Potrebbero piacerti anche
- ANATOMY: The Shoulder Girdle Shoulder Spaces Axilla The ArmDocumento88 pagineANATOMY: The Shoulder Girdle Shoulder Spaces Axilla The ArmNur Liyana MohamadNessuna valutazione finora
- Songs of the workers: on the road, in the jungles, and in the shopsDa EverandSongs of the workers: on the road, in the jungles, and in the shopsNessuna valutazione finora
- Anatomy Physiology of Hip JointDocumento6 pagineAnatomy Physiology of Hip JointSundaraBharathiNessuna valutazione finora
- Hip Joint Anatomy - Overview, Gross AnatomyDocumento14 pagineHip Joint Anatomy - Overview, Gross AnatomyZuraedha ZamilNessuna valutazione finora
- Study Sheet - Gross Anatomy Lower - ExtremityDocumento12 pagineStudy Sheet - Gross Anatomy Lower - ExtremityMuhammad BilalNessuna valutazione finora
- Lower Limb Muscles: Muscle Origin Insertion Innervation Main ActionsDocumento6 pagineLower Limb Muscles: Muscle Origin Insertion Innervation Main ActionsJade Phoebe AjeroNessuna valutazione finora
- Joints of Lower LimbDocumento7 pagineJoints of Lower LimbjsdlzjNessuna valutazione finora
- Joints of Lower LimbDocumento55 pagineJoints of Lower LimbHanis ZahirahNessuna valutazione finora
- Upper Limb Lecture 1Documento45 pagineUpper Limb Lecture 1RAHMADANI SAFITRINessuna valutazione finora
- Radial and Median NervesDocumento33 pagineRadial and Median NervesveegeerNessuna valutazione finora
- Muscular SystemDocumento47 pagineMuscular SystemKrystal Kaye AczonNessuna valutazione finora
- Lower Limb MusclesDocumento43 pagineLower Limb MusclesJonah DelmundoNessuna valutazione finora
- Joints of The Head and Trunk - 2015-RuanDocumento30 pagineJoints of The Head and Trunk - 2015-RuanKw ChanNessuna valutazione finora
- Foot and AnkleDocumento40 pagineFoot and AnkleAhmed Salman100% (2)
- Myofascial Muscle Chains - P. Jonckheere, Et Al., (Trigger, 1998) WWDocumento308 pagineMyofascial Muscle Chains - P. Jonckheere, Et Al., (Trigger, 1998) WW1cucu0100% (6)
- Abdomen NotesDocumento66 pagineAbdomen NotesJason Toniolo0% (1)
- Human AnatomyDocumento76 pagineHuman AnatomyAlwie Afc SionNessuna valutazione finora
- Pelvis Anatomy DiplomaDocumento50 paginePelvis Anatomy DiplomaJason Toniolo100% (1)
- HeadDocumento135 pagineHeadalanNessuna valutazione finora
- S.C.H.E.M.a.T.a - Star Citizen Handy Enthusiast's Manual and Technical AssistantDocumento222 pagineS.C.H.E.M.a.T.a - Star Citizen Handy Enthusiast's Manual and Technical AssistantCesare Verzini100% (1)
- LogHorizonTRPGv0 6Documento173 pagineLogHorizonTRPGv0 6dexad50728Nessuna valutazione finora
- Thorax AnatomyDocumento34 pagineThorax AnatomyJason Toniolo100% (1)
- Three Inch Glory II RULEBOOKDocumento64 pagineThree Inch Glory II RULEBOOKmic697Nessuna valutazione finora
- Basic First Aid PDFDocumento10 pagineBasic First Aid PDFkeziahmaedavidNessuna valutazione finora
- Kami Export - Circulation 2 QPDocumento9 pagineKami Export - Circulation 2 QPKiswal AliNessuna valutazione finora
- 4 The Diagram Shows Part of The Human Digestive SystemDocumento2 pagine4 The Diagram Shows Part of The Human Digestive SystemArif01721Nessuna valutazione finora
- Surgical Instruments and Drains PDFDocumento117 pagineSurgical Instruments and Drains PDFNariska CooperNessuna valutazione finora
- Datema Order Catalogue IndexDocumento115 pagineDatema Order Catalogue IndexDanang Prayogi0% (1)
- Operating Manual Partura® Delivery Bed 140.1010.0Documento58 pagineOperating Manual Partura® Delivery Bed 140.1010.0Uno Medical Technology SANessuna valutazione finora
- Practical20Guide20To20Quantitative20Finance20Interview 604244935Documento212 paginePractical20Guide20To20Quantitative20Finance20Interview 604244935BenjaminNessuna valutazione finora
- Welcome To The JungleDocumento36 pagineWelcome To The JungleJames Marion100% (1)
- FEI Jumping Guidelines For Use of Saddlery, Equipment and DressDocumento44 pagineFEI Jumping Guidelines For Use of Saddlery, Equipment and DressAleksandra TutajNessuna valutazione finora
- Charge Pikes!: English Civil War Miniatures Rules by Wesley A. RogersDocumento35 pagineCharge Pikes!: English Civil War Miniatures Rules by Wesley A. RogersJames MurphyNessuna valutazione finora
- Chapter 58 - Anatomy of The Larynx and Tracheobronchial TreeDocumento11 pagineChapter 58 - Anatomy of The Larynx and Tracheobronchial TreeMon DominguezNessuna valutazione finora
- Valentina Ebook 8-24-17Documento45 pagineValentina Ebook 8-24-17Lee oo86% (7)
- Music in The BibleDocumento102 pagineMusic in The Biblejld4444100% (3)
- The Mask and The Sword - SZNy9tDocumento243 pagineThe Mask and The Sword - SZNy9tthhpitiNessuna valutazione finora
- Favorite IcebreakersDocumento107 pagineFavorite IcebreakersBoukharienglish100% (4)
- Seussical Bilingual Script v1Documento66 pagineSeussical Bilingual Script v1Alex ChenNessuna valutazione finora
- LI Xenos 04Documento118 pagineLI Xenos 04cielaqNessuna valutazione finora
- July 5 - Grade 14Documento2 pagineJuly 5 - Grade 14Rajindu TillakaratneNessuna valutazione finora
- Anatomy SummaryDocumento159 pagineAnatomy Summarydenisa100% (1)
- Narcisistic Families Undertand and Overcome by Taryana RochaDocumento102 pagineNarcisistic Families Undertand and Overcome by Taryana RochaCGTK Design100% (2)
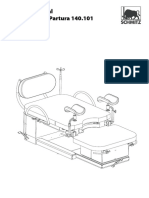
- Repair Manual Delivery Bed Partura 140.101Documento64 pagineRepair Manual Delivery Bed Partura 140.101Uno Medical Technology SANessuna valutazione finora
- Natural Sciencie 3Documento14 pagineNatural Sciencie 3Reyes ArcusaNessuna valutazione finora
- Drummingthegods-1 0Documento141 pagineDrummingthegods-1 0Cristina GiulianiNessuna valutazione finora
- Mass Effect Saga RPG (DLC - Soldiers of The Milky Way)Documento88 pagineMass Effect Saga RPG (DLC - Soldiers of The Milky Way)Eric KrausNessuna valutazione finora
- The PelvisDocumento44 pagineThe PelvisSadatHamisNessuna valutazione finora
- Worms 2 (PC Game) User ManualDocumento47 pagineWorms 2 (PC Game) User ManualrygetzNessuna valutazione finora
- Duolingo French Tips & NotesDocumento111 pagineDuolingo French Tips & NotesAnonymous EoHQjDNessuna valutazione finora
- Podiatry Note TemplatesDocumento209 paginePodiatry Note Templateszanezane27Nessuna valutazione finora
- Aftermath! - FGU4014 Magic!Documento67 pagineAftermath! - FGU4014 Magic!yoNessuna valutazione finora
- How To Make Someone Fall in Love With YouDocumento91 pagineHow To Make Someone Fall in Love With Your7zpc4bbxhNessuna valutazione finora
- AOE PPC Edition Download ManualDocumento19 pagineAOE PPC Edition Download Manual08ibaizabalNessuna valutazione finora
- Brinkwood Almanac v09 - 2Documento217 pagineBrinkwood Almanac v09 - 2Marcos InkiNessuna valutazione finora
- VI Woodwinds 1 Manual v2Documento189 pagineVI Woodwinds 1 Manual v2Nils Van der PlanckenNessuna valutazione finora
- A2 12 QuesDocumento14 pagineA2 12 QuesNaiyar IjazNessuna valutazione finora
- Playout ManualDocumento43 paginePlayout ManualAndrei AndreiNessuna valutazione finora
- Abdomen NotesDocumento66 pagineAbdomen NotesJason Toniolo0% (1)
- Pelvis Anatomy DiplomaDocumento50 paginePelvis Anatomy DiplomaJason Toniolo100% (1)
- Thorax AnatomyDocumento34 pagineThorax AnatomyJason Toniolo100% (1)
- Universal Embryology SummaryDocumento6 pagineUniversal Embryology SummaryJason TonioloNessuna valutazione finora
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocumento7 pagineSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNessuna valutazione finora
- Assignment5 - Female PelvisDocumento8 pagineAssignment5 - Female PelvisMahenurNessuna valutazione finora
- Anatomy and Physiology of Reproductive SystemDocumento93 pagineAnatomy and Physiology of Reproductive SystemMelizza Fajardo BañanoNessuna valutazione finora
- 12th Edition Brunner & Suddarth's Unit 15Documento43 pagine12th Edition Brunner & Suddarth's Unit 15colee5140% (1)
- Klales Et Al Phenice Scoring and ProbabilityDocumento11 pagineKlales Et Al Phenice Scoring and ProbabilityLIDIA ALVIZURI GOMEZNessuna valutazione finora
- 5.6 Muscle Energy Techniques For The Pelvis 167-171Documento5 pagine5.6 Muscle Energy Techniques For The Pelvis 167-171maricartiNessuna valutazione finora
- Obstetrics and Gynecology Ebook Notes PDFDocumento89 pagineObstetrics and Gynecology Ebook Notes PDFGaurav ShyamaniNessuna valutazione finora
- MusculoSkeletal SystemDocumento56 pagineMusculoSkeletal Systemmaj71% (7)
- 173 Anatomy SkeletalDocumento23 pagine173 Anatomy SkeletalChristian Phaul AsendidoNessuna valutazione finora
- The Hip Joint and Pelvic GatewaysDocumento32 pagineThe Hip Joint and Pelvic GatewaysArybaa MeerNessuna valutazione finora
- Pelvic InjuriesDocumento35 paginePelvic InjuriesJavier Saad100% (1)
- Anatomy of The CamelDocumento62 pagineAnatomy of The Cameligorgalopp100% (4)
- Pelvis 1Documento10 paginePelvis 1Nur Liyana MohamadNessuna valutazione finora
- Abdominal Stab Wound Case StudyDocumento36 pagineAbdominal Stab Wound Case StudyMean Elepaño80% (5)
- TBL 1 Limbs and SpineDocumento9 pagineTBL 1 Limbs and SpineffNessuna valutazione finora
- The Skeletal System The Skeletal System: © 2018 Pearson Education, Ltd. 1Documento16 pagineThe Skeletal System The Skeletal System: © 2018 Pearson Education, Ltd. 1lourd nabNessuna valutazione finora
- Bio Mechanics of The HipDocumento71 pagineBio Mechanics of The HipnishantsinghbmeNessuna valutazione finora
- Anatomy & Physiology of Female Reproductive System: Dr. Aida Abd El-RazekDocumento96 pagineAnatomy & Physiology of Female Reproductive System: Dr. Aida Abd El-RazekJennifer DixonNessuna valutazione finora
- Assignment5 - Female PelvisDocumento7 pagineAssignment5 - Female PelvispriyankaNessuna valutazione finora
- Model Paper 21 PrncfetDocumento13 pagineModel Paper 21 PrncfetDr-Sanjay SinghaniaNessuna valutazione finora
- Femur AP ProjectionDocumento9 pagineFemur AP ProjectionIka HarikartiNessuna valutazione finora
- Daftar Nama Penugasan Buku CatatanDocumento5 pagineDaftar Nama Penugasan Buku CatatanMuhammad Mu'adz FathurrachmanNessuna valutazione finora
- Hip DislocationDocumento67 pagineHip DislocationKJ Iza (KJ Nurshariza HPSF)Nessuna valutazione finora
- Obstetric InterventionDocumento238 pagineObstetric InterventionErmiNessuna valutazione finora
- MCN Module 3Documento9 pagineMCN Module 3Fatrick BernardinoNessuna valutazione finora
- CHAPTER TWO ANATOMY OF FEMALE PELVIS AND PhysiologyDocumento62 pagineCHAPTER TWO ANATOMY OF FEMALE PELVIS AND PhysiologyabyNessuna valutazione finora
- Gynae CompilationDocumento787 pagineGynae CompilationMajgsjqNessuna valutazione finora
- Pdfs/residency/anatomy/ Normal-Anatomy-And-Physiology-Of-The-Female-PelvisDocumento34 paginePdfs/residency/anatomy/ Normal-Anatomy-And-Physiology-Of-The-Female-PelvisMohamed FarahatNessuna valutazione finora
- Bruzek 2002 AJPADocumento12 pagineBruzek 2002 AJPAthereeseNessuna valutazione finora
- Joey: How a Blind Rescue Horse Helped Others Learn to SeeDa EverandJoey: How a Blind Rescue Horse Helped Others Learn to SeeValutazione: 5 su 5 stelle5/5 (23)
- Horse Care 101: How to Take Care of a Horse for BeginnersDa EverandHorse Care 101: How to Take Care of a Horse for BeginnersValutazione: 4 su 5 stelle4/5 (5)
- The Power of the Herd: A Nonpredatory Approach to Social Intelligence, Leadership, and InnovationDa EverandThe Power of the Herd: A Nonpredatory Approach to Social Intelligence, Leadership, and InnovationNessuna valutazione finora
- The Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenDa EverandThe Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenValutazione: 4.5 su 5 stelle4.5/5 (49)
- Speak Your Horse's Language:: Communicating with the Driving HorseDa EverandSpeak Your Horse's Language:: Communicating with the Driving HorseNessuna valutazione finora
- How Long Can a Fly Fly?: 175 Answers to Possible and Impossible Questions about AnimalsDa EverandHow Long Can a Fly Fly?: 175 Answers to Possible and Impossible Questions about AnimalsNessuna valutazione finora
- Traditional Blacksmithing: The Fine Art of Horseshoeing and Wagon MakingDa EverandTraditional Blacksmithing: The Fine Art of Horseshoeing and Wagon MakingNessuna valutazione finora
- Second-Chance Horses: True Stories of the Horses We Rescue and the Horses Who Rescue UsDa EverandSecond-Chance Horses: True Stories of the Horses We Rescue and the Horses Who Rescue UsNessuna valutazione finora
- The Everything Horse Book: Buying, riding, and caring for your equine companionDa EverandThe Everything Horse Book: Buying, riding, and caring for your equine companionValutazione: 2 su 5 stelle2/5 (1)
- Wild Horses of the Summer Sun: A Memoir of IcelandDa EverandWild Horses of the Summer Sun: A Memoir of IcelandValutazione: 3.5 su 5 stelle3.5/5 (4)
- The Winning Horseplayer: An Advanced Approach to Thoroughbred Handicapping and BettingDa EverandThe Winning Horseplayer: An Advanced Approach to Thoroughbred Handicapping and BettingNessuna valutazione finora
- Building Your Dream Horse: Charles Wilhelm's Ultimate Foundation TrainingDa EverandBuilding Your Dream Horse: Charles Wilhelm's Ultimate Foundation TrainingValutazione: 4 su 5 stelle4/5 (4)
- Lead with Your Heart: Lessons from a Life with HorsesDa EverandLead with Your Heart: Lessons from a Life with HorsesValutazione: 4 su 5 stelle4/5 (8)
- The USPC Guide to Longeing and Ground TrainingDa EverandThe USPC Guide to Longeing and Ground TrainingValutazione: 4.5 su 5 stelle4.5/5 (3)
- Project Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroDa EverandProject Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroValutazione: 5 su 5 stelle5/5 (9)
- Stable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnDa EverandStable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnValutazione: 5 su 5 stelle5/5 (4)
- Paddock Paradise: A Guide to Natural Horse BoardingDa EverandPaddock Paradise: A Guide to Natural Horse BoardingNessuna valutazione finora
- The Tao Of Horses: Exploring How Horses Guide Us on Our Spiritual PathDa EverandThe Tao Of Horses: Exploring How Horses Guide Us on Our Spiritual PathValutazione: 5 su 5 stelle5/5 (1)
- Fitness Evaluation of the HorseDa EverandFitness Evaluation of the HorseValutazione: 5 su 5 stelle5/5 (1)
- Hoof Physics: How to Recognize the Signs of Hoof DistortionDa EverandHoof Physics: How to Recognize the Signs of Hoof DistortionValutazione: 5 su 5 stelle5/5 (1)
- The Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseDa EverandThe Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseNessuna valutazione finora
- Horses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)Da EverandHorses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)Valutazione: 3.5 su 5 stelle3.5/5 (11)