Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- How To Become A Good Speaker: Kai-Fu Lee Corporate Vice President Microsoft CorporationDocumento63 pagineHow To Become A Good Speaker: Kai-Fu Lee Corporate Vice President Microsoft CorporationwyndinkNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Book of Bible Answers (Volume 1) - by Doug-BatchelorDocumento138 pagineBook of Bible Answers (Volume 1) - by Doug-BatchelorAdventist_Truth100% (3)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- AG C O L: Uide To Ommon RAL EsionsDocumento46 pagineAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanNessuna valutazione finora
- EFFECTS OF VOLCANIC ERUPTION - PPSXDocumento19 pagineEFFECTS OF VOLCANIC ERUPTION - PPSXMyla Balingit AdiNessuna valutazione finora
- Yes Bank FinalDocumento107 pagineYes Bank FinalDrMehul JoshiNessuna valutazione finora
- B2 First For Schools 4, Test 4 Answer Key, Reading and Use of EnglishDocumento7 pagineB2 First For Schools 4, Test 4 Answer Key, Reading and Use of EnglishAlejandro Iglesias Peón0% (1)
- Ameloblastoma: A Clinical Review and Trends in ManagementDocumento13 pagineAmeloblastoma: A Clinical Review and Trends in ManagementEzza RiezaNessuna valutazione finora
- PPTDocumento29 paginePPTwyndinkNessuna valutazione finora
- A Me Lob Last Om ADocumento5 pagineA Me Lob Last Om AandiyoyomdNessuna valutazione finora
- ICDDocumento24 pagineICDwyndinkNessuna valutazione finora
- Asa Ora PDFDocumento8 pagineAsa Ora PDFwyndinkNessuna valutazione finora
- Garp Chapter16Documento5 pagineGarp Chapter16gerawenceNessuna valutazione finora
- Iatrogenic Displacement of Impacted Mandibular Third Molar Into The Pterygomandibular Space 2247 2452.1000563Documento4 pagineIatrogenic Displacement of Impacted Mandibular Third Molar Into The Pterygomandibular Space 2247 2452.1000563wyndinkNessuna valutazione finora
- Exfoliative CheilitisDocumento2 pagineExfoliative CheilitiswyndinkNessuna valutazione finora
- 8 - Precast Concrete Structures-Students PDFDocumento17 pagine8 - Precast Concrete Structures-Students PDFsitehabNessuna valutazione finora
- Esab Ok 55 (3.2 MM)Documento1 paginaEsab Ok 55 (3.2 MM)DHANEESH VELLILAPULLINessuna valutazione finora
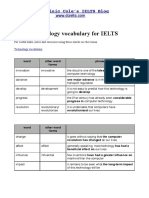
- Technology VocabularyDocumento3 pagineTechnology VocabularyChixo GalaxyNessuna valutazione finora
- Review Questions UAPGADocumento28 pagineReview Questions UAPGAkarenNessuna valutazione finora
- Honda Bikes and ScootersDocumento6 pagineHonda Bikes and ScootersShamrjit AgrahariNessuna valutazione finora
- LLM01v5 0Documento12 pagineLLM01v5 0Alan LeungNessuna valutazione finora
- D 5431 - 93 Rdu0mzetotmDocumento4 pagineD 5431 - 93 Rdu0mzetotmJuanNessuna valutazione finora
- Nuitration in Human 3Documento2 pagineNuitration in Human 3Usman AmeenNessuna valutazione finora
- Zbus and Symmetrical Fault AnalysisDocumento20 pagineZbus and Symmetrical Fault Analysishj203800Nessuna valutazione finora
- MantrasDocumento45 pagineMantrasharibhakta100% (1)
- 4g Frequency BandsDocumento5 pagine4g Frequency BandsaorukoNessuna valutazione finora
- Coronary Stents: Current StatusDocumento42 pagineCoronary Stents: Current StatusMANSI SALUNKENessuna valutazione finora
- Fish CheeksDocumento4 pagineFish Cheekshafsah aminNessuna valutazione finora
- GTE LAB MANUAL Ver 4 - 1Documento135 pagineGTE LAB MANUAL Ver 4 - 1akhilaNessuna valutazione finora
- Rider's Manual: BMW MotorradDocumento136 pagineRider's Manual: BMW MotorradAlex Quintana100% (1)
- Case IH Farmall B - Brochure - 0717Documento7 pagineCase IH Farmall B - Brochure - 0717nadeemmohamed555Nessuna valutazione finora
- Lecture For ClassDocumento97 pagineLecture For ClassRITHWIK DINESHNessuna valutazione finora
- Nature Generator (Emtech Concept Paper)Documento3 pagineNature Generator (Emtech Concept Paper)Min SugaNessuna valutazione finora
- MEC Threads ChartDocumento12 pagineMEC Threads ChartenricoNessuna valutazione finora
- Chemical Engineering Refresher CourseDocumento7 pagineChemical Engineering Refresher CourseAstra BeckettNessuna valutazione finora
- PC-FT 403: Lecture (1) byDocumento21 paginePC-FT 403: Lecture (1) byFT 19 Suparno DasNessuna valutazione finora
- 0900-9914 I1 201012 PDFDocumento132 pagine0900-9914 I1 201012 PDFIvan Arjona50% (2)
- Jurnal Praktikum Dasar-Dasar Pemisahan Kimia Pembuatan Membran Polysulfon (PSF)Documento9 pagineJurnal Praktikum Dasar-Dasar Pemisahan Kimia Pembuatan Membran Polysulfon (PSF)Rizki AuNessuna valutazione finora
- Updated CBRN - Guideline - Final - Dec 16 - 2021Documento110 pagineUpdated CBRN - Guideline - Final - Dec 16 - 2021Mohammed AbdillahiNessuna valutazione finora
- A Better World - Volume 5Documento146 pagineA Better World - Volume 5Zainuddin BusuNessuna valutazione finora
- Biology: Higher Tier Paper 1HDocumento28 pagineBiology: Higher Tier Paper 1HkaruneshnNessuna valutazione finora