Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Jonn Mumford - KundaliniDocumento270 pagineJonn Mumford - KundaliniRagghu RangswamyNessuna valutazione finora
- The Illustrated Canon of Chen Family TaijiquanDocumento768 pagineThe Illustrated Canon of Chen Family Taijiquanj182razor86% (7)
- The Art of Shen Ku - The Ultimate Traveler's GuideDocumento337 pagineThe Art of Shen Ku - The Ultimate Traveler's Guidemiguelfrimer97% (29)
- Tibetan Reiki by WhiteDocumento22 pagineTibetan Reiki by Whitej182razor100% (7)
- Mantra ReikiDocumento26 pagineMantra ReikiSorin100% (4)
- Erotic EmpowermentDocumento9 pagineErotic Empowermentj182razorNessuna valutazione finora
- Orb of Life by OleDocumento4 pagineOrb of Life by Olej182razor100% (3)
- Green Tara Seichim ManualDocumento25 pagineGreen Tara Seichim ManualShadow_Jedi80% (5)
- Ama Deus ReikiDocumento36 pagineAma Deus Reikij182razor100% (2)
- Violet Flame Reiki ManualDocumento30 pagineViolet Flame Reiki ManualVictoria Generao89% (63)
- Crystal Dragons ReikiDocumento36 pagineCrystal Dragons Reikij182razor100% (3)
- ©2010, by Reikiangelos Workshops. All Rights ReservedDocumento29 pagine©2010, by Reikiangelos Workshops. All Rights ReservedLiviu-George Saizescu100% (1)
- Imara ReikiDocumento9 pagineImara ReikiDaniela MaraNessuna valutazione finora
- Mastering Self AttunementsDocumento42 pagineMastering Self Attunementsj182razor67% (3)
- Kundalini 1 9 by OleDocumento11 pagineKundalini 1 9 by OleNarsingh YadavNessuna valutazione finora
- Chinese Dragon ReikiDocumento13 pagineChinese Dragon Reikij182razor100% (8)
- Armanen RunesDocumento128 pagineArmanen Runesfenrissulfir100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Problems 1Documento2 pagineProblems 1Andoy Don M.Nessuna valutazione finora
- Literature 101 Assignment: Step 1: Graphic OrganizerDocumento2 pagineLiterature 101 Assignment: Step 1: Graphic OrganizercatarinaNessuna valutazione finora
- Investigation: Present By:Shivam Ranabhat Project Title: Esport Players Recruit SystemDocumento18 pagineInvestigation: Present By:Shivam Ranabhat Project Title: Esport Players Recruit Systemjames chhetriNessuna valutazione finora
- Seventh Pay Commission ArrearsDocumento11 pagineSeventh Pay Commission Arrearssantosh bharathyNessuna valutazione finora
- A705F Schematic Circuit Diagram HALABTECHDocumento11 pagineA705F Schematic Circuit Diagram HALABTECHbcscneg0% (1)
- MS Y7 Spelling Bee Memo & List 21 22Documento9 pagineMS Y7 Spelling Bee Memo & List 21 22Muhammad Akbar SaniNessuna valutazione finora
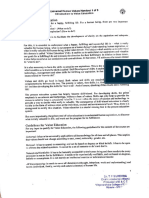
- Guidelines and Standards For External Evaluation Organisations 5th Edition v1.1Documento74 pagineGuidelines and Standards For External Evaluation Organisations 5th Edition v1.1Entrepre NurseNessuna valutazione finora
- ACFrOgDVly789-6Z8jIbi7pBoLupubEgMyOp7PczEvUguHoW3uj oR2PKzDvuhRzzkIhacYjxXRrU6iA7sHt t6MhtpZFq0t uZL2pF5Ra NNZ kmcl5w7BCQeUegKhjRhNuou88XxLodzWwbsrDocumento14 pagineACFrOgDVly789-6Z8jIbi7pBoLupubEgMyOp7PczEvUguHoW3uj oR2PKzDvuhRzzkIhacYjxXRrU6iA7sHt t6MhtpZFq0t uZL2pF5Ra NNZ kmcl5w7BCQeUegKhjRhNuou88XxLodzWwbsrJohn Steven LlorcaNessuna valutazione finora
- The Logistics of Harmonious Co-LivingDocumento73 pagineThe Logistics of Harmonious Co-LivingKripa SriramNessuna valutazione finora
- Adsa Ka SyllabusDocumento3 pagineAdsa Ka SyllabusHacker RanjanNessuna valutazione finora
- Oracle Pac 2nd KeyDocumento48 pagineOracle Pac 2nd KeyKrishna Kumar GuptaNessuna valutazione finora
- Universal Human Values NotesDocumento13 pagineUniversal Human Values NotesS RamNessuna valutazione finora
- THDP-3 Worm Gear Manual Interchangeable Single Punch Tablet PressDocumento8 pagineTHDP-3 Worm Gear Manual Interchangeable Single Punch Tablet Pressdibimrane13Nessuna valutazione finora
- Product-Oriented Learning Competencies: (Beginner)Documento4 pagineProduct-Oriented Learning Competencies: (Beginner)Kri S ELNessuna valutazione finora
- 12V140 Seris Engine Shop ManualDocumento471 pagine12V140 Seris Engine Shop ManualRaed Mahyoub100% (4)
- International Trade SyllabusDocumento3 pagineInternational Trade SyllabusDialee Flor Dael BaladjayNessuna valutazione finora
- SIP Project ProposalDocumento2 pagineSIP Project ProposalDeep SutariaNessuna valutazione finora
- Normal DistributionDocumento23 pagineNormal Distributionlemuel sardualNessuna valutazione finora
- Maya Evaluating InterfacesDocumento6 pagineMaya Evaluating InterfacesChristopher WalkerNessuna valutazione finora
- Tank Top Return Line Filter Pi 5000 Nominal Size 160 1000 According To Din 24550Documento8 pagineTank Top Return Line Filter Pi 5000 Nominal Size 160 1000 According To Din 24550Mauricio Ariel H. OrellanaNessuna valutazione finora
- Comparison of Plate Count Agar and R2A Medium For Enumeration of Heterotrophic Bacteria in Natural Mineral WaterDocumento4 pagineComparison of Plate Count Agar and R2A Medium For Enumeration of Heterotrophic Bacteria in Natural Mineral WaterSurendar KesavanNessuna valutazione finora
- Teacher Empowerment As An Important Component of Job Satisfaction A Comparative Study of Teachers Perspectives in Al Farwaniya District KuwaitDocumento24 pagineTeacher Empowerment As An Important Component of Job Satisfaction A Comparative Study of Teachers Perspectives in Al Farwaniya District KuwaitAtique RahmanNessuna valutazione finora
- Almugea or Proper FaceDocumento5 pagineAlmugea or Proper FaceValentin BadeaNessuna valutazione finora
- Symptoms and DiseasesDocumento8 pagineSymptoms and Diseaseschristy maeNessuna valutazione finora
- RH 120eDocumento8 pagineRH 120eSawadogo Gustave NapinguebsonNessuna valutazione finora
- Gaara Hiden Series Light NovelDocumento127 pagineGaara Hiden Series Light NovelartfardadNessuna valutazione finora
- Project Scheduling: Marinella A. LosaDocumento12 pagineProject Scheduling: Marinella A. LosaMarinella LosaNessuna valutazione finora
- Civil & Structural Designer'S Data Pack: Section 7: MasonryDocumento5 pagineCivil & Structural Designer'S Data Pack: Section 7: MasonryMirea Florentin0% (1)
- Catalog ITEM - Pdf4a3667894b315Documento552 pagineCatalog ITEM - Pdf4a3667894b315Domokos LeventeNessuna valutazione finora
- Mbeya University of Science and TecnologyDocumento8 pagineMbeya University of Science and TecnologyVuluwa GeorgeNessuna valutazione finora