Potrebbero piacerti anche
- Nursing Supply FinalDocumento47 pagineNursing Supply FinalAnang BudiNessuna valutazione finora
- Adverse Drug ReactionsDocumento21 pagineAdverse Drug ReactionsRohit100% (1)
- Factors Affecting Soft Tissue Around Dental ImplantsDocumento5 pagineFactors Affecting Soft Tissue Around Dental Implantsharshita parashar0% (2)
- Current Clinical Concepts in Regenerative Periodontal Therapy PDFDocumento8 pagineCurrent Clinical Concepts in Regenerative Periodontal Therapy PDFFergy Christin MaitimuNessuna valutazione finora
- TB Teaching PlanDocumento5 pagineTB Teaching PlanTrisha Fae Loyola Balagot100% (1)
- Artículo de Técnica Del Muro. G. ZucchelliDocumento10 pagineArtículo de Técnica Del Muro. G. ZucchelliBasma DerdabiNessuna valutazione finora
- Alveolar Bone Preservation in Extraction Sockets Using Non-Resorbable dPTFE Membranes: A Retrospective Non-Randomized StudyDocumento15 pagineAlveolar Bone Preservation in Extraction Sockets Using Non-Resorbable dPTFE Membranes: A Retrospective Non-Randomized StudyDiego SiqueiraNessuna valutazione finora
- International Endodontic JournalDocumento13 pagineInternational Endodontic Journalrestu dewi lestariNessuna valutazione finora
- Comparative Evaluation of Postoperative Pain and Success Rate A 2017 JournalDocumento10 pagineComparative Evaluation of Postoperative Pain and Success Rate A 2017 JournalAlbertoNessuna valutazione finora
- Comparative Biocompatibility and Osteogenic Potential of Two Bioceramic SealersDocumento6 pagineComparative Biocompatibility and Osteogenic Potential of Two Bioceramic SealerssarmientocornejoNessuna valutazione finora
- Healing of tissues in menopausal women following periodontal treatmentDocumento4 pagineHealing of tissues in menopausal women following periodontal treatmentDread NoughtNessuna valutazione finora
- Conservative Managing ofDocumento9 pagineConservative Managing ofsystematic reviewNessuna valutazione finora
- Prognosis of Dental Implants in Patients With Low Bone Density: A Systemic Review and Meta-AnalysisDocumento10 paginePrognosis of Dental Implants in Patients With Low Bone Density: A Systemic Review and Meta-AnalysisNathan LouisNessuna valutazione finora
- Guided Bone Regeneration in The Oral Cavity: A Review: Rita A. Hitti and David G. KernsDocumento13 pagineGuided Bone Regeneration in The Oral Cavity: A Review: Rita A. Hitti and David G. KernsAndi Muhammad FahruddinNessuna valutazione finora
- Art4 PDFDocumento9 pagineArt4 PDFDiana RuizNessuna valutazione finora
- Froum-Rosen-Froum TX PDFDocumento11 pagineFroum-Rosen-Froum TX PDFMark BisharaNessuna valutazione finora
- Reviving Immature Permanent Teeth: A Case Report On Regenerative Endodontic Treatment As A Retreatment OptionDocumento3 pagineReviving Immature Permanent Teeth: A Case Report On Regenerative Endodontic Treatment As A Retreatment OptionInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Comparative Biocompatibility and Osteogenic Potential of Two Bioceramic SealersDocumento6 pagineComparative Biocompatibility and Osteogenic Potential of Two Bioceramic SealersPaulina ÁlvarezNessuna valutazione finora
- Intentional Replantation TechniquesDocumento8 pagineIntentional Replantation Techniquessoho1303Nessuna valutazione finora
- Scope of Endodontics: Regenerative Endodontics: AAE Position StatementDocumento3 pagineScope of Endodontics: Regenerative Endodontics: AAE Position StatementPuneet ChahalNessuna valutazione finora
- The International Journal of Periodontics & Restorative DentistryDocumento7 pagineThe International Journal of Periodontics & Restorative DentistryFrancisco VargasNessuna valutazione finora
- Evaluación de La Recuperación de La Sensibilidad Pulpar en Dientes Necróticos Maduros Mediante Una Técnica de Revascularización Modificada Con Fibrina Rica en PlaquetaDocumento8 pagineEvaluación de La Recuperación de La Sensibilidad Pulpar en Dientes Necróticos Maduros Mediante Una Técnica de Revascularización Modificada Con Fibrina Rica en PlaquetacatalinaNessuna valutazione finora
- Ferrarotti Et Al. Journal of Clinical Periodontology (2018)Documento10 pagineFerrarotti Et Al. Journal of Clinical Periodontology (2018)Jose Luis Bladco MorenoNessuna valutazione finora
- Biocompatibility-Of-Root-Filling-Pastes-Used-In-Primary TeethDocumento12 pagineBiocompatibility-Of-Root-Filling-Pastes-Used-In-Primary TeethRista LewiyonahNessuna valutazione finora
- Journal of Periodontology - 2019 - Kim - Effect of Gingival Phenotype On The Maintenance of Periodontal Health An AmericanDocumento28 pagineJournal of Periodontology - 2019 - Kim - Effect of Gingival Phenotype On The Maintenance of Periodontal Health An AmericanLEONARDO ALBERTO CRESPIN ZEPEDANessuna valutazione finora
- Toxicity Potential of Denture Adhesives: A Scoping Review: SystematicDocumento6 pagineToxicity Potential of Denture Adhesives: A Scoping Review: SystematicDg TistryNessuna valutazione finora
- (2003 Kan) Dimensions of Peri-Implant Mucosa An Evaluation of Maxillary Anterior Single Implants in HumansDocumento7 pagine(2003 Kan) Dimensions of Peri-Implant Mucosa An Evaluation of Maxillary Anterior Single Implants in Humansyena1010100% (1)
- 27 de Oct - Histologic Evaluation of Human Intrabony Periodontal Defects Treated With Deproteinized Bovine Bone Mineral in Combination With OrthodonticDocumento10 pagine27 de Oct - Histologic Evaluation of Human Intrabony Periodontal Defects Treated With Deproteinized Bovine Bone Mineral in Combination With OrthodonticLaura Andrea Agudelo WilchesNessuna valutazione finora
- Autologus Fibroblast InjectionsDocumento14 pagineAutologus Fibroblast InjectionsDr. DeeptiNessuna valutazione finora
- Odontoblast-Like Differentiation and Mineral FormaDocumento11 pagineOdontoblast-Like Differentiation and Mineral Formajuanesteban1890Nessuna valutazione finora
- Rasperini 2013Documento9 pagineRasperini 2013Alexa LoyaNessuna valutazione finora
- RegenerativeEndodontics AReviewofCurrentStatusandaCallforAction PDFDocumento14 pagineRegenerativeEndodontics AReviewofCurrentStatusandaCallforAction PDFVijithNessuna valutazione finora
- Lesion Sterilization and Tissue Repair Therapy (LSTR) of Necrotic Primary Molars: Case ReportDocumento4 pagineLesion Sterilization and Tissue Repair Therapy (LSTR) of Necrotic Primary Molars: Case ReportOmar CoronelNessuna valutazione finora
- Periodontal Regeneration in Vital and Nonvital Teeth - A Clinical StudyDocumento28 paginePeriodontal Regeneration in Vital and Nonvital Teeth - A Clinical Studyneetika guptaNessuna valutazione finora
- Case SeriesDocumento3 pagineCase SeriesDr. DeeptiNessuna valutazione finora
- CTG Histologic EvaluationDocumento7 pagineCTG Histologic EvaluationDr. DeeptiNessuna valutazione finora
- Classification of Facial Peri-Implant Soft Tissue Zucchelli 2019 ColDocumento9 pagineClassification of Facial Peri-Implant Soft Tissue Zucchelli 2019 ColSebastián BernalNessuna valutazione finora
- Journal of Oral Biology and Craniofacial ResearchDocumento9 pagineJournal of Oral Biology and Craniofacial ResearchCyber MagicNessuna valutazione finora
- The Influence of Cortical Bone Perforation On Guided Bone Regeneration in HumansDocumento6 pagineThe Influence of Cortical Bone Perforation On Guided Bone Regeneration in Humanspin.to.teethNessuna valutazione finora
- Biological Width Preservation in Surgical Crown LengtheningDocumento7 pagineBiological Width Preservation in Surgical Crown LengtheningAna OrtizNessuna valutazione finora
- Surgical Management of Periapical Lesion Inmaxillary Incisorswith Combined Bone Graft and Platelet - Rich Fibrin: A Case ReportDocumento5 pagineSurgical Management of Periapical Lesion Inmaxillary Incisorswith Combined Bone Graft and Platelet - Rich Fibrin: A Case ReportTMDCH JournalNessuna valutazione finora
- Clin Adv Periodontics - 2023 - Mallappa - Novel Biomaterial Advanced Platelet Rich Fibrin Plus Block For Multiple GingivalDocumento7 pagineClin Adv Periodontics - 2023 - Mallappa - Novel Biomaterial Advanced Platelet Rich Fibrin Plus Block For Multiple GingivalNikit DixitNessuna valutazione finora
- Outcome of Revascularization Procedure A Retrospective Case Series PDFDocumento8 pagineOutcome of Revascularization Procedure A Retrospective Case Series PDF吳國豪Nessuna valutazione finora
- CTZDocumento7 pagineCTZLeo ValdesNessuna valutazione finora
- 6789.9!-:/.! . !?2@80ab!c! .@8.D!Documento13 pagine6789.9!-:/.! . !?2@80ab!c! .@8.D!Gonçalo Gomes SanchesNessuna valutazione finora
- Surgical Reconstruction of Interdental PDocumento11 pagineSurgical Reconstruction of Interdental PMaria Jose GodoyNessuna valutazione finora
- Desantana 2010Documento8 pagineDesantana 2010javier cifuentesNessuna valutazione finora
- JensenDocumento19 pagineJensencarol colmenaresNessuna valutazione finora
- Utility of PDL Progenitors For in Vivo Tissue RegenerationDocumento15 pagineUtility of PDL Progenitors For in Vivo Tissue RegenerationVirgi AgustiaNessuna valutazione finora
- Jced 13 E935Documento6 pagineJced 13 E935Marwa Wagih ElboraeyNessuna valutazione finora
- An Evidence-Based Review of The Efficacy of Treatment Approaches For Immature Permanent Teeth With Pulp NecrosisDocumento6 pagineAn Evidence-Based Review of The Efficacy of Treatment Approaches For Immature Permanent Teeth With Pulp NecrosisAlina AlexandraNessuna valutazione finora
- Reduced Need For Alveolar Bone Grafting by Presurgical Orthopedics and Pimary GingivoperiosteoplastyDocumento4 pagineReduced Need For Alveolar Bone Grafting by Presurgical Orthopedics and Pimary GingivoperiosteoplastynoraveNessuna valutazione finora
- JR PEDO (Pulpectomy)Documento4 pagineJR PEDO (Pulpectomy)FitriNanditaNessuna valutazione finora
- Holtzclaw2013 PDFDocumento7 pagineHoltzclaw2013 PDFpallav GanataNessuna valutazione finora
- 203 PDFDocumento8 pagine203 PDFJambul Wak Wak WakNessuna valutazione finora
- Retention and Stability: A Review of The LiteratureDocumento8 pagineRetention and Stability: A Review of The LiteratureLanaNessuna valutazione finora
- Subperiostial Minimally Invasive Aesthetic Ridge Augmentation Technique (SMART)Documento10 pagineSubperiostial Minimally Invasive Aesthetic Ridge Augmentation Technique (SMART)Pat TellezNessuna valutazione finora
- Preservation and Augmentation of Molar Extraction Sites Affected by Severe Bone Defect Due To Advanced Periodontitis A Prospective Clinical TrialDocumento12 paginePreservation and Augmentation of Molar Extraction Sites Affected by Severe Bone Defect Due To Advanced Periodontitis A Prospective Clinical TrialBagis Emre GulNessuna valutazione finora
- Journal Homepage: - : IntroductionDocumento9 pagineJournal Homepage: - : IntroductionIJAR JOURNALNessuna valutazione finora
- Jcpe 12206 PDFDocumento17 pagineJcpe 12206 PDFrozh rasulNessuna valutazione finora
- Jcpe 12206 PDFDocumento17 pagineJcpe 12206 PDFrozh rasulNessuna valutazione finora
- Soft Tissue Wound Healing Around Teeth and Dental ImplantsDocumento17 pagineSoft Tissue Wound Healing Around Teeth and Dental ImplantsDavid CastañedaNessuna valutazione finora
- Graftless Solutions for the Edentulous PatientDa EverandGraftless Solutions for the Edentulous PatientSaj JivrajNessuna valutazione finora
- Implantes Bueno PDFDocumento9 pagineImplantes Bueno PDFPosgrado Periodoncia2017Nessuna valutazione finora
- Viruses: Are They Really Culprits For Periodontal Disease? A Critical ReviewDocumento9 pagineViruses: Are They Really Culprits For Periodontal Disease? A Critical ReviewPosgrado Periodoncia2017Nessuna valutazione finora
- Viruses: Are They Really Culprits For Periodontal Disease? A Critical ReviewDocumento9 pagineViruses: Are They Really Culprits For Periodontal Disease? A Critical ReviewPosgrado Periodoncia2017Nessuna valutazione finora
- Rocchietta2018 Aumento de RobordeDocumento15 pagineRocchietta2018 Aumento de RobordePosgrado Periodoncia2017Nessuna valutazione finora
- My RoutineDocumento1 paginaMy RoutinePosgrado Periodoncia2017Nessuna valutazione finora
- Johanna Morocho YourselfDocumento2 pagineJohanna Morocho YourselfPosgrado Periodoncia2017Nessuna valutazione finora
- Comparative and Superlative PracticeDocumento6 pagineComparative and Superlative PracticeQhristhiam KnsNessuna valutazione finora
- Johanna Morocho FamilyDocumento1 paginaJohanna Morocho FamilyPosgrado Periodoncia2017Nessuna valutazione finora
- JOHANNA MOROCHO YourselfDocumento1 paginaJOHANNA MOROCHO YourselfPosgrado Periodoncia2017Nessuna valutazione finora
- Money WorksheetDocumento4 pagineMoney WorksheetPosgrado Periodoncia2017Nessuna valutazione finora
- (Ejercicios Inglés) PDFDocumento6 pagine(Ejercicios Inglés) PDFWen03Nessuna valutazione finora
- Money WorksheetDocumento4 pagineMoney WorksheetPosgrado Periodoncia2017Nessuna valutazione finora
- JOHANNA MOROCHO YourselfDocumento1 paginaJOHANNA MOROCHO YourselfPosgrado Periodoncia2017Nessuna valutazione finora
- My RoutineDocumento1 paginaMy RoutinePosgrado Periodoncia2017Nessuna valutazione finora
- Nombre: Diego Ulloa Materia: English Fecha: 16/10/2018: 1.-Are The Sentences True or FalseDocumento2 pagineNombre: Diego Ulloa Materia: English Fecha: 16/10/2018: 1.-Are The Sentences True or FalsePosgrado Periodoncia2017Nessuna valutazione finora
- Majzoub2014 PDFDocumento20 pagineMajzoub2014 PDFPosgrado Periodoncia2017Nessuna valutazione finora
- Implantes Bueno PDFDocumento9 pagineImplantes Bueno PDFPosgrado Periodoncia2017Nessuna valutazione finora
- Johanna Morocho FamilyDocumento1 paginaJohanna Morocho FamilyPosgrado Periodoncia2017Nessuna valutazione finora
- Mardas2011bueno Dos MaterilaesDocumento8 pagineMardas2011bueno Dos MaterilaesPosgrado Periodoncia2017Nessuna valutazione finora
- 10 1111@j 1600-0501 2008 01606 XDocumento6 pagine10 1111@j 1600-0501 2008 01606 XPosgrado Periodoncia2017Nessuna valutazione finora
- Toloue2012 Bueno Compracion Entre Liofilizado y CalcioDocumento9 pagineToloue2012 Bueno Compracion Entre Liofilizado y CalcioPosgrado Periodoncia2017Nessuna valutazione finora
- Burkhardt 2015Documento12 pagineBurkhardt 2015Posgrado Periodoncia2017Nessuna valutazione finora
- 4678 9130 1 SMDocumento6 pagine4678 9130 1 SMPosgrado Periodoncia2017Nessuna valutazione finora
- Hydroxylapatite Alloplastic: Graft of Osseous DefectsDocumento11 pagineHydroxylapatite Alloplastic: Graft of Osseous DefectsPosgrado Periodoncia2017Nessuna valutazione finora
- BiossDocumento10 pagineBiossPosgrado Periodoncia2017Nessuna valutazione finora
- Antimicrobianos en PeriodonciaDocumento14 pagineAntimicrobianos en PeriodonciaPosgrado Periodoncia2017Nessuna valutazione finora
- 026.araujo & Lindhe JCP 2005Documento7 pagine026.araujo & Lindhe JCP 2005Posgrado Periodoncia2017Nessuna valutazione finora
- Periodontal Disease in PregnancyDocumento19 paginePeriodontal Disease in PregnancyPosgrado Periodoncia2017Nessuna valutazione finora
- Jepsen 2017Documento9 pagineJepsen 2017amarNessuna valutazione finora
- Cervical Checks in Labor ExplainedDocumento17 pagineCervical Checks in Labor ExplainedClaire Anne PunsalanNessuna valutazione finora
- Food & Nutrient Intervention - Specific CVCBDocumento52 pagineFood & Nutrient Intervention - Specific CVCBSiti Ika FitrasyahNessuna valutazione finora
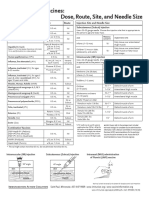
- Injection Site and Needle Size Vaccine Dose RouteDocumento1 paginaInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaNessuna valutazione finora
- Bwdi DR, Chemist&Stp Final ListDocumento226 pagineBwdi DR, Chemist&Stp Final ListzaheerbcNessuna valutazione finora
- Unit Proposal PresentationDocumento29 pagineUnit Proposal PresentationRachel CortezNessuna valutazione finora
- 2441-3300 Kneehab Phy Brochure 2r16Documento2 pagine2441-3300 Kneehab Phy Brochure 2r16MVP Marketing and DesignNessuna valutazione finora
- D-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: ThyrocareDocumento1 paginaD-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: ThyrocareKaran BaglaNessuna valutazione finora
- Mapeh 4Documento4 pagineMapeh 4Joanna Mae ArmasNessuna valutazione finora
- Urinary Tract InfectionDocumento2 pagineUrinary Tract InfectionAnonymous KillerNessuna valutazione finora
- 397 251079 1 10 20211231Documento7 pagine397 251079 1 10 20211231ariaNessuna valutazione finora
- DR Moshiri - Class II Correction by Leveraging Molar Rotation - 2Documento4 pagineDR Moshiri - Class II Correction by Leveraging Molar Rotation - 2Enea NastriNessuna valutazione finora
- Honey Promotes Better Healing Than Silver Sulfadiazine for BurnsDocumento8 pagineHoney Promotes Better Healing Than Silver Sulfadiazine for BurnsFEBRIA RAMADONANessuna valutazione finora
- Medigroup Proposal For ICU BedsDocumento13 pagineMedigroup Proposal For ICU Bedsmohyeb padamshiNessuna valutazione finora
- HospitalAdministration 2Documento13 pagineHospitalAdministration 2JairAntonAtuncarNessuna valutazione finora
- Disaster Associated Health IssuesDocumento29 pagineDisaster Associated Health Issuesmeshack mbalaNessuna valutazione finora
- PPT-cigarette SQUID GAME TEMPLATEDocumento26 paginePPT-cigarette SQUID GAME TEMPLATERuby Ann TerolNessuna valutazione finora
- References: Points Weight Lecture Actual HoursDocumento8 pagineReferences: Points Weight Lecture Actual HoursAlyssa SanchezNessuna valutazione finora
- Pros and Cons of Continuing Nursing EducationDocumento14 paginePros and Cons of Continuing Nursing EducationstanleyNessuna valutazione finora
- Bizmatics-Job OpeningDocumento2 pagineBizmatics-Job OpeningDrGirish ManeraoNessuna valutazione finora
- DACUM Competency Profile For Hemodialysis TechnicianDocumento5 pagineDACUM Competency Profile For Hemodialysis Technicianmanishbabu100% (1)
- CSL AssignmentDocumento2 pagineCSL AssignmentMuhammad QubaisNessuna valutazione finora
- Vaccines For Corona Virus Project-1Documento28 pagineVaccines For Corona Virus Project-1Ananya PuhanNessuna valutazione finora
- Occlusal Variations For Reconstructing The Natural DentitionDocumento5 pagineOcclusal Variations For Reconstructing The Natural DentitionPablo Gutiérrez Da VeneziaNessuna valutazione finora
- Ayurvedic Doctors in ChennaiDocumento1 paginaAyurvedic Doctors in ChennaiAyur IllamNessuna valutazione finora
- Measuring Disease Occurrence and Causal EffectsDocumento4 pagineMeasuring Disease Occurrence and Causal EffectsTrần Khải VănNessuna valutazione finora
- Indonesia Hires OK PDFDocumento94 pagineIndonesia Hires OK PDFikaNessuna valutazione finora
- Khat Factsheet - 020914 PDFDocumento2 pagineKhat Factsheet - 020914 PDFMohammedOumerNessuna valutazione finora