Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- World Quality Report 2019 2020Documento68 pagineWorld Quality Report 2019 2020Remco100% (1)
- Mobile Remote Deposit Capture (Public Facing Site)Documento15 pagineMobile Remote Deposit Capture (Public Facing Site)Kendra ShillingtonNessuna valutazione finora
- Jrockit Mission ControlDocumento4 pagineJrockit Mission ControlsudheerrdNessuna valutazione finora
- Stellaris Launchpad Work BookDocumento278 pagineStellaris Launchpad Work BookJulianaMarianaNessuna valutazione finora
- Unit 2Documento131 pagineUnit 2vineetNessuna valutazione finora
- Yash CANADA VISA SOP 1Documento2 pagineYash CANADA VISA SOP 1amine boudhiefNessuna valutazione finora
- Traffic Sign Detection and RecognitionDocumento4 pagineTraffic Sign Detection and RecognitionInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- C - Programv1 Global EdgeDocumento61 pagineC - Programv1 Global EdgeRajendra AcharyaNessuna valutazione finora
- Whats NewDocumento26 pagineWhats NewDucha FamiNessuna valutazione finora
- Insult Detection Using A Partitional CNN-LSTM ModelDocumento9 pagineInsult Detection Using A Partitional CNN-LSTM ModelCSIT iaesprimeNessuna valutazione finora
- Coding File InventoryDocumento10 pagineCoding File Inventorymaintenance cwaNessuna valutazione finora
- Fortigate SSLVPNDocumento69 pagineFortigate SSLVPNMauricio FloresNessuna valutazione finora
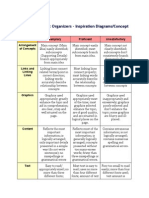
- Rubric For Graphic Organizer1Documento2 pagineRubric For Graphic Organizer1api-235993449Nessuna valutazione finora
- Backup N RecoveryDocumento16 pagineBackup N RecoveryAbraham GetachewNessuna valutazione finora
- PNGDocumento354 paginePNGMoon Din100% (2)
- UMTS RNC Product Description v1 04Documento82 pagineUMTS RNC Product Description v1 04tquanglongNessuna valutazione finora
- Hash Map Programming-Assignment-3Documento16 pagineHash Map Programming-Assignment-3Ranveer SinghaniyaNessuna valutazione finora
- Project Budget Template 22Documento11 pagineProject Budget Template 22koum juniorNessuna valutazione finora
- DEA-41T1.exam.26q: Number: DEA-41T1 Passing Score: 800 Time Limit: 120 MinDocumento9 pagineDEA-41T1.exam.26q: Number: DEA-41T1 Passing Score: 800 Time Limit: 120 MinMỹ Linh NguyễnNessuna valutazione finora
- What S New in Ezchrom Elite 3 3 2 Sp2Documento13 pagineWhat S New in Ezchrom Elite 3 3 2 Sp2David RuizNessuna valutazione finora
- Vodafone USB 4G Upgrade Guide V7.2: Huawei Technologies Co., LTDDocumento10 pagineVodafone USB 4G Upgrade Guide V7.2: Huawei Technologies Co., LTDshikitinsNessuna valutazione finora
- Aja Bridge-Ndi-3g Manual v1.7Documento95 pagineAja Bridge-Ndi-3g Manual v1.7UMcuatrocerocincoNessuna valutazione finora
- CARIS-SIPS BackscatterDocumento1 paginaCARIS-SIPS BackscatterzakariaNessuna valutazione finora
- Cambium Networks Data Sheet Network Service EdgeDocumento4 pagineCambium Networks Data Sheet Network Service EdgeGirish GowdaNessuna valutazione finora
- Window Builder TutorialDocumento7 pagineWindow Builder TutorialBertty Contreras RojasNessuna valutazione finora
- GitHub - Janpetzold - Prince2-Foundation-Summary - A Summary of The Necessary Knowledge For The PRINCE2 Foundation ExamDocumento26 pagineGitHub - Janpetzold - Prince2-Foundation-Summary - A Summary of The Necessary Knowledge For The PRINCE2 Foundation ExamSylwia Chadaj0% (1)
- GPGPU TutorialDocumento155 pagineGPGPU TutorialTiểu Đông ĐôngNessuna valutazione finora
- Sequence DetectorDocumento9 pagineSequence DetectorBHAVYANessuna valutazione finora
- US/OPS - OP1511 - FPS02.pdf: Program Name / Task Recommended FrequencyDocumento2 pagineUS/OPS - OP1511 - FPS02.pdf: Program Name / Task Recommended FrequencyRajeswarNessuna valutazione finora
- KNX 100G - Setup Guide: E G H C D FDocumento4 pagineKNX 100G - Setup Guide: E G H C D FSkrapNessuna valutazione finora