mythology) PDFgie cadusaleNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Creative Writing PieceDocumento3 pagineCreative Writing Pieceapi-608098440Nessuna valutazione finora
- IGNOU Vs MCI High Court JudgementDocumento46 pagineIGNOU Vs MCI High Court Judgementom vermaNessuna valutazione finora
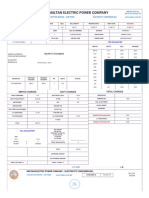
- Multan Electric Power Company: Say No To CorruptionDocumento2 pagineMultan Electric Power Company: Say No To CorruptionLearnig TechniquesNessuna valutazione finora
- Critique On The Lens of Kantian Ethics, Economic Justice and Economic Inequality With Regards To Corruption: How The Rich Get Richer and Poor Get PoorerDocumento15 pagineCritique On The Lens of Kantian Ethics, Economic Justice and Economic Inequality With Regards To Corruption: How The Rich Get Richer and Poor Get PoorerJewel Patricia MoaNessuna valutazione finora
- Judgments of Adminstrative LawDocumento22 pagineJudgments of Adminstrative Lawpunit gaurNessuna valutazione finora
- Roselie Ann A. de Guzman Bsihm3A Centro Escolar University - (Makati)Documento14 pagineRoselie Ann A. de Guzman Bsihm3A Centro Escolar University - (Makati)Cristopher Rico DelgadoNessuna valutazione finora
- Educ 203 CHAPTER 6 Lesson 1Documento13 pagineEduc 203 CHAPTER 6 Lesson 1charmen rogando100% (4)
- Frias Vs Atty. LozadaDocumento47 pagineFrias Vs Atty. Lozadamedalin1575Nessuna valutazione finora
- A Review Essay On The European GuildsDocumento11 pagineA Review Essay On The European GuildsAnonymous xDPiyENessuna valutazione finora
- PERDEV2Documento7 paginePERDEV2Riza Mae GardoseNessuna valutazione finora
- BloggingDocumento8 pagineBloggingbethNessuna valutazione finora
- WAS 101 EditedDocumento132 pagineWAS 101 EditedJateni joteNessuna valutazione finora
- Ecology Block Wall CollapseDocumento14 pagineEcology Block Wall CollapseMahbub KhanNessuna valutazione finora
- Test Bank For Global 4 4th Edition Mike PengDocumento9 pagineTest Bank For Global 4 4th Edition Mike PengPierre Wetzel100% (32)
- Viking Solid Cone Spray NozzleDocumento13 pagineViking Solid Cone Spray NozzlebalaNessuna valutazione finora
- JONES - Blues People - Negro Music in White AmericaDocumento46 pagineJONES - Blues People - Negro Music in White AmericaNatalia ZambaglioniNessuna valutazione finora
- Ground Floor Plan Second Floor Plan: Bedroom 1 T & B Service Area Closet T & BDocumento1 paginaGround Floor Plan Second Floor Plan: Bedroom 1 T & B Service Area Closet T & BAbegail Dela CruzNessuna valutazione finora
- Buyer - Source To Contracts - English - 25 Apr - v4Documento361 pagineBuyer - Source To Contracts - English - 25 Apr - v4ardiannikko0Nessuna valutazione finora
- 1ST Term J3 Business StudiesDocumento19 pagine1ST Term J3 Business Studiesoluwaseun francisNessuna valutazione finora
- Poor Economics: A Radical Rethinking of the Way to Fight Global PovertyDa EverandPoor Economics: A Radical Rethinking of the Way to Fight Global PovertyValutazione: 4.5 su 5 stelle4.5/5 (263)
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfDa EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfValutazione: 5 su 5 stelle5/5 (36)
- Workin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherDa EverandWorkin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherNessuna valutazione finora
- The Meth Lunches: Food and Longing in an American CityDa EverandThe Meth Lunches: Food and Longing in an American CityValutazione: 5 su 5 stelle5/5 (5)
- IF YOU SEE THEM: Young, Unhoused, and Alone in America.Da EverandIF YOU SEE THEM: Young, Unhoused, and Alone in America.Nessuna valutazione finora
- Hillbilly Elegy: A Memoir of a Family and Culture in CrisisDa EverandHillbilly Elegy: A Memoir of a Family and Culture in CrisisValutazione: 4 su 5 stelle4/5 (4284)