Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- TEE in Congenital Heart DiseaseDocumento249 pagineTEE in Congenital Heart DiseaseAdriana VasilicaNessuna valutazione finora
- Echocardiography in TAVI ProcedureDocumento26 pagineEchocardiography in TAVI ProcedurejshNessuna valutazione finora
- Peripartum CardiomyopathyDocumento18 paginePeripartum CardiomyopathyMJ WesleyNessuna valutazione finora
- Ecg Mcqs - Aippg ForumDocumento19 pagineEcg Mcqs - Aippg Forumbmhsh100% (1)
- JSS PDFDocumento28 pagineJSS PDFabhinandanNessuna valutazione finora
- Congenital Heart DefectsDocumento19 pagineCongenital Heart DefectsNader Smadi67% (3)
- Cardiac DysrhythmiasDocumento6 pagineCardiac DysrhythmiasJeffrey Viernes100% (1)
- Survival Analysis, Part 3: Cox Regression: Statistics and Research DesignDocumento2 pagineSurvival Analysis, Part 3: Cox Regression: Statistics and Research DesignGloria KartikaNessuna valutazione finora
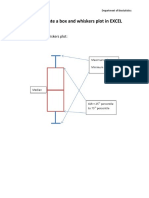
- How To Create A Box and Whiskers Plot in EXCELDocumento9 pagineHow To Create A Box and Whiskers Plot in EXCELGloria KartikaNessuna valutazione finora
- Insertion of An Intra-Aortic Balloon Catheter: PurposeDocumento4 pagineInsertion of An Intra-Aortic Balloon Catheter: PurposeGloria KartikaNessuna valutazione finora
- Contoh Surat SponsorDocumento1 paginaContoh Surat SponsorGloria KartikaNessuna valutazione finora
- MC GowanDocumento13 pagineMC GowanGloria KartikaNessuna valutazione finora
- When Not To Stop A Clinical Trial.23490736Documento4 pagineWhen Not To Stop A Clinical Trial.23490736Gloria KartikaNessuna valutazione finora
- Prevalensi Ventricular HypertrophyDocumento8 paginePrevalensi Ventricular HypertrophyGloria KartikaNessuna valutazione finora
- Cardiology Board Review - Carlquist - PT. 1 PDFDocumento40 pagineCardiology Board Review - Carlquist - PT. 1 PDFGloria KartikaNessuna valutazione finora
- CLN 66 01 107 PDFDocumento5 pagineCLN 66 01 107 PDFGloria KartikaNessuna valutazione finora
- WHO LadderDocumento2 pagineWHO LaddertelorkodokNessuna valutazione finora
- 6.21.10 Rose-Jones Board ReviewDocumento50 pagine6.21.10 Rose-Jones Board ReviewGloria KartikaNessuna valutazione finora
- 24 Newsletter Hypertension and ArrhythmiaDocumento2 pagine24 Newsletter Hypertension and ArrhythmiaGloria KartikaNessuna valutazione finora
- WHO Blindness Action An 2014-2019Documento28 pagineWHO Blindness Action An 2014-2019Gloria KartikaNessuna valutazione finora
- Vision2020 ReportDocumento97 pagineVision2020 ReportAdelaida Castro NavarreteNessuna valutazione finora
- CH 06Documento11 pagineCH 06kavitasibalNessuna valutazione finora
- WHO Clinical Management 0f Avian InfluenzaDocumento83 pagineWHO Clinical Management 0f Avian InfluenzaGloria KartikaNessuna valutazione finora
- Clinical Management 07Documento22 pagineClinical Management 07Fauzi SatriaNessuna valutazione finora
- Staining and Tooth DiscolorationDocumento14 pagineStaining and Tooth DiscolorationGloria KartikaNessuna valutazione finora
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Documento17 pagineKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNessuna valutazione finora
- Degeneratif Copy 2Documento7 pagineDegeneratif Copy 2Gloria KartikaNessuna valutazione finora
- Infeksi Marginalis NadaDocumento48 pagineInfeksi Marginalis NadaGloria KartikaNessuna valutazione finora
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Documento17 pagineKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNessuna valutazione finora
- Hypertension: H.) or May Be Associated With Other Diseases - Dorland'sDocumento1 paginaHypertension: H.) or May Be Associated With Other Diseases - Dorland'sGloria KartikaNessuna valutazione finora
- Exam #4 Study Blueprint 2019Documento2 pagineExam #4 Study Blueprint 2019Stephanie DeeNessuna valutazione finora
- Acute and Chronic Heart FailureDocumento61 pagineAcute and Chronic Heart FailureigohNessuna valutazione finora
- 1 s2.0 S136184152200130X MainDocumento19 pagine1 s2.0 S136184152200130X MainLaura StanciulescuNessuna valutazione finora
- 6 Ab 2Documento3 pagine6 Ab 2Erko100% (1)
- High Risk Consent For PCIDocumento1 paginaHigh Risk Consent For PCISree Sowjanya PatibandlaNessuna valutazione finora
- Heart Rhythm Interpretation ECG Strips 2019Documento21 pagineHeart Rhythm Interpretation ECG Strips 2019daniel situngkirNessuna valutazione finora
- Atrial FibrilasiDocumento5 pagineAtrial FibrilasiAviation MedicineNessuna valutazione finora
- Atrial FlutterDocumento2 pagineAtrial FlutterDhiaNessuna valutazione finora
- The American Journal of Cardiology Vol 107 Issue 4 February 2011Documento153 pagineThe American Journal of Cardiology Vol 107 Issue 4 February 2011ppappi12Nessuna valutazione finora
- Automated Contrast Injectors For AngiogrDocumento6 pagineAutomated Contrast Injectors For AngiogrAditya MadhavpeddiNessuna valutazione finora
- Dilated CardiomyopathyDocumento16 pagineDilated CardiomyopathyRosemarie Manatad TerioNessuna valutazione finora
- Tadeusiewicz Ubiquitous Cardiology - Emerging Wireless Telemedical Applications 2009Documento430 pagineTadeusiewicz Ubiquitous Cardiology - Emerging Wireless Telemedical Applications 2009roxanabluebeeNessuna valutazione finora
- Heart Sound .Mid Systolic Click-Mitral ProlapseDocumento2 pagineHeart Sound .Mid Systolic Click-Mitral ProlapseTeti AndriNessuna valutazione finora
- Cor PulmonaleDocumento22 pagineCor Pulmonalenatijahtun istiqomahNessuna valutazione finora
- ACS NSTEMI Clinical PathwayDocumento3 pagineACS NSTEMI Clinical PathwayXtiaRNessuna valutazione finora
- Ocroteala Ionut Lucian Holter Pus Ieri 22.08.2023Documento17 pagineOcroteala Ionut Lucian Holter Pus Ieri 22.08.2023Lototheone LotoNessuna valutazione finora
- Minutes For 267th Registration Board MeetingDocumento417 pagineMinutes For 267th Registration Board MeetingAnum IrfanNessuna valutazione finora
- History of Palpitation: Editing LinkDocumento6 pagineHistory of Palpitation: Editing LinkTouseef Ur RehmanNessuna valutazione finora
- ReferralDocumento1 paginaReferralmanasabhavaniNessuna valutazione finora
- Type of PacemakerDocumento26 pagineType of PacemakerMohammad AlmuhaiminNessuna valutazione finora
- Biomarkeri IccDocumento11 pagineBiomarkeri IccMihai GRIGORENessuna valutazione finora
- MRCPCH 1: Essential Questions in Paediatrics: Second EditionDocumento14 pagineMRCPCH 1: Essential Questions in Paediatrics: Second EditionHijazi HamadassNessuna valutazione finora