Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Nprot 2008Documento9 pagineNprot 2008AlbarbarawiNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- 2351 (2001) Anne Dell: Science, Et AlDocumento7 pagine2351 (2001) Anne Dell: Science, Et AlAlbarbarawiNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Supplemental Information Quantitative Proteomics Reveals Subset-Specific Viral Recognition in Dendritic CellsDocumento7 pagineSupplemental Information Quantitative Proteomics Reveals Subset-Specific Viral Recognition in Dendritic CellsAlbarbarawiNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Nature Protocol - Subcellular Fraction at IonDocumento7 pagineNature Protocol - Subcellular Fraction at IonAlbarbarawiNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Protein Mass SpectrometryDocumento7 pagineProtein Mass SpectrometryAlbarbarawiNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Manual SupelcoDocumento12 pagineManual Supelcogrubensam100% (3)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
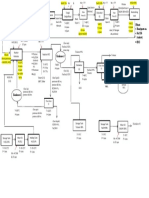
- Filtrate: Hemi/pentosan Na2SO4 (Terlarut) H2O: Filter Press 02 Filter Press 01Documento1 paginaFiltrate: Hemi/pentosan Na2SO4 (Terlarut) H2O: Filter Press 02 Filter Press 01afifahNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Acids, Alkalis and Titrations 2 QP (Paper 1)Documento12 pagineAcids, Alkalis and Titrations 2 QP (Paper 1)Josephine FuNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Exp 6 Lab ReportDocumento15 pagineExp 6 Lab ReportNur Syuhaidah100% (1)
- SBA CONCENTRATION TITRATION 40 CopiesDocumento4 pagineSBA CONCENTRATION TITRATION 40 CopiesTahpehs PhiriNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- KAU Curriculum of ChemistryDocumento47 pagineKAU Curriculum of ChemistrygogookNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Solution PHDocumento3 pagineSolution PHSanjay GuptaNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Protein WorksheetDocumento4 pagineProtein WorksheetKathleen GomezNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Development and Validation of HPLC Method For The PDFDocumento9 pagineDevelopment and Validation of HPLC Method For The PDFAlejandro Muñoz LazoNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Technical ReferenceDocumento14 pagineTechnical ReferenceMehmood AhmedNessuna valutazione finora
- Sodium SaccharineDocumento3 pagineSodium SaccharineHerdian PebiNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Analytical CalculationsDocumento45 pagineAnalytical CalculationsKanchan Kumar NayakNessuna valutazione finora
- Topics Final Exam T3 Ay2022-2023Documento3 pagineTopics Final Exam T3 Ay2022-2023barettNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- K26. Aspek Fisika Dalam BiomolekulDocumento68 pagineK26. Aspek Fisika Dalam BiomolekulFalih KepahiangNessuna valutazione finora
- GWMW - Vik MVG Ve 'V: (Acid-Base Equilibrium)Documento20 pagineGWMW - Vik MVG Ve 'V: (Acid-Base Equilibrium)Shahanaz ParvinNessuna valutazione finora
- Topic 20 Answers To ExercisesDocumento4 pagineTopic 20 Answers To ExercisesSiti NuraqidahNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Ionic Equilibrium WSDocumento20 pagineIonic Equilibrium WSVishal MNessuna valutazione finora
- BS en Iso 17294-1-2006 (2008)Documento42 pagineBS en Iso 17294-1-2006 (2008)Vassilis ZacharisNessuna valutazione finora
- A1 Ch19studyguideDocumento3 pagineA1 Ch19studyguideJana Aldour100% (2)
- Chemistry LaboratoryDocumento56 pagineChemistry LaboratoryYash KapoorNessuna valutazione finora
- Organic Chemistry 7th Edition Bruice Test BankDocumento9 pagineOrganic Chemistry 7th Edition Bruice Test BanknmNessuna valutazione finora
- Rietveld Made Easy - OverviewDocumento3 pagineRietveld Made Easy - Overviewhp2020Nessuna valutazione finora
- Introduction To CATION AnalysisDocumento18 pagineIntroduction To CATION AnalysisJen MaramionNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Jce 2007 P 0124 WDocumento25 pagineJce 2007 P 0124 WAlexaNessuna valutazione finora
- Volumetric Analysis 1Documento3 pagineVolumetric Analysis 1vijay kumarNessuna valutazione finora
- Experiment 3 2Documento6 pagineExperiment 3 2Kenth Roger A. MaquilingNessuna valutazione finora
- Chemical Equilibrium PDFDocumento51 pagineChemical Equilibrium PDFRaam KumarNessuna valutazione finora
- Analysis of Ethoxylated Fatty Amines. Comparison of Methods For The Determination of Molecular WeightDocumento11 pagineAnalysis of Ethoxylated Fatty Amines. Comparison of Methods For The Determination of Molecular Weightkent0331100% (1)
- Chem 2 Weak Base Strong Acid Lab ReportDocumento6 pagineChem 2 Weak Base Strong Acid Lab ReportMohammad Izadi100% (1)
- Chemtech ReviewerDocumento1 paginaChemtech ReviewerRicky Jay86% (7)
- Isolation of Chlorophyll and Carotenoid Pigments From SpinachDocumento4 pagineIsolation of Chlorophyll and Carotenoid Pigments From SpinachTorrez ElvisNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)