Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Risk Adjustment Coding PDFDocumento38 pagineRisk Adjustment Coding PDFGordana Puzovic100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Rope NegotiationDocumento4 pagineRope NegotiationTH x TH100% (1)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- A Mindfulness Intervention For Children With Autism Spectrum DisorderDocumento155 pagineA Mindfulness Intervention For Children With Autism Spectrum Disorderclaughlinsr4721Nessuna valutazione finora
- Blood Cells and Its Types With FunctionsDocumento5 pagineBlood Cells and Its Types With Functionskaleb16_2Nessuna valutazione finora
- OrthosisDocumento35 pagineOrthosissinghmenkaNessuna valutazione finora
- Reiki 1 ManualDocumento11 pagineReiki 1 Manualbelgarath2013100% (1)
- The Chemical ImbalanceDocumento70 pagineThe Chemical ImbalancebredabredaNessuna valutazione finora
- Kriya For Balancing The ChakrasDocumento5 pagineKriya For Balancing The ChakrasFedra Fox Cubeddu100% (2)
- Gross Anatomy and Cell Biology of The Lower Urinary Tract: Committee 1Documento66 pagineGross Anatomy and Cell Biology of The Lower Urinary Tract: Committee 1Gordana PuzovicNessuna valutazione finora
- The Spleen1Documento49 pagineThe Spleen1786waqar786Nessuna valutazione finora
- Primary Tracheal Tumors: Review of 37 CasesDocumento4 paginePrimary Tracheal Tumors: Review of 37 CasesGordana PuzovicNessuna valutazione finora
- Renal Cell CarcinomaDocumento70 pagineRenal Cell CarcinomaIsabel ReyNessuna valutazione finora
- Computed Tomography in The Diagnosis of Subcapsular and Perirenal HematomaDocumento6 pagineComputed Tomography in The Diagnosis of Subcapsular and Perirenal HematomaGordana PuzovicNessuna valutazione finora
- Accuracy of Computed Tomography in Small Bowel ObstructionDocumento3 pagineAccuracy of Computed Tomography in Small Bowel ObstructionGordana PuzovicNessuna valutazione finora
- About Lung Cancer: Overview and TypesDocumento13 pagineAbout Lung Cancer: Overview and TypesGordana PuzovicNessuna valutazione finora
- Transient Hepatic Perfusion Differences (THAD/THID) - What? When? Where?Documento35 pagineTransient Hepatic Perfusion Differences (THAD/THID) - What? When? Where?Gordana PuzovicNessuna valutazione finora
- Ho0113 Wu1Documento6 pagineHo0113 Wu1Gordana PuzovicNessuna valutazione finora
- Recurrent Pyogenic Cholangitis: From Imaging To InterventionDocumento8 pagineRecurrent Pyogenic Cholangitis: From Imaging To InterventionGordana PuzovicNessuna valutazione finora
- PIIS1556086416335158Documento12 paginePIIS1556086416335158Gordana PuzovicNessuna valutazione finora
- 1240approach To Pulmonary Nodules - 4Documento18 pagine1240approach To Pulmonary Nodules - 4Gordana PuzovicNessuna valutazione finora
- Spontaneous Ruptured Intercostal and Lumber Artery in Type 1 NeurofibromatosisDocumento15 pagineSpontaneous Ruptured Intercostal and Lumber Artery in Type 1 NeurofibromatosisGordana PuzovicNessuna valutazione finora
- InTech-Advances Bone MetastasesDocumento16 pagineInTech-Advances Bone MetastasesGordana PuzovicNessuna valutazione finora
- Sjogren's Syndrome, Vasculitis, and Cryoglobulinaemia Associated With (Kappa) Paraprotein With Rheumatoid ActivityDocumento3 pagineSjogren's Syndrome, Vasculitis, and Cryoglobulinaemia Associated With (Kappa) Paraprotein With Rheumatoid ActivityGordana PuzovicNessuna valutazione finora
- Role of Triple Phase Computed Tomography Findings For Evaluation of Hepatic LesionsDocumento8 pagineRole of Triple Phase Computed Tomography Findings For Evaluation of Hepatic LesionsGordana PuzovicNessuna valutazione finora
- Prevalence of Solid Tumors in Incidentally Detected Homogeneous Renal Masses Measuring 20 HU On Portal Venous Phase CTDocumento5 paginePrevalence of Solid Tumors in Incidentally Detected Homogeneous Renal Masses Measuring 20 HU On Portal Venous Phase CTGordana PuzovicNessuna valutazione finora
- Guidance on Evaluating and Treating UTIs and ASBDocumento14 pagineGuidance on Evaluating and Treating UTIs and ASBJohn Vincent Dy OcampoNessuna valutazione finora
- Early Onset Pneumonia Likely Caused Stonewall Jackson's DeathDocumento3 pagineEarly Onset Pneumonia Likely Caused Stonewall Jackson's DeathGordana PuzovicNessuna valutazione finora
- Review On Pancreatic Steatosis Detection by Imaging ModalitiesDocumento10 pagineReview On Pancreatic Steatosis Detection by Imaging ModalitiesGordana PuzovicNessuna valutazione finora
- Imaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Documento10 pagineImaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Gordana PuzovicNessuna valutazione finora
- Journal of Acute Disease: Study On The Relationship of Acute Ketosis Intoxication and Type 2 Diabetes MellitusDocumento5 pagineJournal of Acute Disease: Study On The Relationship of Acute Ketosis Intoxication and Type 2 Diabetes MellitusGordana PuzovicNessuna valutazione finora
- US and CT Findings in The Diagnosis of Tuberculous PeritonitisDocumento5 pagineUS and CT Findings in The Diagnosis of Tuberculous PeritonitisGordana PuzovicNessuna valutazione finora
- Acute Pancreatitis With Normal Amylase and LipaseDocumento1 paginaAcute Pancreatitis With Normal Amylase and LipaseGordana PuzovicNessuna valutazione finora
- Imaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Documento10 pagineImaging in Acute Renal Infection: BJU International (2000), 86 Suppl. 1, 70 79Gordana PuzovicNessuna valutazione finora
- Infection and Immunity-1971-Eudy-269.fullDocumento5 pagineInfection and Immunity-1971-Eudy-269.fullGordana PuzovicNessuna valutazione finora
- Early Onset Pneumonia Likely Caused Stonewall Jackson's DeathDocumento3 pagineEarly Onset Pneumonia Likely Caused Stonewall Jackson's DeathGordana PuzovicNessuna valutazione finora
- The Role of HRCT in Post-Traumatic Hypoxemia: Poster No.: Congress: Type: AuthorsDocumento51 pagineThe Role of HRCT in Post-Traumatic Hypoxemia: Poster No.: Congress: Type: AuthorsGordana PuzovicNessuna valutazione finora
- PIIS000349751101188XDocumento7 paginePIIS000349751101188XGordana PuzovicNessuna valutazione finora
- Click Here Click Here To View Optimized Website For Mobile DevicesDocumento4 pagineClick Here Click Here To View Optimized Website For Mobile DevicesFirman SalamNessuna valutazione finora
- Vitamins Are Organic Compounds Required in The Diet in Small Quantities To Perform Biological FunctionsDocumento70 pagineVitamins Are Organic Compounds Required in The Diet in Small Quantities To Perform Biological FunctionsRose LiteNessuna valutazione finora
- CCMP 2020 Batch Cardiovascular MCQsDocumento2 pagineCCMP 2020 Batch Cardiovascular MCQsharshad patelNessuna valutazione finora
- Thyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Documento11 pagineThyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Vaishnavi SheteNessuna valutazione finora
- PhobiasDocumento10 paginePhobiasapi-276690632Nessuna valutazione finora
- Medical Certificate Guidelines June 2012Documento3 pagineMedical Certificate Guidelines June 2012wudthipanNessuna valutazione finora
- Occupational Therapy Rehabilitation Paraplegic PatientDocumento7 pagineOccupational Therapy Rehabilitation Paraplegic PatientAlina PasăreNessuna valutazione finora
- Don't Steal My Mind!: Extractive Introjection in Supervision and TreatmentDocumento2 pagineDon't Steal My Mind!: Extractive Introjection in Supervision and TreatmentMatthiasBeierNessuna valutazione finora
- Science Blood TransfusionsDocumento10 pagineScience Blood Transfusionsapi-237866019Nessuna valutazione finora
- Giant Skin TagDocumento2 pagineGiant Skin Tagshf.mxlikNessuna valutazione finora
- Expansion Screw Activation Guidelines PDFDocumento1 paginaExpansion Screw Activation Guidelines PDFOsama SayedahmedNessuna valutazione finora
- Science 5Documento81 pagineScience 5Michael Joseph Santos100% (2)
- Diatermo MB 122 and MB 160 Mono-Bipolar: Cautery & ElectrosurgeryDocumento13 pagineDiatermo MB 122 and MB 160 Mono-Bipolar: Cautery & ElectrosurgeryDani Daniela100% (1)
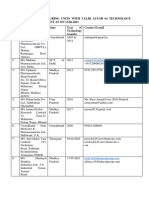
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Documento5 pagineList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesNessuna valutazione finora
- Sage Char-Lee ResumeDocumento2 pagineSage Char-Lee Resumeapi-510197139Nessuna valutazione finora
- Staph and Strep Lab Report BMS 501Documento2 pagineStaph and Strep Lab Report BMS 501aruiz93Nessuna valutazione finora
- EFN - PPTX 3Documento9 pagineEFN - PPTX 3Suheni Khotimah IndrianiNessuna valutazione finora
- Ayushman Bharat - KailashDocumento11 pagineAyushman Bharat - KailashKailash NagarNessuna valutazione finora
- Wallen Et Al-2006-Australian Occupational Therapy JournalDocumento1 paginaWallen Et Al-2006-Australian Occupational Therapy Journal胡知行Nessuna valutazione finora
- Clabsi TeamDocumento20 pagineClabsi Teamapi-344209032100% (1)
- NephrologyDocumento5 pagineNephrologyPooja NalluriNessuna valutazione finora
- Navidas-Case StudyDocumento5 pagineNavidas-Case StudyFran LanNessuna valutazione finora
- Jamnagar Thesis 2004Documento12 pagineJamnagar Thesis 2004Swagath NNessuna valutazione finora