Potrebbero piacerti anche
- 678 FullDocumento9 pagine678 FullDarren WilliamNessuna valutazione finora
- Intracranial TumoursDocumento42 pagineIntracranial TumoursShreyasi PatankarNessuna valutazione finora
- Review of Cystic and Solid TumorDocumento6 pagineReview of Cystic and Solid TumorAnonymous syRbQm6Nessuna valutazione finora
- Transplante CorneaDocumento5 pagineTransplante CorneaJossie TeneriaNessuna valutazione finora
- Uveal Melanoma in Saudi ArabiaDocumento2 pagineUveal Melanoma in Saudi ArabiaJohn GomezNessuna valutazione finora
- RCSD or RCCD Peripheral WITHDocumento2 pagineRCSD or RCCD Peripheral WITHEmma LiamNessuna valutazione finora
- Ovarian Tumour - V2 - Final Maruf Raza1Documento9 pagineOvarian Tumour - V2 - Final Maruf Raza1raiyanbinteazamkhanNessuna valutazione finora
- Salivary Gland Tumors: January 2016Documento19 pagineSalivary Gland Tumors: January 2016Candra HandayaniNessuna valutazione finora
- Neurosurgical Focus An Introductory Overview of Orbital TumorsDocumento9 pagineNeurosurgical Focus An Introductory Overview of Orbital Tumorsnadia emildaNessuna valutazione finora
- (SURG) 5.4b Management of Soft Tissue SarcomaDocumento6 pagine(SURG) 5.4b Management of Soft Tissue SarcomaKenneth TorresNessuna valutazione finora
- Wjoms v1 Id1009Documento4 pagineWjoms v1 Id1009Nexi anessaNessuna valutazione finora
- Salivary Gland TumorsDocumento25 pagineSalivary Gland TumorsdrpnnreddyNessuna valutazione finora
- A Sarcoma A ADocumento13 pagineA Sarcoma A AStefania CristinaNessuna valutazione finora
- Update On Dermoscopy of SpitzReed Naevi and Management Guidelines by The International Dermoscopy SocietyDocumento11 pagineUpdate On Dermoscopy of SpitzReed Naevi and Management Guidelines by The International Dermoscopy SocietyEduarda QuartinNessuna valutazione finora
- Ant Seg TumorsDocumento25 pagineAnt Seg TumorsSwati TyagiNessuna valutazione finora
- Sarcomatoid Salivary Duct Carcinoma of The Submandibular GlandDocumento6 pagineSarcomatoid Salivary Duct Carcinoma of The Submandibular GlandGermanLoopezzNessuna valutazione finora
- Metaplastic Meningioma Presenting With Anemia in A Young Boy Case Report and Review of The LiteratureDocumento5 pagineMetaplastic Meningioma Presenting With Anemia in A Young Boy Case Report and Review of The LiteratureInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Journal Ocular Surface Tumor DiagnosticDocumento22 pagineJournal Ocular Surface Tumor DiagnosticMuammar EduNessuna valutazione finora
- Controversies in The Pathophysiology and Management of HyphemaDocumento12 pagineControversies in The Pathophysiology and Management of HyphemaJoseph Chipana GutierrezNessuna valutazione finora
- Foster KennedyDocumento3 pagineFoster KennedyIsaac TellezNessuna valutazione finora
- FoncDocumento11 pagineFoncNugroho prasetyoNessuna valutazione finora
- Ijo 67 1930Documento19 pagineIjo 67 1930faraamirNessuna valutazione finora
- 10 1016@j Jviscsurg 2015 05 001 PDFDocumento8 pagine10 1016@j Jviscsurg 2015 05 001 PDFErnestine SutrisnoNessuna valutazione finora
- Curr Diag Pathol-2006-12 - Sinonasal CarcinomasDocumento14 pagineCurr Diag Pathol-2006-12 - Sinonasal Carcinomasdarmayanti ibnuNessuna valutazione finora
- Neuroepithelial Tumors of The CNS: Hemispheric Diencephalic Optic Brain Stem CerebellarDocumento4 pagineNeuroepithelial Tumors of The CNS: Hemispheric Diencephalic Optic Brain Stem CerebellarMoof06Nessuna valutazione finora
- Pleomorphic Sarcoma in Paratesticular Region: Case Report Open AccessDocumento5 paginePleomorphic Sarcoma in Paratesticular Region: Case Report Open AccessNurulDiniaPutriNessuna valutazione finora
- Histological Subtypes and Anatomical Location SWMDocumento7 pagineHistological Subtypes and Anatomical Location SWMYuwan RamjadaNessuna valutazione finora
- Case Report: Eccrine Porocarcinoma of Scalp: A Rare Case ReportDocumento4 pagineCase Report: Eccrine Porocarcinoma of Scalp: A Rare Case ReportAyuNessuna valutazione finora
- Adult Orbital Rhabdomyosarcoma Case ReportDocumento3 pagineAdult Orbital Rhabdomyosarcoma Case ReportInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Epidemiology of Childhood Cancer in "Dharmais" Cancer HospitalDocumento16 pagineEpidemiology of Childhood Cancer in "Dharmais" Cancer HospitalIndonesian Journal of CancerNessuna valutazione finora
- 170 FullDocumento6 pagine170 Fullvionica's channelNessuna valutazione finora
- Salivary Gland TumorsDocumento12 pagineSalivary Gland TumorsDurga VoraNessuna valutazione finora
- Journal Review Orbital TumourDocumento26 pagineJournal Review Orbital TumourbhartiNessuna valutazione finora
- Meta 2.1 Ocampo LibroDocumento21 pagineMeta 2.1 Ocampo LibrogermanNessuna valutazione finora
- Meta 2.1 Ocampo Libro (01-07)Documento7 pagineMeta 2.1 Ocampo Libro (01-07)germanNessuna valutazione finora
- Atypical Melanoma Mimicking A Vascular Tumor: Clinical and Dermoscopic FindingsDocumento6 pagineAtypical Melanoma Mimicking A Vascular Tumor: Clinical and Dermoscopic FindingsIJAR JOURNALNessuna valutazione finora
- Cancers: Pediatric Low-Grade GliomasDocumento18 pagineCancers: Pediatric Low-Grade GliomasbogdanneamtuNessuna valutazione finora
- Webb 2001Documento9 pagineWebb 2001kaarlaamendezNessuna valutazione finora
- Surgical Outcomes of Cerebellopontine Angle Tumors in 34 CasesDocumento11 pagineSurgical Outcomes of Cerebellopontine Angle Tumors in 34 Casesresident wiinsNessuna valutazione finora
- Medular PseudoangiosarcomaDocumento5 pagineMedular PseudoangiosarcomaUriel Benito Cabañas RodriguezNessuna valutazione finora
- Rabdo OrbitarioDocumento6 pagineRabdo OrbitarioCaballero X CaballeroNessuna valutazione finora
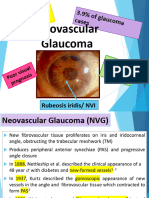
- Rana Greene Neovascular GlaucomaDocumento25 pagineRana Greene Neovascular GlaucomaGG INessuna valutazione finora
- Eye AstrocytomaDocumento5 pagineEye AstrocytomacandiddreamsNessuna valutazione finora
- Squash FinalDocumento29 pagineSquash FinalDaniel Barrios MaestreNessuna valutazione finora
- Periorbital Dermoid Cyst PDFDocumento3 paginePeriorbital Dermoid Cyst PDFRicarhdo Valentino HanafiNessuna valutazione finora
- Neoplasms Ear CanalDocumento12 pagineNeoplasms Ear CanalannaNessuna valutazione finora
- Melanome Acral: Du Diagnostic Au TraitementDocumento8 pagineMelanome Acral: Du Diagnostic Au TraitementIJAR JOURNALNessuna valutazione finora
- Thediagnosisand Managementof Scrotalmasses: Jeffrey S. Montgomery,, David A. BloomDocumento10 pagineThediagnosisand Managementof Scrotalmasses: Jeffrey S. Montgomery,, David A. BloomLyka MahrNessuna valutazione finora
- Ecr 0702Documento17 pagineEcr 0702HerelinuNessuna valutazione finora
- Patho Rapid Question ReviewDocumento22 paginePatho Rapid Question Reviewmrcsexam.iranNessuna valutazione finora
- Meningioma: Tengku Rizky Aditya, MDDocumento30 pagineMeningioma: Tengku Rizky Aditya, MDTengku Rizky AdityaNessuna valutazione finora
- Ceju 65 00148Documento4 pagineCeju 65 00148Meta SakinaNessuna valutazione finora
- DOI: 10.1515/jbcr-2015-0170: Case ReportDocumento4 pagineDOI: 10.1515/jbcr-2015-0170: Case ReporttaufikolingNessuna valutazione finora
- Extra Medullary Plasmacytoma With A Pulmonary Location Resembling Bronchial Carcinoma: A Case ReportDocumento4 pagineExtra Medullary Plasmacytoma With A Pulmonary Location Resembling Bronchial Carcinoma: A Case ReportInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Superficial Acral Fibromyxoma SAF A Case ReportDocumento4 pagineSuperficial Acral Fibromyxoma SAF A Case ReportAthenaeum Scientific PublishersNessuna valutazione finora
- PartII Salivaryglands NEWDocumento15 paginePartII Salivaryglands NEWahmedfikryNessuna valutazione finora
- Treatment of Vascular Malformations of The Mandible: A Description of 12 CasesDocumento5 pagineTreatment of Vascular Malformations of The Mandible: A Description of 12 CasesneyhaaNessuna valutazione finora
- Neuropathology: FK UisuDocumento28 pagineNeuropathology: FK UisuAnggi WahyuNessuna valutazione finora
- Epithelial-Myoepithelial Carcinoma Arising in The Accessory Parotid Gland A Case ReportDocumento4 pagineEpithelial-Myoepithelial Carcinoma Arising in The Accessory Parotid Gland A Case ReportInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Malingering and Factitious Disorder: Christopher Bass, Derick T WadeDocumento10 pagineMalingering and Factitious Disorder: Christopher Bass, Derick T WadePutri YingNessuna valutazione finora
- Factitious Disorders 2: Factitious Disorders and Malingering: Challenges For Clinical Assessment and ManagementDocumento11 pagineFactitious Disorders 2: Factitious Disorders and Malingering: Challenges For Clinical Assessment and ManagementPutri YingNessuna valutazione finora
- KDocumento8 pagineKPutri YingNessuna valutazione finora
- A Case Report On Isoniazid Induced Bullous Drug ReactionDocumento6 pagineA Case Report On Isoniazid Induced Bullous Drug ReactionPutri YingNessuna valutazione finora
- Alcohol Use Disorder Severity and Reported Reasons Not To Seek Treatment: A Cross-Sectional Study in European Primary Care PracticesDocumento10 pagineAlcohol Use Disorder Severity and Reported Reasons Not To Seek Treatment: A Cross-Sectional Study in European Primary Care PracticesPutri YingNessuna valutazione finora
- Isoniazid Induced AlopeciaDocumento2 pagineIsoniazid Induced AlopeciaPutri YingNessuna valutazione finora
- Efficacy and Acceptability of Pharmacological Treat-Ments For Depressive Disorders in Primary Care: Systematic Review and Network Meta-AnalysisDocumento11 pagineEfficacy and Acceptability of Pharmacological Treat-Ments For Depressive Disorders in Primary Care: Systematic Review and Network Meta-AnalysisPutri YingNessuna valutazione finora
- Hold I Ness 1985Documento6 pagineHold I Ness 1985Putri YingNessuna valutazione finora
- Isoniazid Induced Lupus Presenting As Oral Mucosal Ulcers With PancytopeniaDocumento3 pagineIsoniazid Induced Lupus Presenting As Oral Mucosal Ulcers With PancytopeniaPutri YingNessuna valutazione finora
- Severe Skin Rash and Liver Toxic Effects Caused by First-Line Anti-Tuberculosis Drugs: A Case ReportDocumento4 pagineSevere Skin Rash and Liver Toxic Effects Caused by First-Line Anti-Tuberculosis Drugs: A Case ReportPutri YingNessuna valutazione finora
- Ispub 11731Documento4 pagineIspub 11731Putri YingNessuna valutazione finora
- Case Report: Hypersensitivity Reaction and Tolerance Induction To EthambutolDocumento4 pagineCase Report: Hypersensitivity Reaction and Tolerance Induction To EthambutolPutri YingNessuna valutazione finora
- CCDC102B Confers Risk of Low Vision and Blindness in High MyopiaDocumento7 pagineCCDC102B Confers Risk of Low Vision and Blindness in High MyopiaPutri YingNessuna valutazione finora
- Cyclosporine Treatment of Drug-Induced Hypersensitivity SyndromeDocumento4 pagineCyclosporine Treatment of Drug-Induced Hypersensitivity SyndromePutri YingNessuna valutazione finora
- Ethionamide-Induced Pellagra: by Yashashree Gupta and Ira ShahDocumento3 pagineEthionamide-Induced Pellagra: by Yashashree Gupta and Ira ShahPutri YingNessuna valutazione finora
- Ibrt 10 I 1 P 53Documento4 pagineIbrt 10 I 1 P 53Putri YingNessuna valutazione finora
- A Case of The Drug Reaction With Eosinophilia and Systemic Symptom (DRESS) Following Isoniazid TreatmentDocumento4 pagineA Case of The Drug Reaction With Eosinophilia and Systemic Symptom (DRESS) Following Isoniazid TreatmentPutri YingNessuna valutazione finora
- Yield of Imaging Performed As Per Indian Society of Pediatric Nephrology Guidelines in Children With Urinary Tract InfectionDocumento3 pagineYield of Imaging Performed As Per Indian Society of Pediatric Nephrology Guidelines in Children With Urinary Tract InfectionPutri YingNessuna valutazione finora
- Association of Food and Drug Allergy With Anti-Tuberculosis Drug Related Hepatitis or Skin Reactions: A Case Control StudyDocumento6 pagineAssociation of Food and Drug Allergy With Anti-Tuberculosis Drug Related Hepatitis or Skin Reactions: A Case Control StudyPutri YingNessuna valutazione finora
- Urinary Tract Infections in Neonates With Unexplained Pathological Indirect Hyperbilirubinemia: Prevalence and SignificanceDocumento5 pagineUrinary Tract Infections in Neonates With Unexplained Pathological Indirect Hyperbilirubinemia: Prevalence and SignificancePutri YingNessuna valutazione finora
- Peeping Painless ProptosisDocumento3 paginePeeping Painless ProptosisPutri YingNessuna valutazione finora
- CnidariaDocumento50 pagineCnidariacalvinleow1205Nessuna valutazione finora
- T4 An Vuah ThungDocumento6 pagineT4 An Vuah ThungSaint_Dada100% (2)
- Complete Denture ManualDocumento23 pagineComplete Denture ManualCitra PurnamasariNessuna valutazione finora
- Histology of KidneyDocumento4 pagineHistology of KidneyIzzi FekratNessuna valutazione finora
- Long Quiz 1 BiologyDocumento2 pagineLong Quiz 1 BiologyNonita Caracas CubiloNessuna valutazione finora
- TM2 - K37 - Eye Disorders Due To Tropical DiseasesDocumento86 pagineTM2 - K37 - Eye Disorders Due To Tropical DiseasesedelinNessuna valutazione finora
- Pleno A Blok 22 (Abortus)Documento34 paginePleno A Blok 22 (Abortus)Jesslyn HarapanNessuna valutazione finora
- A Model of Diurnal Grazing Patterns and Herbage Intake of A Dairy Cow, Mindy Model DescriptionDocumento19 pagineA Model of Diurnal Grazing Patterns and Herbage Intake of A Dairy Cow, Mindy Model DescriptionconNessuna valutazione finora
- MenuDocumento2 pagineMenubartolopirolo22Nessuna valutazione finora
- Health Reporting: Winner - Bamuturaki Musinguzi, Daily MonitorDocumento14 pagineHealth Reporting: Winner - Bamuturaki Musinguzi, Daily MonitorAfrican Centre for Media Excellence100% (1)
- Soal TOEFLDocumento2 pagineSoal TOEFLArraya Eritha BarcelonaNessuna valutazione finora
- Hpc3 - The Menu and Its CourseDocumento3 pagineHpc3 - The Menu and Its Coursemark danielNessuna valutazione finora
- The Lost HerdDocumento16 pagineThe Lost Herddarkdel100% (2)
- Snow White and Rose RedDocumento5 pagineSnow White and Rose RedkeisyaaurelliawajidiNessuna valutazione finora
- Dog GoldendoodleDocumento8 pagineDog GoldendoodlejustasNessuna valutazione finora
- Whats The SettingDocumento2 pagineWhats The Settingapi-2428046300% (2)
- Spellcaster #7Documento70 pagineSpellcaster #7nispotulmiNessuna valutazione finora
- Writer's Effects ExerciseDocumento4 pagineWriter's Effects ExerciseeleanorNessuna valutazione finora
- "The E-Petvet Card": Marketing Management New Product Development PlanDocumento31 pagine"The E-Petvet Card": Marketing Management New Product Development PlanCharlene Gem BactadNessuna valutazione finora
- Wordlist Spelling Bee AEO 2017Documento50 pagineWordlist Spelling Bee AEO 2017Mike AndersonNessuna valutazione finora
- Standards For Blood Banks and Transfusion Services Standards For Blood Banks and Transfusion ServicesDocumento5 pagineStandards For Blood Banks and Transfusion Services Standards For Blood Banks and Transfusion Serviceslaexm95Nessuna valutazione finora
- SAMPLE of Crow Moon by Lucy H. PearceDocumento32 pagineSAMPLE of Crow Moon by Lucy H. PearceWomancraft Publishing100% (1)
- Pre Test, Grade 7: Dark ChocolateDocumento5 paginePre Test, Grade 7: Dark ChocolateJamMelchor100% (3)
- Group D SpongesDocumento3 pagineGroup D SpongesMukbsNessuna valutazione finora
- Ferlinghetti Lawrence A Coney Island of The MindDocumento48 pagineFerlinghetti Lawrence A Coney Island of The MindDengel dabbebi100% (4)
- Exercise Pamphlet PDFDocumento2 pagineExercise Pamphlet PDFBrittanyNessuna valutazione finora
- HawkDocumento5 pagineHawkhemanta saikia100% (2)
- KDM Kit 1.07Documento16 pagineKDM Kit 1.07Renato MatosNessuna valutazione finora
- Biomechanics of RPD 1Documento9 pagineBiomechanics of RPD 1Padmini ReddyNessuna valutazione finora
- Report Text TurtleDocumento6 pagineReport Text TurtleNadia Aisy-yaya100% (1)