Potrebbero piacerti anche
- HenyaDocumento6 pagineHenyaKunnithi Sameunjai100% (1)
- Interpretation of Arterial Blood Gases (ABGs)Documento6 pagineInterpretation of Arterial Blood Gases (ABGs)afalfitraNessuna valutazione finora
- PandPofCC (8th Edition)Documento629 paginePandPofCC (8th Edition)Carlos Alberto CaicedoNessuna valutazione finora
- ISO 9001:2015 Explained, Fourth Edition GuideDocumento3 pagineISO 9001:2015 Explained, Fourth Edition GuideiresendizNessuna valutazione finora
- Exp 8 - GPG - D12B - 74 PDFDocumento4 pagineExp 8 - GPG - D12B - 74 PDFPRATIKSHA WADIBHASMENessuna valutazione finora
- PROF ED 10-ACTIVITY #1 (Chapter 1)Documento4 paginePROF ED 10-ACTIVITY #1 (Chapter 1)Nizelle Arevalo100% (1)
- TheEconomist 2023 04 01Documento297 pagineTheEconomist 2023 04 01Sh FNessuna valutazione finora
- Bank NIFTY Components and WeightageDocumento2 pagineBank NIFTY Components and WeightageUptrend0% (2)
- Colloidal Silver A Simple Homemade RemedyDocumento9 pagineColloidal Silver A Simple Homemade RemedyGCarrington96Nessuna valutazione finora
- CS Marvin RobeyDocumento7 pagineCS Marvin RobeySandra HarrisNessuna valutazione finora
- CHM271 - Chapter 7 - Colloid - Surface ChemistryDocumento45 pagineCHM271 - Chapter 7 - Colloid - Surface Chemistryhidayahtul adhaNessuna valutazione finora
- The Electrochemical Detection and Characterization of Silver Nanoparticles in Aqueous Solution PDFDocumento3 pagineThe Electrochemical Detection and Characterization of Silver Nanoparticles in Aqueous Solution PDFNayarik HerreraNessuna valutazione finora
- Purificación de Agua Con NanoparticulasDocumento91 paginePurificación de Agua Con NanoparticulaspedrojrsNessuna valutazione finora
- Colloidal Silver Medical Treatment RediscoveredDocumento4 pagineColloidal Silver Medical Treatment RediscoveredVince MiltonNessuna valutazione finora
- Silver-Based Polymeric Nanocomposites As Antimicrobial Coatings For Biomedical ApplicationsDocumento57 pagineSilver-Based Polymeric Nanocomposites As Antimicrobial Coatings For Biomedical ApplicationsDimas PradhasumitraNessuna valutazione finora
- PA600 Dopamine V2.6Documento54 paginePA600 Dopamine V2.6Định YpkNessuna valutazione finora
- AgDocumento9 pagineAgnureen92Nessuna valutazione finora
- Microbial Production of NanoparticlesDocumento11 pagineMicrobial Production of NanoparticlesnadiafarhanaNessuna valutazione finora
- MioPocket ReadmeDocumento27 pagineMioPocket ReadmeMon CeleronNessuna valutazione finora
- Electro Merge??Documento621 pagineElectro Merge??Sadaf MasoodNessuna valutazione finora
- Redox ReactionsDocumento8 pagineRedox ReactionsAbhayNessuna valutazione finora
- Antibacterial Medicines Obtained by Using The Silver NanoparticlesDocumento3 pagineAntibacterial Medicines Obtained by Using The Silver NanoparticlesdropsyNessuna valutazione finora
- Circuit ElectrinicDocumento2 pagineCircuit ElectrinicfamtaluNessuna valutazione finora
- AgNP Silver - Nanoparticles - Synthesized - by - in - V 2 PDFDocumento13 pagineAgNP Silver - Nanoparticles - Synthesized - by - in - V 2 PDFyousra bibaNessuna valutazione finora
- W02 Intermediate RDocumento67 pagineW02 Intermediate RLee MaryNessuna valutazione finora
- Result Prediction Using Weka: An Effort by - Shlok Tibrewal (14bit0088) Siddarth Nyati (14bit0074)Documento11 pagineResult Prediction Using Weka: An Effort by - Shlok Tibrewal (14bit0088) Siddarth Nyati (14bit0074)Siddarth NyatiNessuna valutazione finora
- A Review On Electrochemical Technologies For Water DisinfectionDocumento18 pagineA Review On Electrochemical Technologies For Water DisinfectionArun Siddarth100% (3)
- Synthesis of Silver Nanoparticles by Using Sodium BorohydrideDocumento5 pagineSynthesis of Silver Nanoparticles by Using Sodium BorohydrideGil SalazarNessuna valutazione finora
- Colloidal Silver Fabrication Using The Spark Discharge System and PDFDocumento5 pagineColloidal Silver Fabrication Using The Spark Discharge System and PDFWilton Carlos SilvaNessuna valutazione finora
- LM317L 3-Terminal Adjustable Regulator: FeaturesDocumento25 pagineLM317L 3-Terminal Adjustable Regulator: FeaturespaulpuscasuNessuna valutazione finora
- Galvanic CurrentDocumento26 pagineGalvanic CurrentRana M ArslanNessuna valutazione finora
- MioPocket Old Skins ReadmeDocumento4 pagineMioPocket Old Skins ReadmedankobanankoNessuna valutazione finora
- Relay Basics and DIYDocumento6 pagineRelay Basics and DIYJunior ElimeelogodavejuniorNessuna valutazione finora
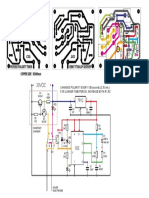
- Peverse Polarity Timer CSG: CHANGES POLARITY EVERY 130 Seconds (2,10 Min.) For Longer Time Period, Increase Both R1, R2Documento1 paginaPeverse Polarity Timer CSG: CHANGES POLARITY EVERY 130 Seconds (2,10 Min.) For Longer Time Period, Increase Both R1, R2Carlos ChaflaNessuna valutazione finora
- Building A Perf-Board Defib TesterDocumento7 pagineBuilding A Perf-Board Defib TesterElectrónica BiomédicaNessuna valutazione finora
- Application of Electrolyzed Water For Improving Pork Meat QualityDocumento7 pagineApplication of Electrolyzed Water For Improving Pork Meat QualityAnyelo MurilloNessuna valutazione finora
- TDCS GerätDocumento18 pagineTDCS GerätPeter Benedikt WeberNessuna valutazione finora
- Silver ManualDocumento94 pagineSilver ManualOmar MahmoudNessuna valutazione finora
- German Dataset TasksDocumento6 pagineGerman Dataset TasksPrateek SinghNessuna valutazione finora
- Plan 8 CS Generator PDFDocumento3 paginePlan 8 CS Generator PDFWansys UnoNessuna valutazione finora
- Redox and DisinfectionDocumento41 pagineRedox and DisinfectionKanchanNessuna valutazione finora
- Control Relay Using IR SensorDocumento5 pagineControl Relay Using IR Sensorsmartxdigital marketNessuna valutazione finora
- Medicinal Properties of Moringa Oleifera PDFDocumento7 pagineMedicinal Properties of Moringa Oleifera PDFsufijinnNessuna valutazione finora
- First Year Experiment 1 - 4Documento20 pagineFirst Year Experiment 1 - 442 Neha TikoneNessuna valutazione finora
- Chlorination of Natural Waters: Hocl CL H 0 H CLDocumento5 pagineChlorination of Natural Waters: Hocl CL H 0 H CLmuratNessuna valutazione finora
- Proteins PDFDocumento20 pagineProteins PDFDOMADO EBTISHAMNessuna valutazione finora
- Sample Meal Plan Low-Carb Diet TextDocumento2 pagineSample Meal Plan Low-Carb Diet TextJan FoxNessuna valutazione finora
- MioPocket ChangelogDocumento59 pagineMioPocket ChangelogMaría José AntúnezNessuna valutazione finora
- Development and Validation of A Miniature Programmable TDCS DeviceDocumento8 pagineDevelopment and Validation of A Miniature Programmable TDCS DevicenetoNessuna valutazione finora
- Transcranial Direct Current Stimulation Improves CDocumento13 pagineTranscranial Direct Current Stimulation Improves CCarolina Robledo CastroNessuna valutazione finora
- Faraday's Law Lab Web VersionDocumento10 pagineFaraday's Law Lab Web Versionv9mpir5Nessuna valutazione finora
- Adam1992 Hypochlorous Acid Decomposition in The PH 5-8 RegionDocumento8 pagineAdam1992 Hypochlorous Acid Decomposition in The PH 5-8 RegionGregorio ValeroNessuna valutazione finora
- Use of Coconut OilDocumento5 pagineUse of Coconut OilRakeshKumarNessuna valutazione finora
- Ag BulletDocumento7 pagineAg BulletdevendrakphyNessuna valutazione finora
- 25 Amazing Uses of Coconut OilDocumento4 pagine25 Amazing Uses of Coconut OilalanladdNessuna valutazione finora
- Electrolysis Process ExplainedDocumento4 pagineElectrolysis Process ExplainedRiddhiSolankiNessuna valutazione finora
- SILVER Nanoparticles PDFDocumento342 pagineSILVER Nanoparticles PDFFERNANDO JOSE NOVAESNessuna valutazione finora
- Thermodynamics of Ag CL H, O, Ag BR H, ODocumento9 pagineThermodynamics of Ag CL H, O, Ag BR H, Oहरिओम हरीNessuna valutazione finora
- Atopic Dermatitis and Skin Microbiome Ne PDFDocumento6 pagineAtopic Dermatitis and Skin Microbiome Ne PDFSmaranda ADNessuna valutazione finora
- MonteCarlito v1 10-2Documento9 pagineMonteCarlito v1 10-2MarkNessuna valutazione finora
- Automatic Hand Sanitizer Using IRDocumento6 pagineAutomatic Hand Sanitizer Using IRsmartxdigital marketNessuna valutazione finora
- Desbloqueio Magellan e Instalação iGO8 Guia Passo-a-passoDocumento2 pagineDesbloqueio Magellan e Instalação iGO8 Guia Passo-a-passokdlao1969Nessuna valutazione finora
- FM11 CH 07 Mini CaseDocumento12 pagineFM11 CH 07 Mini CaseMariam Sharif100% (2)
- The Use of Iodine As An Antiseptic AgentDocumento5 pagineThe Use of Iodine As An Antiseptic AgentABDO ELJANessuna valutazione finora
- How Iodine Kills Single Cellular OrganismsDocumento6 pagineHow Iodine Kills Single Cellular OrganismstonerangerNessuna valutazione finora
- Povidone Iodine Use in Hand Disinfectionskin Preparation and Antiseptic IrrigationDocumento12 paginePovidone Iodine Use in Hand Disinfectionskin Preparation and Antiseptic Irrigationpendekar bodohNessuna valutazione finora
- Review Article: The Role of Iodine in Antisepsis and Wound Management: A ReappraisalDocumento7 pagineReview Article: The Role of Iodine in Antisepsis and Wound Management: A ReappraisalRosdiana Elizabeth SiburianNessuna valutazione finora
- Iodine Revisited: Rose A CooperDocumento14 pagineIodine Revisited: Rose A CooperelsadwihermiatiNessuna valutazione finora
- Penyakit Nasofaring Dan Orofaring. Jakarta: Penerbit Buku Kedokteran EGC. 1997. PGDocumento1 paginaPenyakit Nasofaring Dan Orofaring. Jakarta: Penerbit Buku Kedokteran EGC. 1997. PGsafiraNessuna valutazione finora
- JOURDING Covid and EnchepalitisDocumento24 pagineJOURDING Covid and EnchepalitissafiraNessuna valutazione finora
- Iron and Folic Acid Supplementation Adherence Among Pregnant Women Attending Antenatal Care in North Wollo Zone Northern Ethiopia: Institution Based Cross-Sectional StudyDocumento9 pagineIron and Folic Acid Supplementation Adherence Among Pregnant Women Attending Antenatal Care in North Wollo Zone Northern Ethiopia: Institution Based Cross-Sectional StudysafiraNessuna valutazione finora
- Caspian J - V4n1p1-Fa-DikonversiDocumento7 pagineCaspian J - V4n1p1-Fa-DikonversisafiraNessuna valutazione finora
- JournalDocumento11 pagineJournalsafiraNessuna valutazione finora
- Journal ZincDocumento12 pagineJournal ZincsafiraNessuna valutazione finora
- Growth Chart CDCDocumento18 pagineGrowth Chart CDCsafiraNessuna valutazione finora
- (Q1) Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in The New York City AreaDocumento15 pagine(Q1) Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in The New York City AreasafiraNessuna valutazione finora
- (Q1) The Effect of Age On Mortality in Patients With COVID-19 A Meta-Analysis With 611,583 SubjectsDocumento4 pagine(Q1) The Effect of Age On Mortality in Patients With COVID-19 A Meta-Analysis With 611,583 SubjectssafiraNessuna valutazione finora
- JournalDocumento11 pagineJournalsafiraNessuna valutazione finora
- Risk Factors of Critical & Mortal COVID-19 Cases - A Systematic Literature Review and Meta-Analysis PDFDocumento11 pagineRisk Factors of Critical & Mortal COVID-19 Cases - A Systematic Literature Review and Meta-Analysis PDFinnaNessuna valutazione finora
- MikrografiaDocumento7 pagineMikrografiasafiraNessuna valutazione finora
- (Q1) Epidemiological, Socio-Demographic andDocumento18 pagine(Q1) Epidemiological, Socio-Demographic andsafiraNessuna valutazione finora
- Level B CDocumento14 pagineLevel B CsafiraNessuna valutazione finora
- 3Documento5 pagine3safiraNessuna valutazione finora
- JournalDocumento11 pagineJournalsafiraNessuna valutazione finora
- Fibroblast On Incised Wound Healing Process in White Male Rats (Rattus Norvegicus Strain Wistar) - Thesis, Faculty of Medicine University ofDocumento1 paginaFibroblast On Incised Wound Healing Process in White Male Rats (Rattus Norvegicus Strain Wistar) - Thesis, Faculty of Medicine University ofsafiraNessuna valutazione finora
- Jurnal CovidDocumento5 pagineJurnal CovidsafiraNessuna valutazione finora
- DD Syrigomyelia - Ventriculus Dorsalis MyelomalaciaDocumento1 paginaDD Syrigomyelia - Ventriculus Dorsalis MyelomalaciasafiraNessuna valutazione finora
- Diagnosis KetDocumento4 pagineDiagnosis KetsafiraNessuna valutazione finora
- Differential Diagnosis in Jaw LessionsDocumento15 pagineDifferential Diagnosis in Jaw LessionssafiraNessuna valutazione finora
- Parkinson Disease & Other Movement Disorders: Cherian Abraham Karunapuzha, M.DDocumento40 pagineParkinson Disease & Other Movement Disorders: Cherian Abraham Karunapuzha, M.DsafiraNessuna valutazione finora
- JournalDocumento6 pagineJournalsafiraNessuna valutazione finora
- A ReviewDocumento19 pagineA ReviewsafiraNessuna valutazione finora
- Family ApgarDocumento6 pagineFamily ApgarunjyilNessuna valutazione finora
- Presentation-Package-2015 16x9 ENDocumento12 paginePresentation-Package-2015 16x9 ENFrank Asto PocomuchaNessuna valutazione finora
- The Role of Bifidobacterium Lactis B94 Plus InulinDocumento7 pagineThe Role of Bifidobacterium Lactis B94 Plus InulinsafiraNessuna valutazione finora
- Draf Sistem Rujukan DKIDocumento8 pagineDraf Sistem Rujukan DKIsafiraNessuna valutazione finora
- Patau Syndrome: Journal of Neuropsychiatry February 2007Documento3 paginePatau Syndrome: Journal of Neuropsychiatry February 2007safiraNessuna valutazione finora
- Fibroblast On Incised Wound Healing Process in White Male Rats (Rattus Norvegicus Strain Wistar) - Thesis, Faculty of Medicine University ofDocumento1 paginaFibroblast On Incised Wound Healing Process in White Male Rats (Rattus Norvegicus Strain Wistar) - Thesis, Faculty of Medicine University ofsafiraNessuna valutazione finora
- STAT455 Assignment 1 - Part ADocumento2 pagineSTAT455 Assignment 1 - Part AAndyNessuna valutazione finora
- GATE ECE 2006 Actual PaperDocumento33 pagineGATE ECE 2006 Actual Paperkibrom atsbhaNessuna valutazione finora
- Propiedades Grado 50 A572Documento2 paginePropiedades Grado 50 A572daniel moreno jassoNessuna valutazione finora
- Circular Flow of Process 4 Stages Powerpoint Slides TemplatesDocumento9 pagineCircular Flow of Process 4 Stages Powerpoint Slides TemplatesAryan JainNessuna valutazione finora
- Inventory Control Review of LiteratureDocumento8 pagineInventory Control Review of Literatureaehupavkg100% (1)
- TWP10Documento100 pagineTWP10ed9481Nessuna valutazione finora
- Why Genentech Is 1Documento7 pagineWhy Genentech Is 1panmongolsNessuna valutazione finora
- Nursing Care Management of a Client with Multiple Medical ConditionsDocumento25 pagineNursing Care Management of a Client with Multiple Medical ConditionsDeannNessuna valutazione finora
- EIN CP 575 - 2Documento2 pagineEIN CP 575 - 2minhdang03062017Nessuna valutazione finora
- Petty Cash Vouchers:: Accountability Accounted ForDocumento3 paginePetty Cash Vouchers:: Accountability Accounted ForCrizhae OconNessuna valutazione finora
- Electronics Ecommerce Website: 1) Background/ Problem StatementDocumento7 pagineElectronics Ecommerce Website: 1) Background/ Problem StatementdesalegnNessuna valutazione finora
- Tech Data: Vultrex Production & Drilling CompoundsDocumento2 pagineTech Data: Vultrex Production & Drilling CompoundsJeremias UtreraNessuna valutazione finora
- Book Networks An Introduction by Mark NewmanDocumento394 pagineBook Networks An Introduction by Mark NewmanKhondokar Al MominNessuna valutazione finora
- Cushman Wakefield - PDS India Capability Profile.Documento37 pagineCushman Wakefield - PDS India Capability Profile.nafis haiderNessuna valutazione finora
- Prof Ram Charan Awards Brochure2020 PDFDocumento5 pagineProf Ram Charan Awards Brochure2020 PDFSubindu HalderNessuna valutazione finora
- Planning A Real Estate ProjectDocumento81 paginePlanning A Real Estate ProjectHaile SilasieNessuna valutazione finora
- AFNOR IPTDS BrochureDocumento1 paginaAFNOR IPTDS Brochurebdiaconu20048672Nessuna valutazione finora
- STAT100 Fall19 Test 2 ANSWERS Practice Problems PDFDocumento23 pagineSTAT100 Fall19 Test 2 ANSWERS Practice Problems PDFabutiNessuna valutazione finora
- Striedter - 2015 - Evolution of The Hippocampus in Reptiles and BirdsDocumento22 pagineStriedter - 2015 - Evolution of The Hippocampus in Reptiles and BirdsOsny SillasNessuna valutazione finora
- Towards A Human Resource Development Ontology Combining Competence Management and Technology-Enhanced Workplace LearningDocumento21 pagineTowards A Human Resource Development Ontology Combining Competence Management and Technology-Enhanced Workplace LearningTommy SiddiqNessuna valutazione finora
- GMWIN SoftwareDocumento1 paginaGMWIN SoftwareĐào Đình NamNessuna valutazione finora
- To Introduce BgjgjgmyselfDocumento2 pagineTo Introduce Bgjgjgmyselflikith333Nessuna valutazione finora